Bilateral pulmonary parenchymal metastasis from a low-grade appendiceal mucinous neoplasm
John D M Cavaye, Bree D Stephensen, Jeffrey B Macemon

TL;DR
A rare case of lung metastasis from a slow-growing appendix tumor is reported, highlighting the need for chest imaging in follow-up care.
Contribution
This case highlights the rare occurrence of distant metastasis from low-grade appendiceal tumors without local spread.
Findings
A 50-year-old patient had bilateral lung metastasis from a 12-year-old appendix tumor.
Metastasis occurred without evidence of local or peritoneal spread.
The case suggests chest imaging may be important in surveillance protocols.
Abstract
Low-grade appendiceal mucinous neoplasms, are the most common precursor lesions to pseudomyxomatous peritonei. They are relatively indolent in nature, with a “pushing” style of invasion. We present a case of a 50-year-old gentlemen who underwent staged video assisted thoracoscopic surgery for bilateral pulmonary metastasis secondary to a low-grade appendiceal mucinous neoplasm that had been resected 12 years prior. We highlight the under recognized rare etiology of distant metastasis without evidence of local spread, and therefore whether imaging of the chest should be considered as part of the surveillance protocol.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
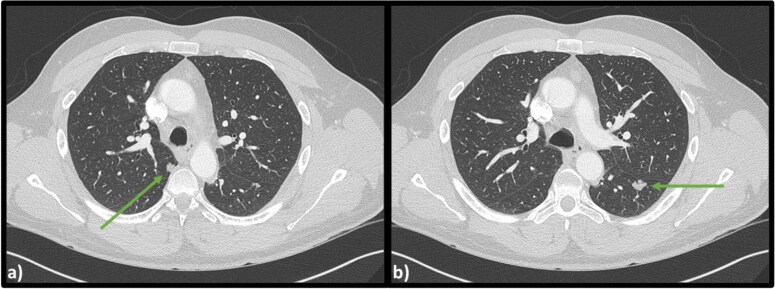 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntraperitoneal and Appendiceal Malignancies · Appendicitis Diagnosis and Management · Ovarian cancer diagnosis and treatment
Introduction
Appendiceal mucinous neoplasm (AMN) is a rare tumor arising from the appendix, found in <1% of appendicectomy specimens [1]. Originally described in 2003, they are characterized by a dilated and mucin filled appendix [2]. These tumors can further be classified as low-grade appendiceal mucinous neoplasm (LAMN) or high-grade appendiceal mucinous neoplasm (HAMN) based on cytological atypia and presence of infiltrative invasion [3]. LAMNs are the most common precursor lesions to pseudomyxoma peritonei (PMP), which occurs secondary to local infiltration, primarily after appendiceal perforation.
PMP is defined by its presence of mucinous ascites, peritoneal implants and omental caking [3]. Despite its slow progression, it causes debilitating symptoms and is ultimately fatal if left untreated, therefore, it is commonly treated with cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) [4].
Appendicectomy has commonly been the mainstay of treatment for LAMNs, with complete excision deemed curative. Higher staged lesions are then often surveilled to detect early progression to PMP [5, 6]. Classically, LAMN has been defined to have an inability to metastasise to distant areas of the body, secondary to its ‘pushing’ style of invasion [2]. Despite this, scarce literature reports have identified distant pulmonary metastasis, secondary to a LAMN [7–11].
We present a case of metastatic pleuropulmonary LAMN, 12 years after initial appendicectomy.
Case report
A 50-year-old Caucasian male presented to the emergency department with chest wall pain after an accidental fall off his roof. Examination elicited no obvious injuries at time of his presentation, with normal vital signs. He had a background of laparoscopic appendicectomy followed by right hemicolectomy for synchronously identified appendiceal carcinoid tumor and mucocoele 12 years prior. His follow up ceased after he moved interstate to his current location.
Computed tomography (CT) scans revealed no injuries, however bilateral lobulated lower lobe pulmonary masses were identified measuring 15 × 11 × 14 mm on the left and 9 × 10 × 10 mm on the right (Fig. 1).
Axial CT scan of the chest indicating (a) lobulated lesion in apical segment of right lower lobe (9 × 10 × 10 mm) and (b) secondary lobulated lesion present in left lower lobe (15 × 11 × 14 mm).
Respiratory function tests were normal, with a negative cryptococcus antigen. CT guided biopsy of his left lower lobe lesion was consistent with a low-grade mucin-producing tumor. It was likely this lesion was a metastasis from his previous appendiceal mucocele, and staged operative intervention to remove both pulmonary lesions was undertaken. Video assisted thoracoscopic surgery (VATS) resection of the left lower lobe superior segment revealed a well-circumscribed deposit of low-grade mucinous neoplasm. Histology comparing the pulmonary lesion with the original appendicectomy confirmed matching pathological appearance. Based on current nomenclature, his initial appendicectomy lesion would be defined as a LAMN with perforation, pT4b. Further right sided lower lobe superior segment pulmonary resection confirmed identical LAMN histology. The patient has since been discharged from hospital and has made a full recovery.
