Extra-skeletal Ewing sarcoma in a 63-year-old female with a history of triple-negative breast cancer: a case report and literature review
Man Kit Ho, Golnesa Safavi, Won Jin Jeon, Evelyn Mendoza

TL;DR
A 63-year-old woman with a history of breast cancer was diagnosed with rare extra-skeletal Ewing sarcoma after initial misdiagnosis.
Contribution
This case highlights the diagnostic challenges and management of EES in older adults with a cancer history.
Findings
EES was confirmed via RNA sequencing showing the EWSR1-FLI1 fusion gene.
The patient received neoadjuvant chemotherapy and tumor resection.
EES can occur in older patients, leading to potential misdiagnosis.
Abstract
Ewing sarcoma (ES), particularly Extra-skeletal Ewing sarcoma (EES), is a rare, aggressive tumor predominantly affecting adolescents and young adults, yet it can occur in older patients, leading to misdiagnosis and delay in treatment. The standard approach includes surgical resection, chemotherapy, and radiation therapy for unresectable disease. This case report presents a 63-year-old female patient with a history of triple-negative breast cancer, who was discovered to have a soft tissue tumor in the left medial thigh. Initially misdiagnosed as rhabdomyosarcoma, the diagnosis of EES was ultimately confirmed via RNA sequencing revealing the EWSR1-FLI1 fusion gene. She underwent neoadjuvant chemotherapy followed by radical resection of the tumor.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
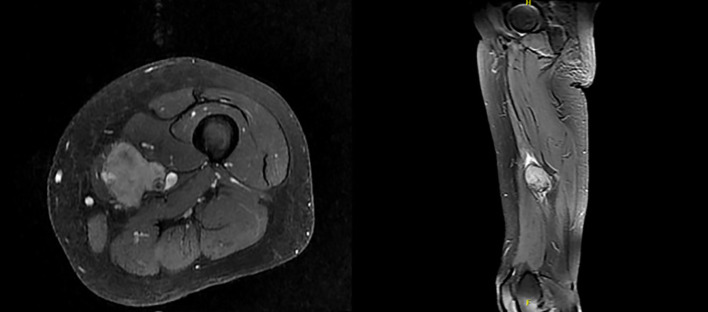 Figure 1
Figure 1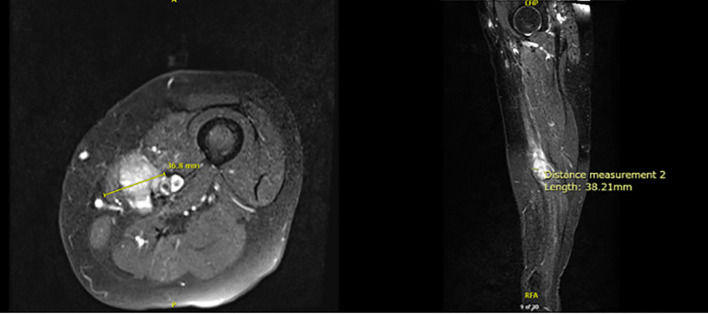 Figure 2
Figure 2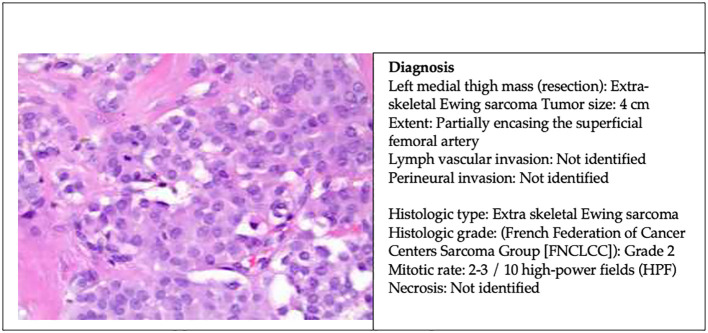 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoma Diagnosis and Treatment · Cardiac tumors and thrombi · Lymphoma Diagnosis and Treatment
Introduction
Ewing sarcoma (ES) is a highly aggressive tumor predominantly affecting the bones of adolescents and young adults (1). Extra-skeletal Ewing sarcoma (EES) is a rare soft tissue malignant tumor belonging to the Ewing sarcoma family of tumors (ESFT) that originates from unique mesenchymal progenitor cells (1). EES is ten times less common than skeletal ES, with an incidence of 0.4 per million, representing less than 5% of all soft tissue sarcomas (2, 3). While 95% of ES cases occur between ages of 4 and 25, EES is more frequently diagnosed in older adults, often presenting with a female predominance (1, 2, 4). This report highlights a case of EES initially misdiagnosed as rhabdomyosarcoma, ultimately confirmed through RNA sequencing with positivity of EWSR1-FLI1 fusion.
