Use of Direct Oral Anticoagulants in Patients With Upper Extremity Deep Vein Thrombosis: A Meta-Analysis of Efficacy and Safety
Ayman Zyada, Ayman Fakhry, Sohiel Nagib, Omar Alnadi, Ahmed Abouelseoud, Rahma Seken, Muhammad Jabr

TL;DR
This study finds that direct oral anticoagulants may be more effective than heparin for treating upper extremity blood clots, but they carry a higher bleeding risk.
Contribution
First meta-analysis comparing direct oral anticoagulants and heparin specifically for upper extremity deep vein thrombosis.
Findings
DOACs showed significantly lower mortality and thrombotic complications compared to historical LMWH data.
Major bleeding rates were higher with DOACs than with LMWH.
Most UEDVT cases were cancer-related or catheter-associated, with rivaroxaban being the most used DOAC.
Abstract
Upper extremity deep vein thrombosis (UEDVT), distinct in etiology from lower limb DVT, often arises from catheter use, malignancy, or thoracic outlet syndrome. While direct oral anticoagulants (DOACs) are established for lower limb DVT, their role in UEDVT remains understudied. This meta-analysis evaluates the efficacy and safety of DOACs compared to low-molecular-weight heparin (LMWH) in UEDVT. A systematic PubMed search identified nine studies (643 DOAC-treated patients). Outcomes included mortality, venous thromboembolism (VTE) recurrence, pulmonary embolism (PE), and major bleeding. DOACs demonstrated significantly lower mortality (2.49% vs. 16.5-27.5%; p<0.001), VTE recurrence (0.93% vs. 5%; p<0.001), and PE incidence (0.31% vs. 5-8%; p<0.001) compared to historical LMWH data. However, major bleeding rates were higher with DOACs (2.02% vs. 0.25%; p<0.001). Patient cohorts…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
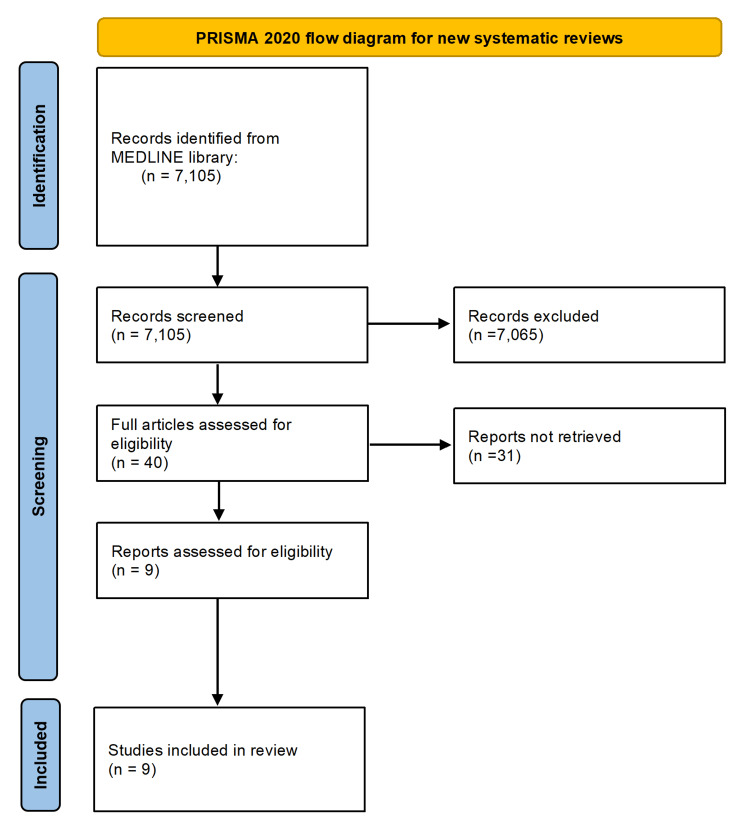 Figure 1
Figure 1| Author | Study Design | Centres | Country | DOAC-N | Total-N | Age-M | Male-N | Ca ptn | Cath ptn | DOAC Agent | |
| 1 | Davies et al. 2018 [ | Prospective | Multicentre | Canada | 70 (100.0%) | 70 | 54 | 23 (32.9%) | 70 (100.0%) | 70 (100.0%) | R70 |
| 2 | Fan et al. 2020 [ | Prospective | Multicentre | China | 44 (52.4%) | 84 | 51 | 25 (29.8%) | 84 (100.0%) | 84 (100.0%) | R44 |
| 3 | Fiori et al. 2020 [ | Retrospective | Single centre | Italy | 10 (100.0%) | 10 | 28 | 3 (30.0%) | 0 (0.0%) | 0 (0.0%) | R5-A5 |
| 4 | Houghton et al. 2017 [ | Prospective | Single centre | USA | 102 (48.6%) | 210 | 60 | 124 (59.0%) | 125 (59.5%) | 107 (51.0%) | R39-A63 |
| 5 | Laube et al. 2017 [ | Retrospective | Single centre | USA | 83 (100.0%) | 83 | 62 | 32 (38.6%) | 83 (100.0%) | 83 (100.0%) | R83 |
| 6 | Montiel et al. 2017 [ | Retrospective | Multicentre | Sweden | 55 (100.0%) | 55 | 49 | 27 (49.1%) | 10 (18.2%) | 5 (9.1%) | R46-A7-D2 |
| 7 | Porfidia et al. 2020 [ | Retrospective | Multicentre | Italy | 61 (100.0%) | 61 | 49 | 32 (52.5%) | 0 (0.0%) | 0 (0.0%) | R37-A11-D7-E6 |
| 8 | Schastlivtsev et al. 2019 [ | Prospective | Single centre | Russia | 30 (100.0%) | 30 | 52 | 13 (43.3%) | 2 (6.7%) | 4 (13.3%) | R30 |
| 9 | Vedovati et al. 2021 [ | Prospective | Multicentre | Europe | 188 (100.0%) | 188 | 52 | 88 (46.8%) | 55 (29.3%) | 62 (33.0%) | R102-A56-D12-E18 |
| Characteristics | Value |
