Case Report: Diagnostic overlap of OHVIRA syndrome and Gartner duct cyst: challenges in imaging and management
Junfeng Zhao, Yaqing Bao, Linglu Gong, Zhan Shi, Xiaoqiang Chen, Yan Li

TL;DR
This case report highlights the difficulty in distinguishing OHVIRA syndrome from Gartner duct cyst in prepubertal girls using imaging techniques.
Contribution
The study presents two cases showing diagnostic overlap between OHVIRA syndrome and Gartner duct cyst due to similar imaging features.
Findings
Both cases showed unilateral renal agenesis and cystic lesions near the bladder on CT and MRI.
Diagnostic challenges arose due to overlapping embryologic origins and imaging findings between the two conditions.
Abstract
This case series explores the diagnostic overlap between OHVIRA syndrome (obstructed hemivagina and ipsilateral renal anomaly) and Gartner duct cyst (GDC) with ipsilateral renal dysplasia in two prepubertal girls. Both cases exhibited similar imaging features on CT and MRI—including unilateral renal agenesis, ectopic ureter with abnormal insertion, cystic lesions posterolateral to the bladder— which led to significant diagnostic challenges. Despite differing in pathology, the overlap in embryologic origins and imaging findings made differentiation difficult. This series underscores the importance of comprehensive imaging and a multidisciplinary approach for accurate diagnosis. Current management strategies are discussed, highlighting the need for individualized treatment plans in prepubertal patients with complex genitourinary anomalies.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
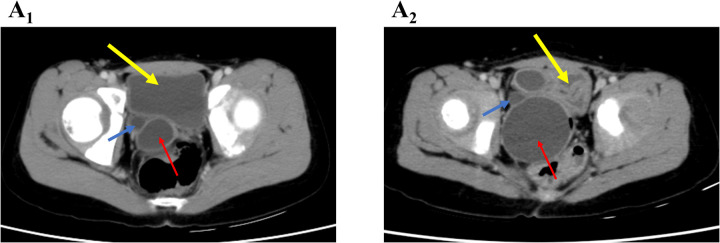 Figure 1
Figure 1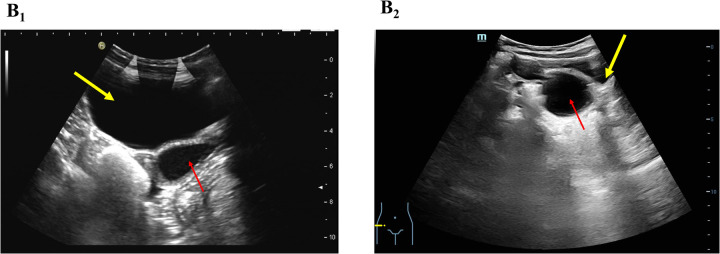 Figure 2
Figure 2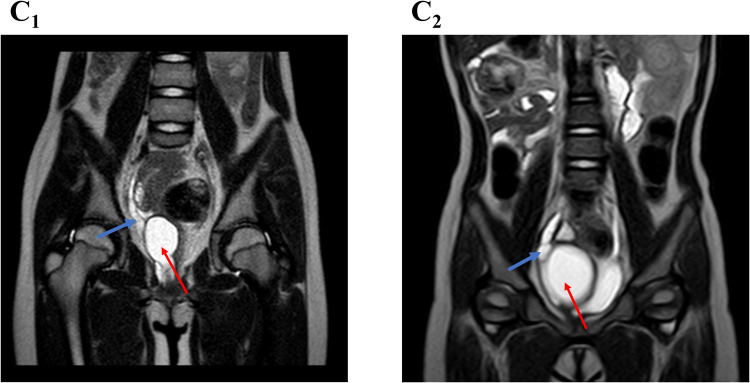 Figure 3
Figure 3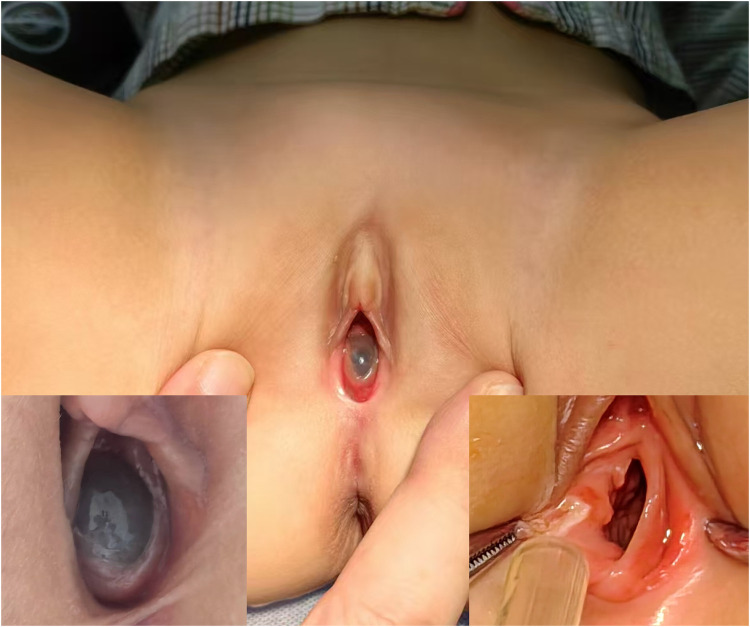 Figure 4
Figure 4- —Medical Health Science and Technology Project of Zhejiang province
- —Ningbo medical key supporting discipline
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParvovirus B19 Infection Studies · Tumors and Oncological Cases · Teratomas and Epidermoid Cysts
Introduction
