Emergency Chest Pain Center: A Novel Approach to Reduce Door to Balloon Time
Marwa A. Sabe, Frank J. Kaeberlein, Sharif A. Sabe, Allyson Kelly, Tracy Summerfield, Ahmed A. Sabe

TL;DR
A new approach placing a catheterization lab in the emergency department reduced treatment time and mortality for heart attack patients.
Contribution
Introducing an emergency department-based catheterization lab to reduce door-to-balloon time for STEMI patients.
Findings
ED catheterization lab patients had significantly shorter door-to-balloon times (54 vs 83 minutes).
ED catheterization lab patients had lower 30-day, 1-year, and 10-year mortality rates.
ED catheterization lab implementation is a feasible strategy for improving STEMI outcomes.
Abstract
Percutaneous coronary intervention is the preferred treatment for acute ST-segment elevation myocardial infarction (STEMI), and shorter door-to-balloon time (D2B) is associated with lower mortality. We implemented a catheterization laboratory within the emergency department (ED) as a novel strategy to reduce D2B. The purpose of this paper was to compare D2B and mortality in STEMI patients presenting to ED vs standard catheterization labs at a community hospital. We prospectively reviewed consecutive patients presenting with STEMI to our institution between 1998 and 2011 and treated with primary percutaneous coronary intervention. The primary endpoints were D2B and time to death. A multivariable linear regression model was used to assess the relationship between catheterization lab location and D2B. The relationship between D2B and mortality was examined using a Cox proportional…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
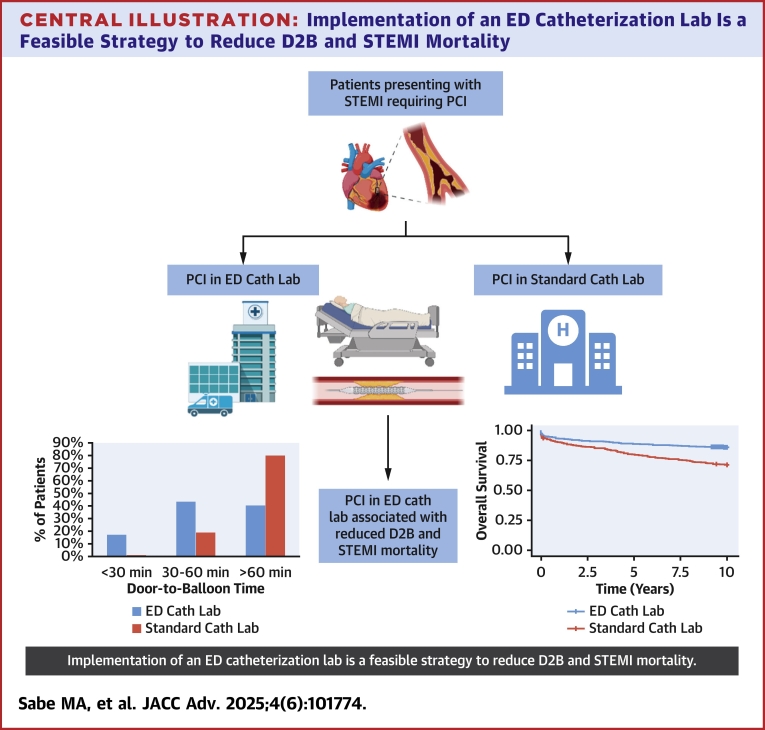 Figure 1
Figure 1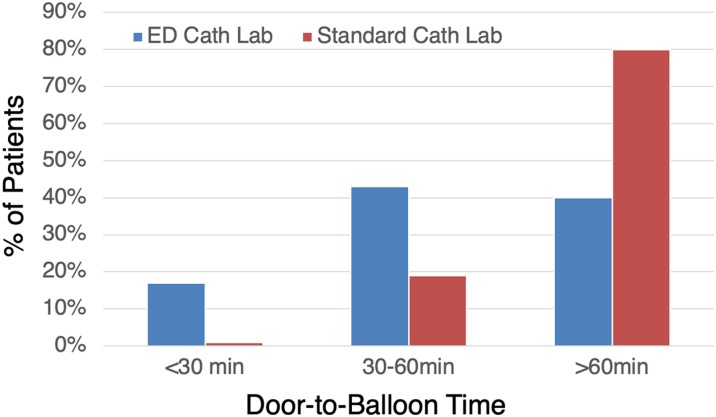 Figure 2
Figure 2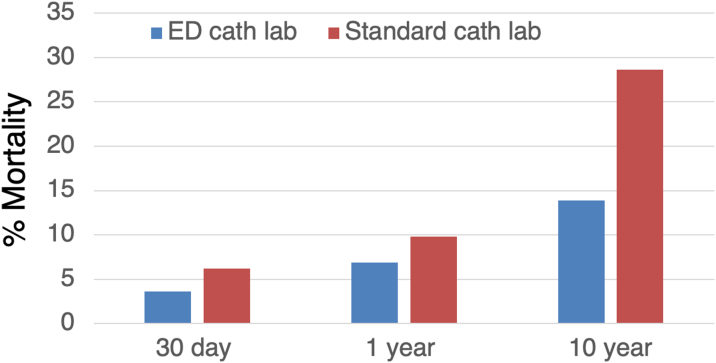 Figure 3
Figure 3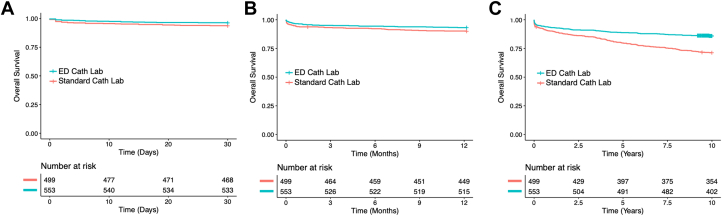 Figure 4
Figure 4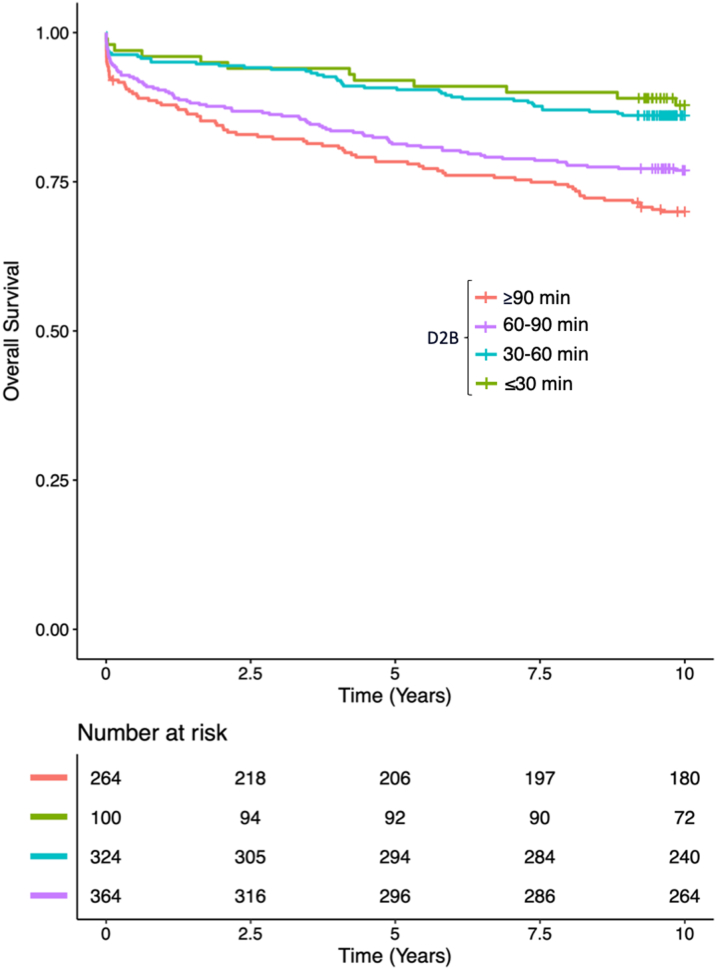 Figure 5
Figure 5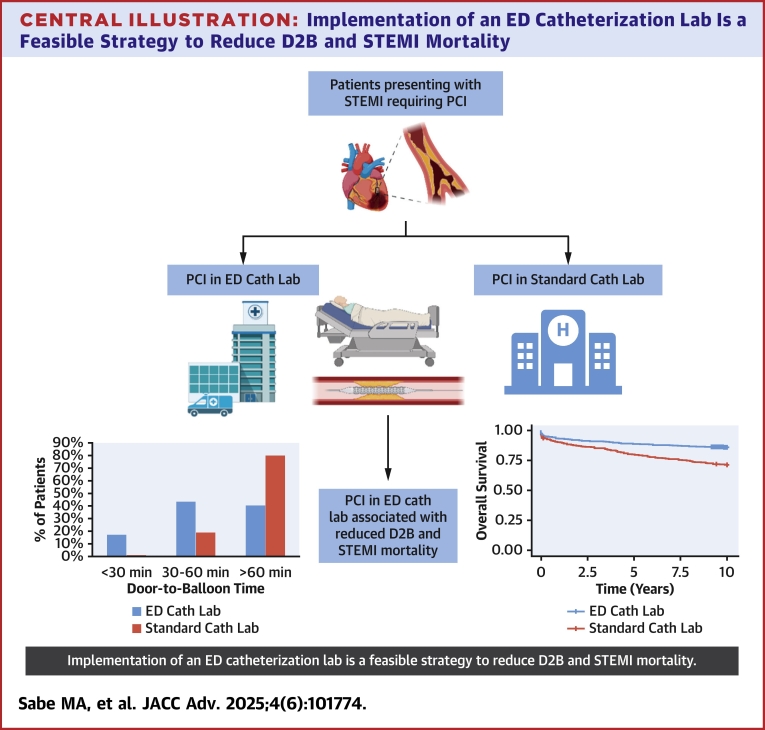 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Myocardial Infarction Research · Cardiac Arrest and Resuscitation · Cardiac Imaging and Diagnostics
Primary percutaneous coronary intervention (PCI) is the treatment of choice for acute ST-segment elevation myocardial infarction (STEMI). In this setting, decreased door-to-balloon (D2B) time is associated with improved patient outcomes. The recommended D2B time is <90 minutes, and every 30-minute increase in D2B time has been shown to increase 1-year mortality by 7.5%.1 Park et al2 found that every reduction in D2B time by 30 minutes was associated with continuous improvement in 1-year mortality. Furthermore, D2B ≤30 minutes may be associated with improved in-hospital mortality compared to D2B >30 minutes, even if less than the recommended 90-minute threshold.3
In an effort to keep D2B <90 minutes, there have been worldwide attempts to reduce D2B time. These include out-of-hospital ECG transmission,4^,^5 obtaining ECG within 10 minutes of presentation, central paging systems for cath lab activation,6 emergency department (ED) triage of patients with early activation of catheterization labs by the ED physicians,7 and immediate transfer by an in-house transfer team.8 Khot et al8 found that among patients presenting with STEMI, ED physician-directed activation of the catheterization lab and ED-mediated transfer to an immediately available catheterization lab resulted in shorter D2B times. Importantly, these strategies were associated with a reduced mean infarct size, length of stay, and total hospital costs per admission.8 Therefore, hospital implementation of strategies targeted to reduce D2B times are necessary to improve outcomes in patients with STEMI.