Case presentation
A 63-year-old woman presented to the oncology office in February 2024 with an enlarging mass in the left medial thigh. She reported no fever, bone pain, or joint pain. Her medical history included epilepsy and stage IIB triple-negative invasive ductal carcinoma of the right breast without gene mutation in 2020. She was treated with bilateral mastectomy with perioperative chemotherapy in 2021 including a total of 240 mg/m² of doxorubicin. Physical examination revealed a 5 x 5 cm subcutaneous, hard, and mobile mass in the left medial thigh.
An Ultrasound (US) in December 2023 indicated a markedly hypervascular solid lobulated 3.9 x 3.1 x 2.8 cm soft tissue mass in the mid inner left thigh, highly suspicious for malignancy tumor. In January 2024, a fine needle aspiration biopsy revealed malignant neoplasm without specific classification. A subsequent core biopsy suggested high-grade sarcoma with extensive necrosis, favoring rhabdomyosarcoma. However, RNA sequencing later confirmed EES with EWSR1::FLI1 fusion (Box 1). Further immunohistochemical (IHC) stains showed diffuse positivity for CD99 and 10% positivity for Ki67, while S100 protein and desmin were negative (Box 2).
Box 1Molecular study.Cancer-type relevant biomarkers.BiomarkerMethodAnalyteResultBiomarkerMethodAnalyteResult EWSR1
Seq
RNA-Tumor
Pathogenic Fusion EZH2SeqDNA-TumorMutation Not DetectedBRAFSeqDNA-TumorMutation Not DetectedFUSSeqRNA-TumorFusion Not DetectedMSISeqDNA-TumorStableHRASSeqDNA-TumorMutation Not DetectedMismatch Repair StatusIHCProteinProficient (Intact)IGF1RCNA-SeqDNA-TumorAmplification Not DetectedNTRK1/2/3SeqRNA-TumorFusion Not DetectedKRASSeqDNA-TumorMutation Not DetectedRETSeqRNA-TumorFusion Not DetectedMETSeqDNA-TumorMutation Not DetectedTumor Mutational BurdenSeqDNA-TumorLow, 5 mut/MbMYOD1SeqDNA-TumorMutation Not DetectedCDK4CNA-SeqDNA-TumorAmplification Not DetectedNF1SeqDNA-TumorMutation Not DetectedERBB2(HER2/Neu)SeqDNA-TumorMutation Not DetectedCNA-SeqDNA-TumorDeletion Not DetectedPAX3SeqRNA-TumorFusion Not DetectedNRASSeqDNA-TumorMutation Not DetectedPAX/SeqRNA-TumorFusion Not DetectedPIK3CASeqDNA-TumorMutation Not DetectedPD-L1 (SP142)IHCProteinNegative|0%TP53SeqDNA-TumorMutation Not DetectedPDGFRASeqDNA-TumorIndeterminateCNA-SeqDNA-TumorDeletion Not DetectedGenomic signatures.BiomarkerMethodAnalyteResultMicrosatellite instability (MSI):SeqDNA-TumorStableTumor Mutational Burden (TMB):SeqDNA-TumorLow (5)Genomic Loss of Heterozygosity (LOH):SeqDNA-TumorLow - 5%Genes tested with pathogenic or likely pathogenic alternations.GeneMethodAnalyteVariant interpretationProtein AlternationExonDNA AlternationVariant Frequency %EWSR1SeqRNA-TumorPathogenic FusionEWSR1-FLI1/––
Box 2Surgical pathology report of left inner thigh mass biopsy. Initial Surgical Pathology Report.
