Risk factors for ocular graft-versus-host disease: A systematic review and meta-analysis
Yuanyuan Wang, Yuan Min, Yanfei Sun, Mengxin Xue, Feng Li

TL;DR
This study identifies risk factors for eye-related complications after stem cell transplants, helping doctors spot high-risk patients early.
Contribution
A systematic review and meta-analysis to clarify risk factors for ocular graft-versus-host disease after allogeneic stem cell transplants.
Findings
Elderly patients and female donors are associated with higher oGVHD risk.
Chronic graft-versus-host disease significantly increases the likelihood of oGVHD.
Peripheral hematopoietic stem cells and matched-relative donors are linked to higher oGVHD prevalence.
Abstract
AIM Allogeneic hematopoietic stem cell transplantation (allo-HSCT) is an important treatment for blood disease, and ocular graft-versus-host disease (oGVHD) is a common complication that significantly affects the quality of life of patients. Currently, the risk factors for oGVHD are still controversial.Methods To provide a scientific foundation for the prevention of oGVHD in patients undergoing allo-HSCT, studies on the factors influencing the development of oGVHD were searched in PubMed, Embase, Web of Science, Sino Med, the Cochrane Library, CIKI, the Wanfang Database, and the VIP Database from database construction to May 2024.Results Seventeen studies included 4,501 patients who received allo-HSCT, of which 1,526 were diagnosed with oGVHD, involving 22 factors. The overall prevalence of oGVHD was 37.8%.[95% CI (0.294, 0.463)].The prevalence of oGVHD based on the diagnostic criteria…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
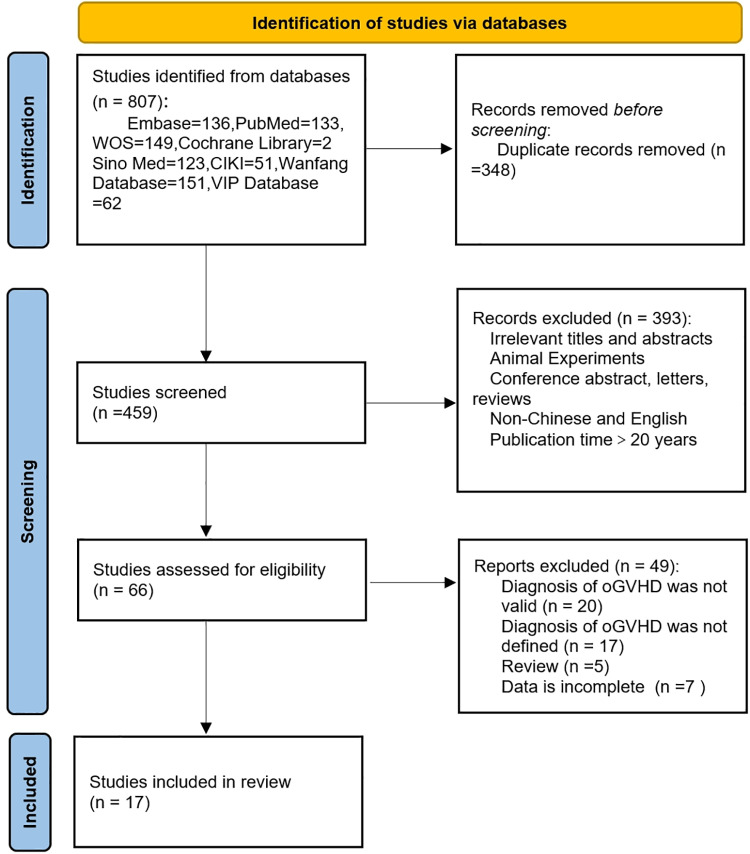 Fig 1
Fig 1- —http://dx.doi.org/10.13039/100014718Innovative Research Group Project of the National Natural Science Foundation of China
- —Jingling hospital
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCorneal Surgery and Treatments · Ocular Surface and Contact Lens · Hematopoietic Stem Cell Transplantation
Introduction
Allogeneic hematopoietic stem cell transplantation (allo-HSCT) is an important treatment for blood system diseases. By the end of 2023, there would have been 14,551 transplant patients in China, with an 88% transplant success rate, indicating an increasing trend, according to statistics [1]. The most prevalent side effect following allo-HSCT is graft-versus-host disease (GVHD), which can be acute or chronic [2,3]. GVHD has become more common as allo-HSCT technology has been used and developed. The incidence of GVHD is estimated to be between 30% and 70%. Ocular graft-versus-host disease (oGVHD) develops in 60–90% of patients following allo-HSCT. It typically manifests as part of chronic GVHD (cGVHD) [4], occurs less frequently in acute graft-versus-host disease (aGVHD), and is associated with poor overall survival in patients after transplantation. The hallmark symptom of oGVHD is T-cell-mediated inflammatory damage, which results in dry eye (DE), cicatricial conjunctivitis, and dry keratoconjunctivitis [5]. The majority of these symptoms are accompanied by lifelong visual impairment. Patients’ everyday activities and quality of life are severely impacted by these irreversible visual impairments [2,6]. oGVHD merits greater consideration in light of the growing societal focus on transplant recipients' quality of life [7,8].
