Acute-Subacute Paracoccidioidomycosis
Carlos McFarlane, Omayra Chincha, Carlos Seas

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
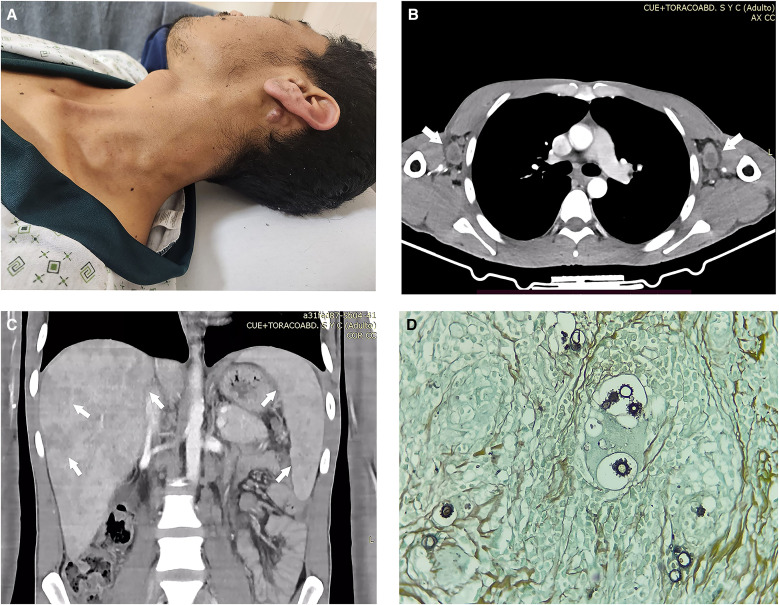 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFungal Infections and Studies · Nail Diseases and Treatments
A 29-year-old male farmer from Yambrasbamba, Amazonas, in the Amazon rainforest in Peru presented with a 4-month history of cervical lymphadenopathy, persistent fever, jaundice, weight loss, abdominal pain, and malaise. Physical examination revealed multiple mobile and painless lymph nodes in the submental, submandibular, and cervical chains (Figure 1A). Jaundice and hepatosplenomegaly were present. Laboratory tests showed microcytic hypochromic anemia (hemoglobin: 9 g/dL), leukocytosis (15,600 cells/mm^3^) with lymphocytosis (neutrophils 35.8%, eosinophils 0.5%, basophils 0.8%, monocytes 2.2%, and lymphocytes 60.7%), elevated alkaline phosphatase (1,177 U/L), and elevated total bilirubin (14 mg/dL; direct bilirubin 12.6 mg/dL). Serologies for HIV, human T-lymphotropic virus-1, syphilis, hepatitis C, and hepatitis B were negative. A chest computed tomography (CT) scan revealed cervical and axillary lymphadenopathy without pulmonary involvement (Figure 1B). Abdominal CT showed hepatosplenomegaly with multiple liver and spleen abscesses and enlargement of mesenteric lymph nodes (Figure 1C). Histopathology of a cervical lymph node biopsy demonstrated chronic granulomatous inflammation with abundant giant cells. Periodic acid–Schiff and Grocott methenamine silver stains confirmed the presence of fungal structures consistent with Paracoccidioides species (Figure 1D). The patient was initially treated with amphotericin B deoxycholate for 2 weeks, followed by trimethoprim-sulfamethoxazole at discharge. By that time, the fever, abdominal pain, and malaise had resolved. Partial improvement in jaundice was observed, with a reduction in alkaline phosphatase levels (821 U/L) and total bilirubin (3.3 mg/dL). This presentation corresponds to the acute-subacute form (AF) of paracoccidioidomycosis, also known as the juvenile form, characterized by rapid onset of symptoms. Clinical manifestations are related to the involvement of the mononuclear phagocytic system, with lymphadenopathies in superficial and/or deep lymph nodes being the most common presentation. Although typically associated with younger individuals, the AF can also occur in adults and is usually severe because of the rapid progression of the disease and significant involvement of the mononuclear system, leading to a marked depression of cell-mediated immune response.1^,^2
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Peçanha PM Peçanha-Pietrobom PM Grão-Velloso TR Rosa Júnior M Falqueto A Gonçalves SS, 2022. Paracoccidioidomycosis: What we know and what is new in epidemiology, diagnosis, and treatment. J Fungi (Basel) 8: 1098.36294662 10.3390/jof 8101098 PMC 9605487 · doi ↗ · pubmed ↗
- 2Hahn RC Hagen F Mendes RP Burger E Nery AF Siqueira NP Guevara A Rodrigues A Mde Camargo ZP, 2022. Paracoccidioidomycosis: Current status and future trends. Clin Microb Rev 35: e 0023321.10.1128/cmr.00233-21PMC 976969536074014 · doi ↗ · pubmed ↗