| Total patients with UEDVT treated with DOAC | 643 |
| Median age | 52 years |
| Male percentage | 57.11% |
| Percentage of patients with cancer | 66.72% |
| Percentage of patients with a central line | 64.53% |
| Median treatment period | 3 months |
| Median follow-up period | 6 months |
| Outcome | Events (n) | Total Patients | Proportion (p) | 95% CI |
| Death | 16 | 643 | 2.49% | 1.50%-3.98% |
| Recurrence of VTE | 6 | 643 | 0.93% | 0.38%-2.03% |
| Pulmonary embolism | 2 | 643 | 0.31% | 0.06%-1.12% |
| Major bleeding | 13 | 643 | 2.02% | 1.13%-3.42% |
| Outcome | DOAC (%) | LMWH (%) (Median) | z-Score | p-Value | Significance |
| Mortality | 2.49 | 22.0 (16.5-27.5) | -12.06 | <0.001 | DOAC significantly lower |
| VTE recurrence | 0.93 | 5.0 | -4.73 | <0.001 | DOAC significantly lower |
| Pulmonary embolism | 0.31 | 6.5 (5-8) | -6.32 | <0.001 | DOAC significantly lower |
| Major bleeding | 2.02 | 0.25 (2.5 per 1,000) | 8.99 | <0.001 | DOAC significantly higher |
| Methodological Component | Description |
| Effect size | Proportions (e.g., recurrence rate, mortality) |
| CI method | Clopper–Pearson exact |
| Comparative test | One-sample z-test against historical controls |
| Heterogeneity | Calculated Q and I² separately |
| Software | Stata, version 12.0 (StataCorp LLC, Texas) |
| Limitations | Absence of data allowing random-effects model or subgroup analysis |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVenous Thromboembolism Diagnosis and Management · Diagnosis and Treatment of Venous Diseases · Atrial Fibrillation Management and Outcomes
Introduction and background
Direct oral anticoagulants (DOACs, a class of oral blood-thinning medications) are approved for the treatment of lower limb deep vein thrombosis (DVT) and have been extensively studied in comparison to traditional anticoagulants in terms of efficacy and safety [1,2]. However, evidence regarding their use in upper extremity DVT (UEDVT, blood clots in the deep arm/shoulder veins) remains scarce.
UEDVT can lead to life-threatening complications such as pulmonary embolism (PE) if untreated, and it presents distinct characteristics compared to lower limb DVT. While some cases share common risk factors, such as malignancy, hereditary and acquired thrombophilia, sepsis, pregnancy, and immobility associated with fractures [3,4], UEDVT is frequently secondary to conditions such as central venous catheter placement, iatrogenic injuries, axillary lymphadenopathy, or thoracic outlet syndrome (TOS).
DOACs may behave differently in UEDVT compared to lower limb DVT due to distinct pathophysiological and clinical factors. UEDVT is often catheter-related or cancer-associated, involving fibrin-rich thrombi and persistent prothrombotic stimuli, which may respond less effectively to DOACs. Additionally, faster venous flow, altered hemodynamics, and the presence of foreign bodies like catheters can impact drug distribution and clot resolution. In cancer patients, drug interactions and altered pharmacokinetics further complicate DOAC use. Unlike lower limb DVT, UEDVT lacks strong clinical trial data supporting DOAC efficacy, making low-molecular-weight heparin (LMWH) the preferred treatment in many such cases.