In addition to some of the aforementioned techniques to decrease D2B time, we implemented a catheterization laboratory within the ED at our institution as a novel strategy to further reduce D2B time and improve access to immediate revascularization. In this study, we compare D2B time and mortality in patients presenting with STEMI to the ED-based vs standard catheterization labs at a community hospital. To our knowledge, this is the first reported study of an emergency chest pain center which includes a catheterization lab in the ED.
Methods
Study population
We included 1,053 consecutive patients with STEMI who underwent primary angioplasty at our institution between April 1998 and December 2011. Patients were non-randomized to either the ED or standard catheterization laboratory (cath lab). The decision to send the patient to either cath lab was based on physician preference and catheterization laboratory availability. Standard STEMI protocol was utilized in both labs. Patients who refused cardiac catheterization or had a contraindication to cardiac catheterization were excluded from the study. This study was approved by the Cleveland Clinic Mercy Hospital Institutional Review Board (IRB#2019006).
Variables and outcomes of interest
The exposure of interest was the type of cath lab used (ED vs standard). The primary endpoints were D2B time and time to death (up to 30 days, 1 year, and 10 years). Patient demographics, medications, and past medical history were collected from the electronic medical record. Left ventricular ejection fraction (LVEF) and mitral regurgitation severity were obtained from a 2-dimensional echocardiogram or left ventriculogram that was obtained during the STEMI hospitalization. D2B time (in minutes) was collected at the time of catheterization and calculated as the time from entry into our institution to reperfusion. Mortality data were obtained from the social security death index and the hospital medical record.
Statistical analysis
Continuous variables were examined for normality and reported as either mean ± SD or median (IQR). Categorical variables were expressed as a number and percent. A Student's t-test (for normal variables) and a Wilcoxon rank-sum test (for non-normal variables) were used to compare continuous variables. A Fisher's exact test was used to compare categorical variables.
A multivariable linear regression model was used to assess the relationship between cath lab location and door-to-balloon time in minutes. We included variables that could be confounders of this relationship as well as other predictors of our outcomes. We entered into the model any variable with an association with the outcomes on univariable analysis with a P value <0.20 in addition to those which were clinically relevant.
The univariate relationship between cath lab location and the primary outcome time to death (up to 30 days, 1 year, 10 years) was examined using a Kaplan-Meier curve. A Cox proportional hazards model was used to adjust for univariate predictors of mortality. Age, sex, and race were included in the model, as were any predictors with a P value < 0.2 on univariate analysis and those that were clinically relevant. Specifically, we included clinical variables that could have an impact on mortality in patients presenting with STEMI, including history of diabetes, hypertension, congestive heart failure, severe mitral regurgitation, and prior coronary artery bypass grafting (CABG). Additional clinical variables at the time of presentation that could impact mortality were included in the model such as cardiogenic shock and the use of intra-aortic balloon pump.
We also examined the relationship between D2B (divided into categories) and mortality using a Cox proportional hazards model and included relevant covariates as noted earlier.