OHVIRA syndrome (Obstructed Hemivagina and Ipsilateral Renal Anomaly) and Gartner duct cyst (GDC) are rare congenital anomalies of the genitourinary system, both arising from abnormalities in the Müllerian and/or Wolffian ducts (1–3). OHVIRA syndrome typically presents with an obstructed hemivagina, uterine anomalies, and ipsilateral renal agenesis. GDCs are remnants of the Wolffian duct that develop in the anterolateral vaginal wall and may extend toward the posterior aspect of the bladder (4). Notably, approximately 10% of GDCs are associated with renal agenesis or dysplasia, which is often accompanied by an ectopic ureter (4, 5). Such ectopic ureters are also commonly observed in OHVIRA syndrome (3). Therefore, when both conditions are associated with an ectopic ureter, overlapping imaging features may lead to significant diagnostic challenges.
We describe two prepubertal girls who were referred to our tertiary hospital for evaluation and management, presented one month apart (Supplementary Table S1). These cases highlight the diagnostic complexities in distinguishing these two anomalies and underscore the importance of imaging analysis supported by a multidisciplinary approach for appropriate management. Written informed consent was obtained from the patients and their families for publication of these cases.
Case descriptions
Case 1: OHVIRA syndrome with ectopic ureter
An 8-year-old girl was referred for evaluation after prenatal ultrasound revealed right renal ectopia with multicystic dysplasia. Her growth and development were normal. One year ago, a contrast-enhanced abdominal computed tomography (CT) revealed right renal dysplasia, with compensatory hypertrophy of the left kidney (Supplementary Figure S1A). Dilation of the distal ureter behind the bladder and a cystic mass located between the bladder and rectum suggested vaginal fluid accumulation (Figure 1A1, Supplementary Figure S1B). Due to the absence of symptoms, outpatient follow-up was recommended.
Axial CT image showing a cystic mass (red arrow) and a dilated ureter (blue arrow), both located posterior and lateral to the bladder (yellow arrow) on the right side. (A1) OHVIRA syndrome case; (A2) Gartner duct cyst case.
Upon admission, physical examination was unremarkable. Ultrasound revealed a uterus measuring 21 × 10 × 19 mm and a cystic mass (33 × 24 mm) posterior to the bladder, closely related to the vagina (Figure 2B1). The distal right ureter (9 mm) appeared to communicate with the vagina (Supplementary Figure S2). Magnetic resonance imaging (MRI) indicated a cystic lesion posterior to the bladder, likely due to vaginal distension from an oblique septum (Supplementary Figures S3A,B). The dilated right distal ureter appeared to ectopically insert into the vagina (Figure 3C1).