-
- HIGH-GRADE MALIGNANT NEOPLASM, FAVOR RHABDOMYOSARCOMA.
-
- EXTENSIVE NECROSIS PRESENT.
Amended Surgical Pathology Report.
-
- HIGH-GRADE SARCOMA, CONSISTENT WITH EXTRA-SKELETAL SARCOMA/PNET.
-
- EXTENSIVE NECROSIS PRESENT. Immunohistochemical Stain.IHC StainResultIHC StainResultAE1/AE3NegativeKi6710% PositiveS100 ProteinNegativeMyoD1Focally positiveCD20NegativeMyogeninNegativeSMANegativeCD138NegativeDesminNegativeCD99Positive
Magnetic Resonance Imaging (MRI) in January 2024 demonstrated a soft tissue mass measuring 4.3 x 3.2 x 6 cm, encasing the neurovascular bundle at the level of middle thigh, consistent with soft tissue sarcomatous mass (Figure 1). Fluorodeoxyglucose positron emission tomography (PDG-PET) indicated a hypermetabolic 5 cm mass in the left medial thigh without evidence of metastasis.
MRI of bilateral lower extremities with contrast in January 2024.
Neoadjuvant chemotherapy, comprising vincristine, doxorubicin, and cyclophosphamide, alternating with ifosfamide and etoposide, commenced in March 2024. Due to toxicity, the schedule was adjusted to every three weeks from every two weeks. Due to her prior treatment with doxorubicin for breast cancer, serial echocardiograms were conducted prior to each cycle of doxorubicin to monitor cardiac function. Additionally, she received dexrazoxane for cardioprotection prior to each dose of doxorubicin.
Following six cycles of neoadjuvant chemotherapy, MRI revealed a reduction in tumor size to 3.7 x 3.8 x 2.8 cm (Figure 2). Computed tomography (CT) Angiogram showed an avidly enhancing lesion within the left medial thigh measuring up to 2.8 cm with encasement/abutment of the femoral neurovascular bundle.
MRI of bilateral lower extremities with contrast in July 2024.
After eight cycles of chemotherapy, the patient underwent radical resection of left medial thigh sarcoma with en-bloc segmental resection of involved sartorius, superficial femoral artery, and saphenous nerve. The pathology report revealed a 4 cm extra-skeletal Ewing sarcoma with clear margin and partially encasing the superficial femoral artery (Figure 3). The patient has been recovering well postoperatively. A PET-CT scan in 6 months was scheduled to monitor the disease activity. She will be continued with six additional cycles of adjuvant chemotherapy for a total of 14 cycles and followed up with medical oncology, surgical oncology, and vascular surgery within 2 weeks postoperatively.
Surgical pathology report of left medial thigh mass resection.
Discussion
EES is part of the ESFT and is much less common than skeletal ES. Approximately 85% of cases of ES are linked to the chromosomal translocation t(11; 22)(q24; q12), which creates the EWSR1-FLI1 fusion gene, functioning as both a pioneering transcription factor and a potent oncogene (5). About 10% of cases involve the translocation t(21;22)(q22;q12), leading to the EWSR1-ERG fusion protein, an oncogenic transcription factor that inhibits apoptosis (1, 6, 7). The remaining 5% exhibit rare translocations, including t(7;22)(p22;q12), t(17;22)(q12;q12), and t(2;22)(q33;q12) within EWSR1-ETS (Ewing sarcoma breakpoint region 1 - E-twenty six transformation specific) family, as well as t(2;16)(q35:p11) and t(16;21)(p11;q22) within the FUS-ETS (Fused in sarcoma - E-twenty six transformation specific) family (7). No studies have demonstrated a higher incidence of Ewing sarcoma in patients with breast cancer, or vise versa. However, research by Gorthi et al. revealed a link between BRCA1 and Ewing sarcoma. They found that EWS-FLI1 increases transcription to cause R-loops and block BRCA1 repair, which mimics BRCA deficiency without genetic mutation (8).