Results
A total of 1,053 patients who presented with STEMI were included in this analysis; 553 of which were treated in the ED cath lab, and 500 went to the standard cath lab. There was no significant difference in the age (59.7 vs 58.9 years, P = 0.29), sex (70% vs 73% male, P = 0.31), or race (95% vs 94% white, P = 0.31) between the 2 groups (see Table 1). Approximately 20% of all patients had diabetes mellitus (DM), and there were no significant differences in the rate of diabetes between the 2 groups (P = 0.4). There was no significant difference between a history of CABG (P = 0.8) or left main coronary artery disease on presentation (P = 0.7). Patients who presented to the standard cath lab were more likely to have an LVEF <40% (11% vs 6.5%, P = 0.005), but there was no difference in Killip class at presentation (P = 0.16). Unadjusted outcomes comparing ED and standard cath lab groups are reported in Table 2.Table 1. Baseline Characteristics of ED vs Standard Cath LabED Cath Lab (n = 553)Standard Cath Lab (n = 500)P ValueAge, y59.7 ± 12.958.9 ± 12.20.29Sex0.31 Male386 (70%)364 (73%) Female167 (30%)137 (27%)Race White523 (95%)470 (94%) Black25 (5%)28 (6%) Other5 (<1%)2 (<1%)History of DM109 (20%)88 (18%)0.37History of HTN253 (46%)214 (43%)0.35LVEF <40%36 (6.5%)57 (11%)0.005Killip Class 3-434 (6.1%)42 (8.4%)0.16History of CABG40 (7.3%)39 (7.8%)0.75Culprit vessela LM7 (1.3%)5 (1.0%) LAD191 (35%)175 (35%) LCx86 (16%)59 (12%) RCA289 (52%)258 (51.6%) SVG10 (1.8%)13 (2.6%) Ramus5 (0.9%)7 (1.4%)CABG = coronary artery bypass grafting; DM = diabetes mellitus; ED = emergency department; HTN = hypertension; LAD = left anterior descending coronary artery; LCx = left circumflex coronary artery; LM = left main coronary artery; LVEF = left ventricular ejection fraction; RCA = right coronary artery; SVG = saphenous vein graft; Ramus = ramus intermedius coronary artery.aSome patients presented with multiple culprit coronary vessels.Table 2. Unadjusted Outcomes Comparing ED vs Standard Cath LabED Cath Lab (n = 553)Standard Cath Lab (n = 500)Unadjusted P ValueD2B<0.001 <30 min96 (17%)4 (0.8%) 30-60 min232 (42%)92 (18%) >60 min225 (41%)404 (81%)IABP137 (25%)163 (33%)0.005LOS post-intervention4.4 (6.4)4.4 (4.4)0.997cath lab = catheterization laboratory; D2B = door to balloon time; ED = emergency department; IABP = intra-aortic balloon pump placement; LOS = length of stay.
After adjusting for covariates, the patients who were treated in the ED cath lab had a significantly lower D2B time than patients treated in the standard cath lab (median 54 vs 83 minutes, P < 0.001). When D2B time was split into categories of <30 minutes, 30 to 60 minutes, and ≥60 minutes, patients in the ED cath lab were more likely to have a <30-minute D2B time (17% vs <1%, P < 0.001) (Figure 1). Twenty-eight patients had D2B ≤15 minutes, and all these patients were treated in the ED cath lab. The lowest D2B in this study was 6 minutes, and this patient was treated in the ED cath lab.Figure 1. Door-to-Balloon Times in ED and Standard Catheterization LabsPatients presenting with ST-segment elevation myocardial infarction undergoing primary percutaneous intervention had lower door-to-balloon times when treated in the emergency department catheterization lab (ED cath lab, blue bars), compared to standard catheterization lab (standard cath lab, red bars).
After adjusting for age, sex, race, history of DM, history of heart failure, history of CABG, history of hypertension, cardiogenic shock on presentation, the use of intraaortic balloon pump, severe mitral regurgitation, and LVEF <40%, patients who presented to the ED cath lab had a significantly lower 30-day mortality (adjusted hazard ratio [adj HR]: 0.54, 95% CI: 0.29-0.99, P = 0.047) and 1-year mortality (adj HR: 0.58, 95% CI: 0.37-0.91, P < 0.018) than patients treated in the standard cath lab. Patients who were treated in the ED cath lab also had significantly lower long-term (up to 10 years) mortality than patients treated in the standard cath lab (adj HR: 0.39, 95% CI: 0.29-0.53, P < 