The causes of oGVHD are not widely discussed at present, and the findings of the scant published research are contradictory [9]. Meta-analysis constitutes a cornerstone methodology in evidence-based medicine, employing quantitative statistical techniques to systematically synthesize and evaluate outcomes from multiple independent studies addressing congruent research objectives. This analytical paradigm transforms fragmented empirical observations into clinically actionable high-level evidence while resolving epistemic discrepancies through quantitative synthesis [10]. Thus, the purpose of this study was to explore the risk factors for oGVHD via a systematic review and meta-analysis to identify and screen high-risk patients early and reduce the occurrence of oGVHD.
Materials and methods
Databases and search strategy
As required by the PRISMA declaration, our investigation was appropriately registered on the PROSPERO portal (CRD42024566501). The search strategy was developed on the basis of the following research content: (1) terms related to graft-versus-host disease or ocular graft-versus-host disease; (2) terms related to the eye; and (3) terms related to risk factors, in the form of a combination of subject terms and free words, and the finalized search terms were graft-versus-host disease/dry-eye syndrome/risk factors. Searches were performed on PubMed, Embase, Web of Science, Sino Med, the Cochrane Library, CIKI, the Wanfang Database, and the VIP Database. The initial search was conducted on May 10, 2024, and the PubMed search strategy is shown in Table 1.
Table 1: Strategy for searching the literature in the PubMed database.
Data extraction and quality assessment
Two researchers independently read all titles and abstracts and screened the literature using the inclusion/exclusion criteria. The inclusion criteria were as follows: (1) a clear definition of oGVHD; (2) oGVHD as an outcome indicator and a discussion of its influencing factors; and (3) all the original quantitative studies were considered. The exclusion criteria were as follows: (1) animal experiments; (2) conference papers or reviews; (3) non-Chinese or English literature; (4) did not extract valid data; and (5) publication time >20 years. The included literature was read in its entirety, with information retrieved, such as authors, year, region, sample size, diagnostic criteria, influencing factors, effect values, and confidence intervals. If a consensus could not be reached, it was confirmed by a third researcher.
Cohort studies were evaluated for quality via the Newcastle‒Ottawa Scale (NOS). The NOS scale is divided into 3 dimensions with 8 items. Low-risk entries are assigned 1 star up to a maximum of 9 stars, and 0--3, 4--6, and 7--9 stars are considered low-, medium- and high-quality studies, respectively [11]. Cross-sectional studies were evaluated for quality via the American Agency for Healthcare Quality and Research (AHRQ) scale, which consists of 11 items. Each entry can be answered with “yes” or “no”, with “yes” receiving one point and “no” or “unclear” receiving no points. A score of 11 was assigned, with 0--3, 4--7, and 8--11 points for low-, medium-, and high-quality studies, respectively [12].