Discussion
Cases of parenchymal pulmonary metastasis from appendiceal mucinous lesions are rare, first reported in 1962 where pulmonary metastasis from an appendiceal mucocele was identified post-mortem [7]. Mortman et al. later published three patients with pulmonary disease secondary to a mucinous lesion [8]. Two of these patients had appendiceal lesions that would be today classified as LAMN, and all three had evidence of disseminated abdominal PMP [8]. Further cases have been reported of parenchymal pulmonary lesions identified in patients that had previously undergone cytoreductive surgery for PMP [9, 10].
Appropriately, since 1962, the nomenclature to define such mucinous appendiceal lesions has evolved to the current tiered structure. The current system classifies mucinous lesions on a spectrum from LAMN through to invasive adenocarcinoma, based on features of invasion, cytological atypia and presence of signet ring cells [3]. However, in cases where low-grade lesions can metastasise distantly, authors have queried whether these cases are in fact adenocarcinomas due to the added threat they pose [8–10].
Most recently, Zhao et al. reported a case of LAMN with pulmonary metastasis at time of diagnosis [11]. The pulmonary lesion was initially diagnosed as an adenocarcinoma, however, next generation sequencing confirmed it had identical tumor mutations to the LAMN identified post hemicolectomy [11]. Notably, like our patient, their case had no evidence of disseminated PMP alongside the pulmonary disease. Our case supports this literature in identifying distant metastasis without evidence of localized “pushing” invasion. This may indicate that LAMNs have a potential for hematogenous spread, especially given our case demonstrates bilateral spread of disease. However, more investigation is required to identify the true propensity and mechanism in which these lesions manage to metastasize distantly.
Our case highlights the potential for disease metastasis long after initial diagnosis, suggesting more rigorous surveillance strategies for patients diagnosed with a LAMN need to be considered. There is limited consensus on appropriate guidelines to establish surveillance post LAMN diagnosis [5, 6, 12]. Two separate institutions have published their guidelines for postoperative surveillance using biochemical tumor markers alongside repeat abdominopelvic CT scans to assess for extension to PMP. Due to the risk of pulmonary metastasis, we recommend chest CT be added to surveillance protocols in patients with high-risk initial disease. To our knowledge, this is the first case of bilateral pulmonary metastasis from a LAMN.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Smeenk RM, van Velthuysen MLF, Verwaal VJ, et al. Appendiceal neoplasms and pseudomyxoma peritonei: a population based study. Eur J Surg Oncol J Eur Soc Surg Oncol Br Assoc Surg Oncol 2008;34:196–201. 10.1016/j.ejso.2007.04.00217524597 · doi ↗ · pubmed ↗
- 2Misdraji J, Yantiss RK, Graeme-Cook FM, et al. Appendiceal mucinous neoplasms: a clinicopathologic analysis of 107 cases. Am J Surg Pathol 2003;27:1089–103. 10.1097/00000478-200308000-0000612883241 · doi ↗ · pubmed ↗
- 3Carr NJ, Cecil TD, Mohamed F, et al. A consensus for classification and pathologic reporting of pseudomyxoma peritonei and associated appendiceal neoplasia: the results of the Peritoneal Surface Oncology Group International (PSOGI) modified Delphi process. Am J Surg Pathol 2016;40:14–26. 10.1097/PAS.000000000000053526492181 · doi ↗ · pubmed ↗
- 4Rizvi SA, Syed W, Shergill R. Approach to pseudomyxoma peritonei. World J Gastrointestinal Surg 2018;10:49–56. 10.4240/wjgs.v 10.i 5.49PMC 612100130190782 · doi ↗ · pubmed ↗
- 5Hannan E, Roman LM, O'Brien L, et al. Surveillance of low-grade appendiceal mucinous neoplasms for progression to pseudomyxoma peritonei: results from a structured surveillance programme. Colorectal Dis 2025;27:e 17266. 10.1111/codi.17266 PMC 1168316339690127 · doi ↗ · pubmed ↗
- 6Campana LG, Wilson MS, Halstead R, et al. The need for tailored posttreatment surveillance for low-grade appendiceal mucinous neoplasms (LAMN). J Surg Oncol 2022;125:317–9. 10.1002/jso.2670234719029 · doi ↗ · pubmed ↗
- 7“Mucocele appendicis” with pseudomyxoma peritonei and pulmonary metastases. Acta Pathologica Microbiologica Scandinavica 1964;60:483–6.10.1111/apm.1964.60.4.48314154710 · doi ↗ · pubmed ↗
- 8Mortman KD, Sugarbaker PA, Shmookler BM, et al. Pulmonary metastases in pseudomyxoma peritonei syndrome. Ann Thorac Surg 1997;64:1434–6. 10.1016/S 0003-4975(97)00806-09386716 · doi ↗ · pubmed ↗