0.0001) (Table 3, Figures 2 and 3, Figure 2, Figure 3). Other significant predictors of mortality included older age, a diagnosis of DM, LVEF <40%, and cardiogenic shock on presentation (Table 4).Table 3. Adjusted Hazard Ratios Comparing Mortality in ED vs Standard Cath LabSurvival Follow-Up TimeAdjusted HR for ED Cath Lab vs Standard Cath LabP Value30 d0.540.0471 y0.580.01810 y0.39<0.0001cath lab = catheterization laboratory; ED = emergency department; HR = hazard ratio.Figure 2. Thirty-Day, 1-Year, and 10-Year Mortality in ED and Standard Catheterization LabsPercent mortality demonstrated in patients treated in emergency department catheterization lab (ED cath lab, blue bars), compared to standard catheterization lab (standard cath lab, red bars).Figure 3. Cox Regression Assessing Short- and Long-Term Mortality in ED vs Standard Catheterization LabCox proportional hazards regression plot shown for (A) 30-day mortality, (B) 1-year mortality, and (C) 10-year mortality of patients presenting with ST-segment elevation myocardial infarction undergoing percutaneous intervention in the emergency department catheterization lab (ED cath lab, blue) compared to standard catheterization lab (standard cath lab, red).Central IllustrationImplementation of an ED Catheterization Lab Is a Feasible Strategy to Reduce D2B and STEMI Mortalitycath lab = catheterization lab; ED = emergency department; PCI = percutaneous coronary intervention; STEMI = ST-segment elevation myocardial infarction.Table 4. Multivariable Cox Regression Model: Predictors of 10-Year MortalityHR95% CIP ValueED cath lab0.390.29-0.53<0.0001Age1.041.03-1.06<0.0001Female1.190.88-1.610.25Race (White)0.730.1-5.440.76History of DM1.811.35-2.44<0.0001History of CABG1.10.7-1.720.68IABP1.10.79-1.510.59Cardiogenic shock2.631.75-3.94<0.0001LVEF <40%2.221.66-2.97<0.00013-4+ MR1.200.83-1.730.33HTN1.050.8-1.390.71CABG = coronary artery bypass grafting; cath lab = catheterization laboratory; DM = diabetes mellitus; ED = emergency department; HTN = hypertension; IABP = intra-aortic balloon pump; LVEF = left ventricular ejection fraction; MR = mitral regurgitation.
Lower D2B was found to be associated with improved survival (Figure 4). After adjusting for relevant covariates, D2B < 30 min and 30-60 min was associated with significant improvement in mortality at 10 years compared to D2B > 90 min (Table 5).Figure 4. Cox Regression Demonstrating Categorical Door-to-Balloon Time and 10-Year SurvivalCox proportional hazards regression plot shown for 10-year mortality of patients presenting with ST-segment elevation myocardial infarction undergoing percutaneous intervention categorized based on door-to-balloon time (D2B).Table 5. Multivariable Cox Regression Model: Door-to-Balloon Time and 10-Year MortalityHR95% CIP ValueD2B (ref: >90 min) <30 min0.350.19-0.670.001 30-60 min0.480.33-0.700.0001Age1.041.03-1.05<0.0001Female1.120.83-1.500.46Race (White)1.290.17-9.50.80History of DM1.831.36-2.47<0.0001History of CABG1.00.64-1.580.97IABP1.210.88-1.660.25Cardiogenic shock2.431.62-3.66<0.0001LVEF <40%2.041.53-2.72<0.00013-4+ MR1.310.92-1.890.14HTN0.960.72-1.270.76CABG = coronary artery bypass grafting; D2B = door to balloon time; DM = diabetes mellitus; HTN = hypertension; IABP = intra-aortic balloon pump; LVEF = left ventricular ejection fraction; MR = mitral regurgitation.
Discussion
In the present study, we sought to examine whether implementation of a catheterization laboratory in the emergency department for primary PCI improved door-to-balloon times and survival in patients presenting with STEMI to a community hospital. To our knowledge, this is the first reported study describing a cath lab in the ED, and we present the lowest published D2B time of 6 minutes. We found that patients treated in the ED cath lab had a significantly lower D2B time than patients treated in the standard cath lab, with 17% of patients having a D2B <30 minutes and a minimum D2B of 6 minutes. Of note, this cath lab did have a D2B as low as 5 minutes, which occurred after the analysis presented here.
