Paraneoplastic Trichomegaly as a Harbinger of Metastatic Renal Cell Carcinoma: A Case Report
Allison Reichl, Rena Callahan

TL;DR
A man with unusual eyelash growth was later diagnosed with metastatic kidney cancer, highlighting the importance of considering hidden cancers in rare skin symptoms.
Contribution
This case report presents paraneoplastic trichomegaly as an exceptionally rare initial sign of metastatic renal cell carcinoma.
Findings
Trichomegaly resolved with treatment but the patient eventually died from metastatic RCC.
Trichomegaly is typically linked to congenital syndromes or HIV, not cancer.
Unusual mucocutaneous symptoms may indicate an underlying malignancy.
Abstract
Renal cell carcinoma (RCC) is a common malignancy, often diagnosed incidentally on cross-sectional imaging. While classic symptoms such as flank pain, hematuria, and a palpable abdominal mass are well-known, RCC may present with more insidious findings. Here, we describe a case of paraneoplastic trichomegaly as the initial manifestation of metastatic RCC. A man in his 60s presented with progressive eyelash lengthening and mild hypertrichosis of the extremities and beard. Medication review and initial endocrine workup were unrevealing. Laboratory tests showed iron deficiency anemia, and subclinical hematuria was noted on urinalysis. Imaging revealed a right renal mass and retroperitoneal lymphadenopathy. Biopsy confirmed clear cell RCC. The patient was treated with neoadjuvant immunotherapy followed by radical nephrectomy. His trichomegaly improved with treatment. Unfortunately, he…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
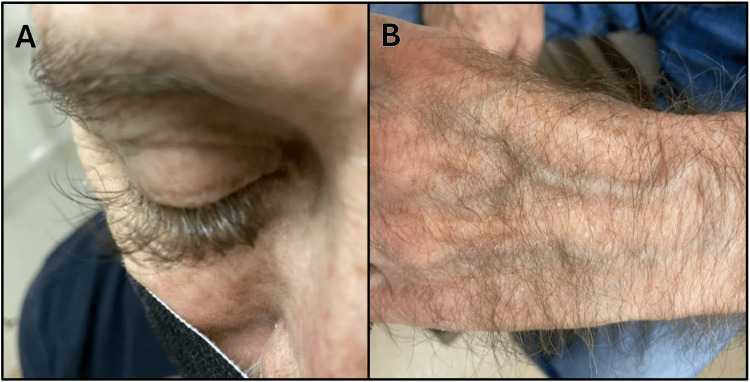 Figure 1
Figure 1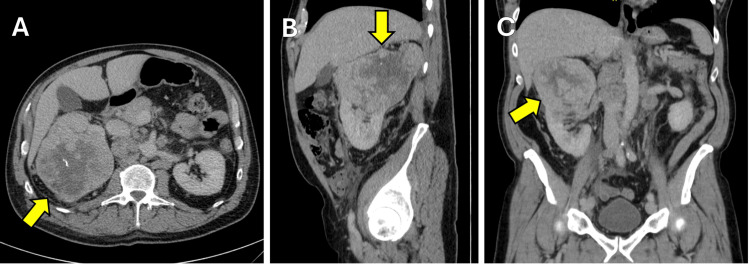 Figure 2
Figure 2| Test | Patient Value | Reference Range | Units |
| WBC Count | 8.0 | 3.8-10.8 | x103/uL |
| Hemoglobin | 12.1 | 13.2-17.1 | g/dL |
| Platelet Count | 362 | 140-400 | x103/uL |
| Iron | 29 | 50-160 | mcg/dL |
| TIBC | 259 | 230-425 | mcg/dL |
| Ferritin | 563 | 24-380 | ng/mL |
| Vitamin B12 | 534 | 200-1100 | pg/mL |
| Folate | 12.3 | >5.4 | ng/mL |
| Testosterone, Total | 573 | 200-1100 | ng/dL |
| Testosterone, Free | 75 | 35-155 | pg/mL |
| DHEA | 88 | 22-244 | mcg/dL |
| FSH | 5.9 | 1.6-8.0 | mIU/mL |
| Prolactin | 6.7 | 2-18 | ng/mL |
| TSH | 1.37 | 0.4-4.5 | mIU/L |
| Free T4 | 1.1 | 0.8-1.8 | ng/mL |
| Hemoglobin A1c | 6.0 | <5.7 | % |
| Urinalysis | (+) trace occult blood, (-) protein, (-) WBC | - | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenetic and rare skin diseases. · Cutaneous Melanoma Detection and Management · Cancer Diagnosis and Treatment
Introduction
Renal cell carcinoma (RCC) is a relatively common malignancy, with a peak incidence between 60 and 70 years of age; its lifetime prevalence is 2.3% in men and 1.3% in women [1,2]. The majority of RCCs are identified incidentally, in part due to the increasing availability of cross-sectional abdominal imaging techniques [3]. At the time of RCC diagnosis, 70% of cases are stage I and 11% are Stage IV [4]. The three most common histological subtypes of RCC are clear cell (75-80%), papillary (10-15%), and chromophobe (5%) [5].