Current guidelines provide recommendations for the management of UEDVT. The European Society for Vascular Surgery (ESVS) guidelines suggest anticoagulation therapy unless major contraindications are present, with LMWH, an injectable anticoagulant, followed by vitamin K antagonists as the conventional regimen [5]. Similarly, the American College of Chest Physicians (ACCP) guidelines recommend anticoagulation for a minimum duration of three months [6].
The primary aim of this study is to assess the efficacy of DOACs in the treatment of UEDVT and to compare their outcomes with those reported for traditional anticoagulant therapies. This study was previously presented at the International Vein Congress (IVC Miami 2025) on April 26, 2025.
Method
A meta-analysis evaluated existing literature on UEDVT cases treated with DOACs, comparing their clinical outcomes with those of conventional anticoagulant therapies. A systematic literature search was performed in MEDLINE using MESH keywords: "DOAC", "AND", "upper limb DVT", following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, without imposing language restrictions up to February 21, 2025. Manual screening of reference lists from retrieved articles was conducted to identify additional eligible studies. Inclusion criteria comprised confirmed diagnoses of UEDVT, treatment with DOACs, and documented follow-up completion. Exclusion criteria encompassed studies involving thrombolytic therapy, incomplete follow-up data, no reported clinical outcomes in anticoagulated patients, and case reports or case series with fewer than 10 participants.
From the initial 7,105 records identified, 7,065 were excluded following title and abstract screening. Forty studies underwent full-text evaluation and were double-checked by another assessor to avoid bias, of which nine met the inclusion criteria, encompassing a pooled cohort of 643 patients for final analysis. The PRISMA flow diagram is shown in Figure 1.
PRISMA flow chart PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses
The primary clinical outcomes assessed included mortality, venous thromboembolism (VTE) recurrence, incidence of PE, and major bleeding events. Recurrent VTE was defined as recurrent UEDVT and DVT of the lower limbs or thrombosis occurring at unusual sites in most studies. Major bleeding was defined according to the criteria of the International Society of Thrombosis and Haemostasis in seven studies. PE was limited to symptomatic ones in most studies. We have used the Newcastle-Ottawa Scale to assess the quality of risk of bias in the included studies, which showed a 7/9 score given to historical LMWH data used and heterogeneous cohorts; however, this score indicates a low risk of bias.
Review
Results
The nine studies included patients with UEDVT of varying etiologies [7-16], including idiopathic, coagulopathic, iatrogenic, central line-related, malignancy-associated DVT, and TOS-related DVT, as shown in Table 1.
Patients' characteristics
A total of 643 patients with UEDVT were treated with DOACs. The median age was 52 years, with 57.11% of the patients being male. Among the studied population, 66.72% had cancer-related UEDVT and 64.53% had catheter-related thrombosis, as shown in Table 2.
Among the patients treated with DOACs, the distribution of specific agents was as follows: rivaroxaban (70.9%), apixaban (22%), edoxaban (3.7%), and dabigatran (3.3%). The median treatment duration was three months, while the median follow-up period extended to six months. The overall mortality rate among DOAC-treated patients was 2.49% (16/643). The recurrence rate of VTE was observed to be 0.93% (6/643), while the incidence of PE was relatively low at 0.31% (2/643). Additionally, the occurrence of major bleeding events was documented at 2.02% (13/643). These outcomes are summarized in Table 3.
Statistical comparison with LMWH
The outcomes of DOAC-treated patients were compared with historical LMWH data for the four primary endpoints: mortality, VTE recurrence, PE, and major bleeding, as shown in Table 4.
Regarding mortality, the DOAC-treated cohort reported 16 deaths among 643 patients (2.49%). In contrast, LMWH-treated populations historically exhibited 30-day mortality rates, ranging from 16.5% to 27.5% in UEDVT patients [17]. A one-sample z-test confirmed this difference as statistically significant (z=−12.06, p<0.001), favoring DOACs.
Recurrent VTE occurred in six DOAC-treated patients (0.93%), whereas LMWH/warfarin regimens are associated with a 5% recurrence rate in UEDVT [17]. The z-test demonstrated statistical significance (z=−4.73, p<0.001). PE incidence was 0.31% (2/643) with DOACs compared to 5-8% in LMWH cohorts [17]. The difference was significant (z=−6.32, p<0.001). DOACs had a higher major bleeding rate (2.02%, 13/643) compared to LMWHs (0.25%, 2.5/1,000) [18]. This increase was statistically significant (z=8.99, p<0.001).