B-ultrasound showing a cystic mass (red arrow) posterior to the bladder (yellow arrow), likely originating from the vagina. (B1) OHVIRA syndrome case; (B2) Gartner duct cyst case.
Sagittal MRI image showing a dilated right distal ureter (blue arrow) adjacent to a cyst (red arrow), possibly ectopically opening into the cyst. (C1) OHVIRA syndrome case; (C2) Gartner duct cyst case.
A multidisciplinary team, including radiologists, gynecologists, and pediatric urologists, consulted on the case. The surgical team performed cystoscopy, vaginoscopic septum resection, and laparoscopic removal of the dysplastic kidney and ureter. Cystoscopy revealed the absence of the right ureteral orifice, while the left appeared normal. Vaginoscopy identified and resected an oblique septum compressing the upper right vaginal wall, exposing a hemivagina merging distally with the original vagina. Laparoscopy successfully removed the ectopic dysplastic kidney and distal ureter. The patient recovered uneventfully and was discharged on postoperative day three. The patient and her family were satisfied with the treatment outcome, noting a smooth recovery and effective care. A three-month follow-up ultrasound showed no vaginal fluid accumulation, and the patient remained asymptomatic.
Case 2: Gartner duct cyst with ectopic ureter and renal dysplasia
A 2-year-7-month-old girl was referred for evaluation following prenatal ultrasound findings of right renal ectopia with dysplasia. Growth and development were normal. An MRI performed one month earlier revealed right renal dysplasia and a funnel-shaped cystic mass located below and posterior to the bladder (Supplementary Figure S4). A tubular cystic structure (55 × 7 mm) adjacent to the mass appeared to connect with its lower portion, suggesting an ectopic ureter (Figure 3C2). Due to the absence of symptoms, outpatient follow-up was recommended.
On admission, a cystic mass approximately 2 cm in diameter was observed protruding from the vaginal introitus between the labia minora (Figure 4). The rest of the physical examination was unremarkable. Ultrasound revealed a cystic mass (67 × 40 × 39 mm) posterior to the bladder (Figure 2B2), likely originating from the vagina, and a right-sided cystic structure (28 × 14 × 24 mm) that appeared to communicate with it. A contrast-enhanced abdominal CT scan revealed an ectopic, dysplastic right kidney above the iliac vessels, cystic dilation of the distal ureter (Supplementary Figure S5A), and possible vaginal dilatation, suggesting hydrocolpos (Figure 1A2; Supplementary Figure S5B).
A 2-year-7-month-old girl with Gartner duct cyst involving an ectopic ureter and renal dysplasia, showing a cystic mass (approximately 2 cm in diameter) protruding between the labia minora, originating near the vaginal introitus.
A multidisciplinary team also evaluated the case for OHVIRA syndrome with imperforate hymen. Consent was obtained for cystoscopy, vaginoscopy, and laparoscopic exploration. Under anesthesia, examination revealed a cystic mass near the vaginal opening, with normal urethral and vaginal orifices. Cystoscopy confirmed the absence of the right ureteral orifice, while the left was normal. Vaginoscopy revealed a normal vaginal wall and cervix. Incision of the cyst released clear fluid, revealing an ectopic ureteral opening. Laparoscopy was used to remove the ectopic dysplastic kidney and distal ureter. The patient recovered well and was discharged on day three. The patient's parents were satisfied with the outcome, noting the successful recovery and effective care provided. A two-month follow-up ultrasound showed no cystic masses, and the patient remained asymptomatic.