D2B time of <90 minutes has been shown to be associated with decreased mortality in patients presenting with STEMI.9, 10, 11 Therefore, the American College of Cardiology/American Heart Association recommends a D2B of 90 minutes or less in these patients.12 However, there are conflicting data regarding D2B time. Menees et al13 found no significant difference in in-hospital and 30-day mortality in a large national registry (CathPCI Registry) despite improvements in D2B time, and they suggest that improved outcomes may be a reflection of institutional factors and/or operator experience. That particular study did not assess longer-term survival, and the authors note that this is a limitation of the study and that benefit may be seen in the long term.13 Our study demonstrated improved 30-day mortality, 1-year mortality, as well as long-term mortality up to 10 years. After adjusting for relevant covariates, our study also found that older age, history of DM, LVEF <40%, and cardiogenic shock on presentation were significant independent predictors of mortality in this patient population.
The long-term benefit of shorter D2B time may be related to improved long-term left ventricular function, decrease in scar formation, and possibly less scar-mediated sudden cardiac death; however, these hypotheses would need to be assessed in future studies. The phrase “time is muscle” has been emphasized by experts as data have shown that early PCI can improve LV function.14
There are some practical issues to consider when building a cath lab in the ED. Our team had to obtain institutional as well as state support to allow for a smaller than average sized cath lab to be built within the ED only for use in emergent cases. In addition to size limitations, it is important to consider cost, maintenance, and education of ED staff. We did have ED nurses who were cross-trained for the cath lab, which allowed for immediate triage, evaluation, and preparation in the ED cath lab upon arrival. Although the ED cath lab and standard cath lab are no farther than 5 minutes apart, the majority of time saved stems from streamlined logistics of evaluation and transfer especially during off-hours when the cath lab team is not in-house. Although a 6-minute door-to-balloon time is not the norm, when a patient is able to be evaluated, triaged, and prepped upon arrival with a cath lab team already called en route, very short D2B times were able to be obtained. The cath lab team is on call from home and do not stay in-hospital for call. However, when pre-hospital ECG STEMIs are called by emergency medical technicians, there are instances when D2B can be quite short and under 10 minutes. There are other practical benefits in having an ED cath lab, for instance, with unstable patients, especially during off-hours, there are readily available ED physicians ready to intubate and further support patients from a critical care perspective. In addition, the ED cath lab at our institution was used for emergent transvenous pacers when necessary.
Study limitations
This study had several limitations, including that it was an observational, single-center analysis. As opposed to tertiary care centers where a significant number of patients with STEMI are triaged in the prehospital phase (ie, from a referral hospital), most of the patients presenting at this community hospital, similar to other community hospitals, were self-presenters, which could account for the higher overall D2B times. However, this study emphasizes that an emergency chest pain center is a model that could enhance the care of patients presenting with STEMI at local hospitals. Another limitation is that we did not have data available about post-PCI LV function or heart failure, which could account for long-term outcomes. As opposed to death data, which were available from the social security death index (SSDI), these data were not readily available as not all patients continued to follow up at this hospital in the long term. Another limitation of this study is that patients were not randomized to the 2 different cath lab locations; however, there were similar numbers of patients in each group and very few differences in baseline characteristics. There is nonetheless risk of selection bias and residual confounding particularly with regard to allocation to ED vs standard cath labs. Although patients who presented to the standard cath lab were more likely to have heart failure with reduced ejection fraction, and thus may represent a sicker patient population and may have reflected a selection bias in referral, after adjusting for cardiogenic shock on admission, LM disease, and LVEF ≤40%, the use of the ED cath lab was independently associated with lower mortality. There were periods of time when the ED cath lab was closed for renovation, during which all patients were referred to the standard cath lab; however, this was a short time period overall and did not correlate specifically with the beginning or end of the study time period. The authors recognize that temporal changes in STEMI treatment protocols and technology can also impact D2B and mortality outcomes and look forward to evaluating the impact of the ED cath lab in contemporary cohorts. Finally, for the long-term follow-up, death data were assessed using medical record review and SSDI, which may have limitations if a patient was not recorded as expired in the medical record or SSDI.