The Cochran’s Q, I² statistic, and p-values for heterogeneity across the nine studies in the meta-analysis for each outcome are as follows: 1. VTE recurrence: Q=6.10, I²=0%, p=0.64, so, there is no significant heterogeneity among studies for VTE recurrence. 2. PE: Q=2.02, I²=0%, p=0.98, it indicates extremely low variability; no heterogeneity detected. 3. Major bleeding: Q=13.37, I²=40.2%, p=0.10, a moderate heterogeneity is present. Although not statistically significant (p>0.05), variability across studies warrants caution in interpreting pooled results. The summary of data synthesis approach is shown in Table 5.
Discussion
Interpretations
DOACs were associated with a significantly lower mortality rate (2.49% vs. 16.5-27.5%) [17]. Similarly, the recurrence rate of VTE was lower in the DOAC cohort (0.93%) compared to LMWH historical data (5%) [17]. The incidence of PE was also lower among DOAC-treated patients (0.31% vs. 5-8%) [17]. However, the major bleeding rate appeared to be higher with DOACs (2.02%) than with LMWH (0.25%) [18].
The findings suggest that DOACs may offer a favorable safety and efficacy profile in the management of UEDVT. Notably, the lower mortality and recurrence rates observed with DOACs, compared to historical LMWH data, highlight their potential advantage. However, the higher incidence of major bleeding associated with DOAC use raises concerns that warrant further investigation to explore bleeding risk modifiers (e.g., renal function, DOAC type).
Limitations
Several factors contribute to the challenges of studying UEDVT, including heterogeneity in patient populations, variations in the underlying etiology of thrombosis, and differences in anticoagulant regimens. The diverse pathophysiology of UEDVT, particularly catheter-associated and malignancy-associated cases, may influence treatment response and outcomes. Moreover, variations in follow-up protocols across studies make direct comparisons challenging.
The lack of routine imaging follow-up to assess venous patency limits the ability to determine the long-term impact of DOACs on clot resolution and post-thrombotic syndrome development. Future studies should aim to incorporate standardized imaging and longer follow-up periods to better evaluate the durability of treatment effects. We also acknowledge certain limitations of this study, including potential confounding variables of the patients' understanding predisposing factors, the use of various DOAC agents in the nine studies we included, and the reliance on historical data for LMWH comparisons. Small PE event numbers might limit statistical power to detect differences. Also, combining retrospective and prospective studies might bias pooled estimates.
Conclusions
The available data suggest that DOACs may offer advantages over LMWHs in terms of lower mortality and PE incidence rates in UEDVT patients. However, because the available sources do not provide specific recurrence or major bleeding rates for LMWH across distinct DVT subgroups, such as cancer-related or catheter-related cases, we were unable to perform comprehensive statistical comparisons for these outcomes. As the advantages of DOACs in this study are based solely on indirect comparisons with historical controls, further randomized head-to-head trials with detailed outcome data are necessary to fully assess the comparative effectiveness and safety of DOACs versus LMWHs in UEDVT treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rivaroxaban compared with standard anticoagulants for the treatment of acute venous thromboembolism in children: a randomised, controlled, phase 3 trial Lancet Haematol Male C Lensing AWA Palumbo JS 18277202010.1016/S 2352-3026(19)30219-431699660 · doi ↗ · pubmed ↗
- 2Apixaban Agrawal A Kerndt CC Manna B Treasure Island (FL): Stat Pearls Publishing Stat Pearls [Internet], Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 507910/
- 3Risk and prognosis of upper extremity deep vein thrombosis Ann Vasc Dis Endo Y Unno N Yamamoto N 2002041620233777965310.3400/avd.oa.23-00005 PMC 10539128 · doi ↗ · pubmed ↗
- 4Diagnosis and management of upper extremity deep-vein thrombosis in adults Thromb Haemost Grant JD Stevens SM Woller SC 1097110810820122309331910.1160/TH 12-05-0352 · doi ↗ · pubmed ↗
- 5Editor's choice - European Society for Vascular Surgery (ESVS) 2021 clinical practice guidelines on the management of venous thrombosis Eur J Vasc Endovasc Surg Kakkos SK Gohel M Baekgaard N 9826120213333467010.1016/j.ejvs.2020.09.023 · doi ↗ · pubmed ↗
- 6Antithrombotic therapy for VTE disease: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines Chest Kearon C Akl EA Comerota AJ 096141201210.1378/chest.11-2301 PMC 327804922315268 · doi ↗ · pubmed ↗
- 7Midterm outcomes in patients with upper extremity deep vein thrombosis J Vasc Surg Venous Lymphat Disord Beiswenger AC Quereshy HA Rouabhi M 930938820203245702310.1016/j.jvsv.2020.02.024 · doi ↗ · pubmed ↗
- 8A prospective study of rivaroxaban for central venous catheter associated upper extremity deep vein thrombosis in cancer patients (catheter 2)Thromb Res Davies GA Lazo-Langner A Gandara E 889216220182841621310.1016/j.thromres.2017.04.003 · doi ↗ · pubmed ↗