Discussion
GDC with an ectopic ureter results from the failure of the terminal ureteric bud to separate from the mesonephric duct, preventing proper fusion with the primitive bladder and leading to ectopic insertion into the GDC (5). In OHVIRA syndrome, abnormal development of the mesonephric duct disrupts Müllerian duct fusion, causing the ureter to open into the ipsilateral obstructed hemivagina (1, 3). This embryologic overlap contributes to the imaging and clinical similarities between OHVIRA and GDC, which, especially when accompanied by renal dysplasia and ectopic ureter, pose significant challenges for preoperative diagnosis. Therefore, these overlapping imaging features emphasize the need for comprehensive imaging and a multidisciplinary approach for accurate differentiation in prepubertal patients.
Both cases were asymptomatic until treatment, whereas adolescents or adults may experience cyclic abdominal pain, urinary symptoms (e.g., infections or incontinence), or uterine bleeding (6, 7). Detailed imaging, including CT, MRI, and ultrasound, played a critical role in identifying key features of each condition. However, even with advanced imaging, intraoperative exploration was necessary to accurately diagnose the cysts and determine the proper course of treatment. In Case 1, imaging and ultrasound failed to identify uterus didelphys, leading to an uncertainty in the preoperative diagnosis. Laparoscopy and vaginoscopy ultimately confirmed the diagnosis of OHVIRA syndrome.
Case 2 had a similar clinical history and imaging findings to Case 1, initially suggesting OHVIRA syndrome. Intraoperative exploration revealed that the cyst originated from the paravaginal area, further complicating the diagnosis. Possible diagnoses included a blind-ended ectopic ureterocele, obstructed hemivaginal protrusion, Gartner duct cyst, or other mesonephric (Wolffian) duct derivatives (5, 8). However, further evaluation was needed to confirm the exact diagnosis.
Vaginoscopy identified only one cervix, and laparoscopy confirmed a single uterine body, ruling out OHVIRA syndrome. Ectopic ureteroceles are typically located distal to the trigone, inserting into the bladder neck, urethra, or other pelvic areas, often presenting with urinary incontinence depending on the function of the ipsilateral kidney (9). However, the blind-ended cyst in this case did not align with these features. Cystoscopy showed no right hemitrigone, ureteral orifice, intravesical ureterocele, or ectopic ureter opening into the urethra. Exploration of the cyst cavity revealed a wide ureteral opening at the proximal end without compression signs, ruling out this diagnosis as well. GDCs can extend alongside anterolateral vaginal wall from the proximal bladder to the perineal vestibule—consistent with this case's presentation. Unfortunately, histopathological analysis was not performed, which could have helped differentiate the cyst's origin, specifically whether it was a mesonephric or Müllerian derivative. Mesonephric (Wolffian) cysts typically consist of cuboidal or low columnar cells, whereas Müllerian derivatives are characterized by stratified squamous epithelium (2).
However, the appropriate timing of surgical intervention in OHVIRA and GDC cases remains controversial (10). OHVIRA in prepubertal patients is often discovered incidentally, whereas adolescents may present with cyclic pain, hematocolpos, or infections following menstruation (1). Treatment is typically recommended at puberty to alleviate symptoms and prevent complications such as endometriosis or infertility (11). Jang Hee Han et al. (3) reported 43 prepubertal OHVIRA cases, with six symptomatic patients undergoing vaginal septum resection and three undergoing nephrectomy for ectopic multicystic dysplastic kidney. The remaining cases did not routinely undergo septum resection due to insufficient evidence. Carmen Capito et al. (12) retrospectively studied eight prepubertal OHVIRA cases, with seven undergoing septum and dysplastic kidney resection, though symptom status was not specified. In our case, we performed transvaginal septal resection and nephrectomy safely.
For GDC, conservative management is recommended for asymptomatic cases, while excision or marsupialization is indicated for symptomatic cases with compression or infections. Sida Niu et al. (2) used fluorescein dye for complete GDC resection, while Sandra L. Emmons et al. (13) advised against resection if intact removal was not feasible, suggesting marsupialization or sclerotherapy instead. In our case, considering the patient's young age and the potential local trauma associated with complete GDC excision, a partial cyst wall resection was performed. Despite imaging suggesting renal agenesis, an ectopic ureter opening into the GDC was identified, prompting excision of the dysplastic kidney.