An observational study in pediatric and adult patients indicates that patients with EES tend to be significantly older than those with skeletal ES. EES most commonly occurs in the trunk (75.9%), followed by the head and neck (10.3%) and lower extremities (10.3%) (9). In contrast, a meta-analysis focusing on pediatric cases found no significant age association with EES incidence (10). Among children, the thorax is the most frequent location (33%), with extremities following closely (31%) (11). The lungs are the most common distant metastasis site in both pediatric and adult EES patients (9, 12). Overall, the prognosis of EES is generally more favorable than skeletal ES. Several factors, such as the presence of metastasis, older age, pelvic involvement, elevated white blood cell counts, elevated lactate dehydrogenase (LDH), low hemoglobin, large tumor size at diagnosis, and poor histologic response to preoperative chemotherapy are associated with worse outcomes (2, 13–15).
The diagnosis of ESS is often delayed due to its non-specific clinical presentation, typically manifesting as rapidly progressive swelling at the tumor site, often accompanied by compression-related symptoms (16). While US, CT, and MRI can help with diagnosis and local staging, their imaging characteristics are non-specific. Nuclear bone scans or PET scans are recommended for detecting bone metastases. Definitive diagnosis relies on pathological, immunohistochemical, and molecular findings (1, 2, 4, 17). Microscopically, EES typically consists of monomorphic small round blue cells with large spherical nuclei, inconspicuous nucleoli, and indistinct cytoplasmic borders (2, 4). CD99, expressed in about 95% of ES, is a sensitive but poorly specific diagnostic marker for ES as it is also expressed in other round cell sarcomas and even leukemias (4, 7); ZETB16 has demonstrated even greater sensitivity. Recently, NKX2.2 has been identified as a target of EWS-FLI1 (18) and shows high specificity when combined with CD99 or ZETB16 (19). Ewing cells also express FLI-1, CD45, S-100 protein, synaptophysin, vimentin, and desmin (1, 2, 20).
Given the sensitivity and specificity of IHC in ES, most of the ES can be diagnosed with pathology and IHC. However, for the cases with atypical clinical and pathological presentations, molecular genetics testing via Fluorescence in-situ hybridization (FISH), reverse transcriptase - polymerase chain reaction (RT-PCR), and/or direct sequencing becomes crucial for the diagnosis (2, 4, 21). A tumor sample can be analyzed for the EWS-FLI1 and EWS-ERG fusions using RT-PCR or for the EWS-associated fusions via FISH (22).
According to National Comprehensive Cancer Network (NCCN), all members of the ESFT, including EES, follow the same treatment algorithm. Wide surgical resection is recommended to enhance survival rates (23). NCCN advises at least nine weeks of multiagent chemotherapy prior to local therapy, which can improve five-year survival rate from 5-10% to over 65% by eliminating micrometastases (23, 24). VDC-IE (vincristine, doxorubicin, and cyclophosphamide alternating with ifosfamide and etoposide) is recommended as the first line systemic chemotherapy regimen (23). A randomized trial reported that VDC-IE given on an every-2-week schedule is more effective than an every-3-week regimen without increased toxicity (25). Large clinical trials indicate that 14 to 17 cycles of chemotherapy yield favorable outcomes, encompassing both neoadjuvant and adjuvant therapy (26).