Conclusions
In this observational study, we found that implementation of a cath lab for primary PCI in the ED significantly improved D2B time as well as 30-day, 1-year, and long-term mortality in patients presenting with STEMI at a community hospital. To our knowledge, this is the first reported study to present this novel technique to reduce D2B times and subsequently improve survival in patients presenting with STEMI. Implementation of a cath lab in the ED is a feasible option for institutions with primary PCI and requires collaboration between interventional cardiology and emergency medicine teams.PerspectivesCOMPETENCY IN SYSTEMS-BASED PRACTICE: Implementation of hospital-based strategies to reduce door-to-balloon time in the treatment of patients presenting with acute ST-segment elevation myocardial infarction is important to reduce cardiovascular mortality. We implemented a catheterization laboratory within the ED at our institution as a novel strategy to further reduce D2B time and improve access to immediate revascularization. We found that D2B was shorter in ED vs standard catheterization lab patients, and ED catheterization lab patients had lower short- and long-term mortality than standard catheterization lab patients.TRANSLATIONAL OUTLOOK: These findings indicate that implementation of an ED catheterization lab is a feasible strategy which community hospitals can utilize to reduce D2B and STEMI mortality.
Funding support and author disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1De Luca G.Suryapranata H.Ottervanger J.P.Antman E.M.Time delay to treatment and mortality in primary angioplasty for acute myocardial infarction: every minute of delay counts Circulation 109102004122312251500700810.1161/01.CIR.0000121424.76486.20 · doi ↗ · pubmed ↗
- 2Park J.Choi K.H.Lee J.M.Prognostic implications of door-to-balloon time and onset-to-door time on mortality in patients with ST -segment-elevation myocardial infarction treated with primary percutaneous coronary intervention J Am Heart Assoc 892019 e 01218810.1161/JAHA.119.012188 PMC 651211531041869 · doi ↗ · pubmed ↗
- 3Yamada T.Takahashi A.Mizuguchi Y.Impact of shorter door-to-balloon time on prognosis of patients with STEMI-single-center analysis with a large proportion of the patients treated within 30 min Cardiovasc Interv Ther 3422019971042973667010.1007/s 12928-018-0521-1 · doi ↗ · pubmed ↗
- 4Canto J.G.Rogers W.J.Bowlby L.J.French W.J.Pearce D.J.Weaver W.D.The prehospital electrocardiogram in acute myocardial infarction: is its full potential being realized? National Registry of Myocardial Infarction 2 Investigators J Am Coll Cardiol 2931997498505906088410.1016/s 0735-1097(96)00532-3 · doi ↗ · pubmed ↗
- 5Emergency department: rapid identification and treatment of patients with acute myocardial infarction. National Heart Attack Alert Program coordinating committee, 60 minutes to treatment working group Ann Emerg Med 23219943113298304613 · pubmed ↗
- 6Eckstein M.Koenig W.Kaji A.Tadeo R.Implementation of specialty centers for patients with ST-segment elevation myocardial infarction Prehosp Emerg Care 13220092152221929156010.1080/10903120802471980 · doi ↗ · pubmed ↗
- 7Bradley E.H.Herrin J.Wang Y.Strategies for reducing the door-to-balloon time in acute myocardial infarction N Engl J Med 355222006230823201710161710.1056/NEJ Msa 063117 · doi ↗ · pubmed ↗
- 8Khot U.N.Johnson M.L.Ramsey C.Emergency department physician activation of the catheterization laboratory and immediate transfer to an immediately available catheterization laboratory reduce door-to-balloon time in ST-elevation myocardial infarction Circulation 1161200767761756296010.1161/CIRCULATIONAHA.106.677401 · doi ↗ · pubmed ↗