This study did not confirm whether the fluid in the GDC or OHVIRA cavities was urine, nor were contrast studies performed to delineate the ectopic ureteral course or identify its precise openings. Histopathological examination was also not conducted to distinguish the cyst origin (mesonephric vs. Müllerian). Moreover, the small uterine size typical of prepubertal girls limited the visualization of uterine duplication on imaging. As a result, intraoperative findings played a pivotal role in establishing the final diagnosis. Future studies incorporating histopathological confirmation, imaging enhancements, and extended follow-up are warranted to strengthen diagnostic accuracy and evaluate long-term outcomes.
Conclusion
The overlapping embryologic origins and imaging features of OHVIRA syndrome with ectopic ureter and GDC with ectopic ureter and renal dysplasia pose significant diagnostic challenges. These cases highlight the need for careful clinical evaluation, detailed imaging, and a multidisciplinary approach for accurate differentiation and appropriate intervention. For asymptomatic cases, the benefits of prepubertal surgical treatment require long-term follow-up to assess outcomes and potential complication.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Peixoto SA Souza NS Tannure SP Bicalho BT. Hemihysterectomy in a patient with uterus didelphys, vaginal septum and ipsilateral renal agenesis: a case report and literature review. Int J Gynaecol Obstet. (2024) 165(3):969–74. 10.1002/ijgo.1524737968793 · doi ↗ · pubmed ↗
- 2Niu S Didde RD Schuchmann JK Zoorob D. Gartner’s duct cysts: a review of surgical management and a new technique using fluorescein dye. Int Urogynecol J. (2020) 31(1):55–61. 10.1007/s 00192-019-04091-931471622 · doi ↗ · pubmed ↗
- 3Han JH Lee YS Im YJ Kim SW Lee MJ Han SW. Clinical implications of obstructed hemivagina and ipsilateral renal anomaly (OHVIRA) syndrome in the prepubertal age group. P Lo S One. (2016) 11(11):e 0166776. 10.1371/journal.pone.016677627861623 PMC 5115795 · doi ↗ · pubmed ↗
- 4Kalva SP Rammurti S Subbarao D Chittibabu N Murthy VS. Small ureterocele-like Gartner’s duct cyst associated with ipsilateral renal aplasia: a case report. Australas Radiol. (2001) 45(1):62–3. 10.1046/j.1440-1673.2001.00877.x 11259976 · doi ↗ · pubmed ↗
- 5Dwyer PL Rosamilia A. Congenital urogenital anomalies that are associated with the persistence of Gartner’s duct: a review. Am J Obstet Gynecol. (2006) 195(2):354–9. 10.1016/j.ajog.2005.10.81516890546 · doi ↗ · pubmed ↗
- 6Schlomer B Rodriguez E Baskin L. Obstructed hemivagina and ipsilateral renal agenesis (OHVIRA) syndrome should be redefined as ipsilateral renal anomalies: cases of symptomatic atrophic and dysplastic kidney with ectopic ureter to obstructed hemivagina. J Pediatr Urol. (2015) 11(2):77.e 1–6. 10.1016/j.jpurol.2014.12.00425797857 · doi ↗ · pubmed ↗
- 7Lim LM Sivapatham L Chong A Wahab A. Obstructed hemivagina ipsilateral renal agenesis (OHVIRA) syndrome-A retrospective cohort analysis of the Sabah population. J Pediatr Adolesc Gynecol. (2023) 36(6):541–4. 10.1016/j.jpag.2023.07.00237451429 · doi ↗ · pubmed ↗
- 8Acien P Acien M Romero-Maroto J. Blind hemibladder, ectopic ureterocele, or Gartner’s duct cyst in a woman with Mullerian malformation and supposed unilateral renal agenesis: a case report. Int Urogynecol J. (2010) 21(3):365–9. 10.1007/s 00192-009-0952-419597716 · doi ↗ · pubmed ↗