Although EES is radiosensitive, surgical resection should be prioritized whenever feasible, as it has shown superiority over definitive radiotherapy. Perioperative radiotherapy may be considered for resectable lesions with positive margins, while definitive radiotherapy is reserved for inoperable lesions. Further, palliative radiotherapy can be beneficial for symptomatic patients in certain situations (14, 23). Metastatic disease or unresectable recurrent disease should be managed similarly as localized ES, utilizing systemic chemotherapy and local control strategies (2, 23).
New therapeutic approaches, particularly targeted therapy, are urgently needed to improve outcome for advanced disease. Despite the EWS-FLI1 fusion protein driving ES oncogenesis, inhibition of these proteins themselves has proved challenging and clinically unsuccessful. Instead, those targeted therapies acting on the tumor microenvironment appear more promising (27, 28).
Conclusion
In this case report, our 63-year-old female patient was initially misdiagnosed with rhabdomyosarcoma in the lower extremity. However, RNA sequencing revealed the presence of the EWSR1-FLI1 fusion, confirming a diagnosis of EES, which necessitates a distinctly different treatment approach than that for rhabdomyosarcoma. Complicating her case further, the patient had previously received doxorubicin for triple-negative breast cancer, placing her at risk of exceeding the recommended maximum lifetime cumulative dose of 550 mg/m² (29). Despite the research indicates that Ewing sarcoma phenocopies BRCA1-deficient tumors, there is no study showed a direct connection between Ewing sarcoma and breast cancer. Given the significant mortality associated with metastatic EES, there remains an unmet need for biomarkers that can predict treatment response. Additionally, development of new therapeutic approaches, particularly targeted therapies, warrants further investigation to enhance the outcome for the patients with widely metastatic and refractory EES.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Durer S Gasalberti DP Shaikh H. Ewing sarcoma. In: Stat Pearls. Treasure Island (FL): Stat Pearls Publishing (2024).32644609 · pubmed ↗
- 2Abboud A Masrouha K Saliba M Haidar R Saab R Khoury N. Extraskeletal Ewing sarcoma: Diagnosis, management and prognosis. Oncol Lett. (2021) 21:354. doi: 10.3892/ol.2021.12615 33747211 PMC 7967932 · doi ↗ · pubmed ↗
- 3Bianchi G Laginestra MA Simonetti E Ibrahim T Macri F Ostetto F. Extraskeletal ewing sarcoma of the extremities and trunk: A retrospective analysis of a mono-institutional series. Oncol Res Treat. (2024) 47:496–508. doi: 10.1159/000540613 39084202 · doi ↗ · pubmed ↗
- 4Zollner SK Amatruda JF Bauer S Collaud Sde Alava E Du Bois SG. Ewing sarcoma-diagnosis, treatment, clinical challenges and future perspectives. J Clin Med. (2021) 10(8):1685. doi: 10.3390/jcm 10081685 33919988 PMC 8071040 · doi ↗ · pubmed ↗
- 5Riggi N Stamenkovic I. EWS-FLI-1 expression triggers a Ewing’s sarcoma initiation program in primary human mesenchymal stem cells. Cancer Res. (2008) 68:2176–85. doi: 10.1158/0008-5472.CAN-07-1761 18381423 · doi ↗ · pubmed ↗
- 6Riggi N Stamenkovic I. The biology of ewing sarcoma. Cancer Lett. (2007) 254:1–10. doi: 10.1016/j.canlet.2006.12.009 17250957 · doi ↗ · pubmed ↗
- 7Dupuy M Lamoureux F Mullard M Postec A Regnier L Baud'huin M. Ewing sarcoma from molecular biology to the clinic. Front Cell Dev Biol. (2023) 11:1248753. doi: 10.3389/fcell.2023.1248753 37752913 PMC 10518617 · doi ↗ · pubmed ↗
- 8Gorthi A Romero JC Loranc E Cao L Lawrence LA Goodale E. EWS-FLI 1 increases transcription to cause R-loops and block BRCA 1 repair in Ewing sarcoma. Nature. (2018) 555:387–91. doi: 10.1038/nature 25748 PMC 631812429513652 · doi ↗ · pubmed ↗