Statistical methods
Stata 16.0 was utilized for the statistical analysis. The effect markers for dichotomous variables were the odds ratio (OR) or hazard ratio (HR) and the 95% confidence interval (CI). Heterogeneity was determined by the χ2 test; if P < 0.10 and I^2^ > 50%, the studies were considered significantly heterogeneous, and a random effects model was used; otherwise, a fixed effects model was used. Differences were considered statistically significant if P < 0.05. Sensitivity analyses were conducted by replacing the random and fixed effects models to compare the robustness of the combined results of the two models, and the “leave-one-out” method was used to exclude one study from each of the influencing factors of >3 included studies to reassess the change in the overall effect. According to the recommendations of the Cochrane Evidence-Based Guidelines, for fewer than 10 included studies, funnel plots were used to visually assess publication bias. For subgroups containing 10 or more studies, publication bias was statistically evaluated using Egger's linear regression test, with the significance level set at P < 0.05.
Results
Literature screening
While 348 duplicates were removed from the 807 articles found in the preliminary literature search, 459 articles—175 in Chinese and 284 in English—were found in the first screening. After screening the titles and abstracts of 459 papers, 66 were selected for full-text reading, and 17 documents that satisfied the requirements were ultimately included. Fig 1 illustrates the specific screening procedure.
PRISMA 2020 flow diagram for systematic reviews.
Basic information and quality assessment results
The seventeen studies, comprising three prospective cohort studies, nine retrospective cohort studies, and five cross-sectional studies, are listed in Table 2 along with their respective features. Of these, six studies were of moderate quality, and eleven were of high quality; the findings of the meta-analysis were largely reliable. The quality assessment results of this systematic review are presented in Tables 3 and 4. The studies included thirteen districts with a sample size of 4,480 people, and a total of twenty-two factors associated with the occurrence of oGVHD were extracted. Owing to the different results of the studies, some factors were considered relevant in some studies and irrelevant in others, which were included in the same group for analysis. The factors numbered ①--⑯ were reported in ≥2 studies, and the remaining six factors were reported in only one study; therefore, they were not included in the meta-analysis, as described in the discussion.
Table 2: Basic characteristics of the included studies.
Table 3: Quality assessment ratings for cross-sectional studies.
Table 4: Results of quality assessment of cohort studies.
Impact factor effect value analysis
Meta-analysis of the combined effect values of the influencing factors reported in ≥2 studies led to the conclusion that elderly age, female sex, matched-relative donor (MRD), peripheral hematopoietic stem cell (PBSC) count, and occurrence of aGVHD, cGVHD, and oral and skin GVHD were risk factors for the development of oGVHD (P < 0.05). The combined effect values for each factor are detailed in Table 5.
Table 5: Results of heterogeneity test and meta-analysis of oGVHD influencing factors.
Prevalence of oGVHD
A total of 4,501 patients were included in this study, of whom 1,526 were diagnosed with oGVHD, and the incidence of oGVHD was 37.8% [95% CI (0.294, 0.463), I^2^ = 98.0%, P = 0.000], which is highly heterogeneous, so subgroup analyses were performed on the basis of diagnostic criteria. Among the seventeen studies, two provided data on both the NIH and ICCGVHD diagnostic criteria, so were included by both subgroups. Seven studies used self-defined diagnostic criteria, and the incidence of oGVHD was 32.0% [95% CI (0.184, 0.457)]. Seven studies used the NIH-recommended diagnostic criteria, and the incidence of oGVHD was 46.7% [95% CI (0.390, 0.545)]. Five studies used the diagnostic criteria recommended by the ICCGVHD, with an oGVHD incidence of 33.7% [95% CI (0.167, 0.506)]. All the subgroups presented a high degree of heterogeneity.
Sensitivity analysis
Table 6 shows the results of using two different models for each factor. With the exception of diabetes mellitus, steroid medication, and SIT < 10 mm/5 min, all 16 factors of interest showed a high degree of concordance in the total effect sizes, suggesting that the results were typically stable. The results of the Leave-One-Out method (see S19–S30 Figs in S2 File) show that all fall within the confidence intervals.
Table 6: Two different models for influencing factors.
Bias analysis
When the incidence of oGVHD in 17 studies was examined, the results of Egger’s test revealed that there was not publication bias (t = 1.05, P = 0.308), the results are shown in S18 Fig in S2 File. And the funnel plots of factors also revealed some evidence of publication bias. Maybe attributable to notable variations across studies in temporal scope, geographical distribution, and study design, combined with insufficient sample sizes – factors likely representing the primary sources of heterogeneity.
Discussion
The proportion of patients who survive allo-HSCT has been increasing as medicine has advanced. Even while oGVHD is not the primary cause of death for patients, it may decrease patients' quality of life and exacerbate a number of burdens from psychological and physical sources [29]. As a result, it is critical to research, assess, and mitigate the risk factors for oGVHD. The two most widely used diagnostic criteria for oGVHD are now advocated by the ICCGVHD and the NIH, as there are currently no standardized criteria for the diagnosis of this condition [30,31]. In certain preliminary investigations, researchers typically make a diagnosis. The incidence of oGVHD in this study was 46.7% according to the NIH diagnostic criteria, which is comparable to that reported in a recent cohort [18]. The current study slightly lessened the diagnostic criteria for ICCGVHD. The variability in the results may be related to the insufficient number of included studies, large differences in population characteristics, and different timings of observations.
According to a prospective study [32], age is a crucial factor to consider when transplanting. Aging increases the risk of DE and modifies the structure of the eye [33]. In this study, older patients were more likely to experience oGVHD following transplantation (P = 0.044). Gender also had a significant effect. These findings indicate a link between the onset of oGVHD and female donors. This may be caused by the homozygous immunological reaction that follows the identification of the Y chromosome and results in organic damage [34]. This has led some researchers to hypothesize that donor‒recipient sex matching can prevent the development of oGVHD [18]. These findings are consistent with those of earlier research on cGVHD [18,35]. However, this component was not statistically significant in this study (P = 0.873).
For allo-HSCT to be effective, donor T cells must undergo a graft-versus-tumor response. Since we believe that donor selection is associated with oGVHD, this study examined the donor‒recipient connection from several perspectives. The findings revealed that patients who selected MRD had a greater frequency of oGVHD than did those who selected an unrelated donor and that kinship was associated with oGVHD. This outcome can be explained by variations in the patients' pretreatment regimens and immunosuppressive medications, with patients who opt for MRD typically using milder regimens [18]. The current study, however, demonstrated that the impact of blood type incompatibility between donors and recipients progressively diminished and was not a significant predictor of oGVHD (P = 0.515). Bone marrow (BM), cord blood, or peripheral blood are the usual sources of donor cells. The use of PBSCs has increased dramatically as a result of their benefits over BM, which include simple collection, less cell contamination, and quicker implantation [36]. Nonetheless, the use of PBSCs increases the incidence of cGVHD [37,38]. The significantly greater concentration of T cells and CD34 + cells in the PBSC grafts than in the BM grafts may be the cause of this connection [3]. Additionally, patients who receive BM as grafts have better psychological status and prognoses, which helps them return to work [39]. The choice of PBSCs as grafts is a substantial risk factor for oGVHD, and this investigation confirms that conclusion (P = 0.000). Given the limited selection, the influencing factors associated with the objective conditions of the receptor supply cannot be changed or directly intervened, and the clinician can do more by paying attention to the appearance of the patient's eye symptoms and detecting oGVHD as early as possible.
Prior to receiving a donor cell transfusion, patients must be pretreated. This is a crucial tool for GVHD prophylaxis and consists of several chemotherapy regimens, the majority of which are coupled with TBI [40]. According to several theories [41], TBI damages the lacrimal gland, which can result in DE. Steroids are anti-inflammatory and pro-apoptotic, but because they can cause a variety of infectious and noninfectious problems, their prolonged use should be avoided [42]. Pretreatment regimens that minimize pretreatment-related toxicity while promoting implantation and reducing GVHD incidence have been optimized in recent years [43]. TBI and steroid therapy were not significant risk factors for oGVHD in the current investigation.
Among the studies [14,16,20,26] we analyzed, researchers discussed the impact of various conditioning regimens (e.g., immunosuppressants or chemotherapeutic agents) on oGVHD. Despite protocol variations, all studies consistently concluded that this factor showed no significant association with oGVHD.
We propose that oGVHD and systemic GVHD may share immunopathological mechanisms. Research indicates a robust correlation between the onset of oGVHD and systemic GVHD [18]. Similarly, patients with prior aGVHD (P = 0.000) and cGVHD (P = 0.000) had an increased risk of oGVHD in our study. When systemic GVHD occurs in patients, it indicates that the immune response may be widespread across multiple organs, including the skin, liver, gastrointestinal tract, etc. Patients with a history of oral and cutaneous GVHD are more prone to develop eyelid margin lesions [44] because the inner surface of the catheter is made of mucosa [16,45] and is frequently targeted by T cells or other inflammatory cells.
The results indicate that the likelihood of developing eyelid edge lesions is greater in both acute and chronic cases. The findings demonstrated that the development of oGVHD in both the acute and chronic phases was linked to both cutaneous (P = 0.000) and oral (P = 0.000) GVHD. Ocular surface damage is caused by gastrointestinal and hepatic GVHD, according to certain studies [45], and thus increases the likelihood of developing oGVHD. Furthermore, it has been suggested that the quantity of organs involved may play a significant role in ocular involvement [16]. This suggests that the ocular surface—a region with weaker immune privilege—is more vulnerable to attack, as systemic immune reactions can directly target this site. Ocular pathological changes represent a local manifestation of systemic immune dysregulation rather than isolated events. Therefore, controlling systemic GVHD is the central strategy for preventing and treating ocular complications.
Unexpectedly, oGVHD may manifest before other tissues and organs, and rejection responses to the eye and other organs may be mutually causal, mutually encouraging, and lead to malignant cycles. To prevent the onset of GVHD, we must thus provide patients with various systemic host-resistant illnesses with more care while providing effective therapy and symptom management. However, it is noteworthy that in the report by ZHUANG [45], approximately 6% of patients exhibited ocular symptoms without rejection reactions in other organs, suggesting that the development of oGVHD may precede pathological manifestations in other tissues and organs. The driving mechanisms linking systemic GVHD and oGVHD require further investigation.
There is ongoing debate concerning a few of the oGVHD-related variables. In contrast to the findings of HÉBERT et al. [21], Na et al. [16] reported that hyperglycemia affects the function of the ocular surface immune response and proposed that a history of diabetes is a risk factor for the development of oGVHD. A prospective investigation revealed that increasing the humidity level in the ward is a successful preventive strategy [46]. According to research by Jay et al. [9], being white may help prevent oGVHD. Nevertheless, more thorough evidence does not bolster these theories.
Limitations
There are several limitations to this study. First, this field contains multiple knowledge gaps where research findings remain fragmented. There is not much prospective evidence, the study is mostly retrospective. Second, although our model demonstrates reasonable stability, variations in confounding factors may predispose the analysis toward individual-level effects rather than population-level considerations—an unavoidable bias inherent to small-sample investigations and the primary source of heterogeneity in this study. Consequently, caution is warranted when interpreting these findings. Third, standardized baseline ophthalmic examinations are generally lacking for hematologic patients, with current diagnostic practices predominantly relying on patient-reported symptoms or observable early clinical manifestations. Fourth, among the validated risk factors for oGVHD in this study are non-modifiable objective conditions, which inherently limit the clinical controllability and practical applicability of the conclusions. Furthermore, most existing studies have inadequately addressed potential pre-existing ocular comorbidities or systemic conditions in their study populations. Notably, none of the currently included studies have systematically examined these adjustable parameters. Future research should prioritize investigation of modifiable factors such as treatment protocols, pharmacological agents, and laboratory biomarkers in relation to oGVHD development.
Conclusion
Research has revealed that the risk factors for oGVHD include the incidence of aGVHD, cGVHD, oral and skin GVHD, female donors, MRD, PBSC, and elderly patients. Through systematic meta-analysis, we achieved synthesis of existing evidence. Despite methodological limitations inherent to the restricted number of primary studies, this work successfully established a robust knowledge framework. Our findings not only provide researchers with a reference for evidence grading, but more critically, by identifying evidence gaps and proposing optimized research directions, lay a theoretical and hypothesis-driven foundation for future high-quality investigations involving large-scale cohorts and multi-center validation trials. To provide a more pertinent and rigorous scientific evidence-based clinical basis, hematologists and ophthalmologists must collaborate to perform high-quality, multicenter, large-sample studies in the future. Clinicians can create oGVHD prediction models for patient risk assessment on the basis of the findings of this study. Targeted baseline ophthalmologic examination, early identification of high-risk patients, health promotion, and follow-up were performed. Improving oGVHD-related visual loss or significant eye damage is essential for improving patient prognosis and posttransplant quality of life.
Supporting information
S1 FileList of raw analysis data.(XLSX)
S2 FileData analysis and results.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chinese bone marrow repository. Annual Report of the China Bone Mental Fund for 2022 [EB/OL]. 2023. [cited 2024 May 10]. Available from: https://www.cmdp.org.cn/show/1080031.html
- 2Altan-Yaycıoğlu R, Aydın Akova Y, Dönmez O. Age-related differences in the clinical patterns of ocular graft-versus-host disease. Turk J Ophthalmol. 2022;52(6):366–73. doi: 10.4274/tjo.galenos.2022.50945 36578178 PMC 9811231 · doi ↗ · pubmed ↗
- 3Jeppesen H, Sengeløv H, Eriksson F, Kiilgaard JF, Andersen ST, Lindegaard J, et al. Chronic ocular graft-versus-host disease after allogeneic haematopoietic stem cell transplantation in Denmark – factors associated with risks and rates in adults according to conditioning regimen. Bone Marrow Transplant. 2020;56(1):144–54. doi: 10.1038/s 41409-020-0993-332655136 · doi ↗ · pubmed ↗
- 4Pellegrini M, Bernabei F, Barbato F, Arpinati M, Giannaccare G, Versura P, et al. Incidence, risk factors and complications of ocular graft-versus-host disease following hematopoietic stem cell transplantation. Am J Ophthalmol. 2021;227:25–34. doi: 10.1016/j.ajo.2021.02.022 33626365 · doi ↗ · pubmed ↗
- 5Jeppesen H, Gjærde LK, Lindegaard J, Julian HO, Heegaard S, Sengeløv H. Ocular chronic graft-versus-host disease and its relation to other organ manifestations and outcomes after allogeneic hematopoietic cell transplantation. Transplant Cell Ther. 2022;28(12):833.e 1-833.e 7. doi: 10.1016/j.jtct.2022.08.016 36002105 · doi ↗ · pubmed ↗
- 6Kitko CL, Pidala J, Schoemans HM, Lawitschka A, Flowers ME, Cowen EW, et al. National institutes of health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I Ia. The 2020 clinical implementation and early diagnosis working group report. Transplant Cell Ther. 2021;27(7):545–57. doi: 10.1016/j.jtct.2021.03.033 33839317 PMC 8803210 · doi ↗ · pubmed ↗
- 7Chang Y-J, Pei X-Y, Huang X-J. Haematopoietic stem-cell transplantation in China in the era of targeted therapies: current advances, challenges, and future directions. Lancet Haematol. 2022;9(12):e 919–29. doi: 10.1016/S 2352-3026(22)00293-9 36455607 · doi ↗ · pubmed ↗
- 8Wang X, Huang R, Zhang X, Zhang X. Current status and prospects of hematopoietic stem cell transplantation in China. Chin Med J (Engl). 2022;135(12):1394–403. doi: 10.1097/CM 9.0000000000002235 35866344 PMC 9481431 · doi ↗ · pubmed ↗