The classically taught triad of flank pain, palpable abdominal mass, and hematuria occurs in less than 10% of patients with newly diagnosed RCC [6]. Of patients with RCC, 10-40% have associated paraneoplastic syndromes (PNS), which sometimes are the presenting complaint. These resolve with nephrectomy in up to 52% of cases [7]. Here we present an unusual case of paraneoplastic eyelash growth associated with the onset of RCC.
Case presentation
A man in his 60s presented to his primary care physician for several months of unusual lengthening and thickening of his eyelashes (Figure 1A). On further history, he also endorsed mild lengthening of the hair on his arms, hands, beard, and lower extremities (Figure 1B). He was otherwise asymptomatic and not taking medications known to cause trichomegaly. Laboratory workup (Table 1) for endocrinopathies was benign. He was noted to have a mild normocytic anemia with low serum iron and low iron saturation. Ferritin was elevated. Urinalysis demonstrated trace blood. In hindsight, the patient recalled that he had experienced one episode of gross hematuria six months prior, which had resolved on its own.
Patient's (A) lengthened eyelashes and (B) left hand hair growth.
Cross-sectional imaging was obtained, demonstrating an 11.7 cm mass in the right kidney and nodules in the right retroperitoneum consistent with metastatic RCC (Figure 2). The patient was referred to Oncology. Core biopsy of the left para-aortic lymph node was then obtained; pathology showed clear cell carcinoma. The patient was treated with 10 cycles of neoadjuvant nivolumab (a PD-1 inhibitor) and cabozantinib (a tyrosine kinase inhibitor) prior to right radical nephrectomy.
(A) Axial, (B) sagittal, and (C) coronal views of right renal mass.
The patient continued adjuvant nivolumab and cabozantinib monthly after nephrectomy, and his eyelash growth slowed significantly on treatment. Within one year, the patient experienced disease progression with progressive multi-station lymphadenopathy demonstrated on PET/CT. Nineteen months after his initial diagnosis, he passed away due to acute thrombotic complications of the carcinoma, including a large superior mesenteric vein thrombus. Autopsy demonstrated widely metastatic disease throughout the abdomen, lymph nodes, lungs, and myocardium.
Discussion
Hypertrichosis is classically associated with endocrine disorders and medications, but has been reported as a rare paraneoplastic phenomenon of carcinomas [8,9]. The biochemical mechanism promoting hair growth remains poorly understood [8].
Eyelash trichomegaly is a specific type of hypertrichosis. The term "trichomegaly" was first coined by Gray in 1944, in reference to long "movie lashes" desired by Hollywood actresses [10]. Since that time, scientists have elucidated the basic pathophysiology of lash hair follicles. Over a span of 4-11 months, eyelashes cycle through phases of continuous growth (anagen phase), transition (catagen phase), and rest (telogen phase) [11]. Trichomegaly stems from the prolongation of the anagen phase, but the cause for the induction of this prolongation remains murky. In Oncology literature, epidermal growth factor receptor (EGFR) antagonists (i.e., cetuximab or erlotinib) have been strongly associated with trichomegaly [12,13], suggesting EGFR-mediated signaling may serve as a “molecular brake” on eyelash growth [14].
Trichomegaly was initially postulated to be a cutaneous manifestation specific to HIV/AIDS [15], but has since been reported in association with atopic conditions, congenital disorders, malnutrition, and malignancy [16]. Documented association with renal cancer is exceedingly rare. There exists one case report of a 55-year-old man who developed trichomegaly 13 months after radical nephrectomy for stage one renal adenocarcinoma; he was ultimately found to have recurrence of disease in the lymph nodes and died shortly after [17].
In the case of the current patient, the lengthening and thickening of his eyelashes and existing body hair differed from the diffuse lanugo that has been described in paraneoplastic hypertrichosis lanuginosa [9]. However, his presentation may have been a variant of this syndrome.
The clinical implications of RCC-related PNS are not well-established. PNS itself lacks a clear definition, but it is loosely described as a set of signs and symptoms triggered by a malignant tumor that cannot be associated with its primary site or metastases [18]. In a retrospective study of 2865 patients with localized RCC, those with PNS (defined as anemia, polycythemia, hypercalcemia, and liver dysfunction) had a higher risk of death from all causes (hazard ratio (HR) = 1.64; 95%CI = 1.35-1.99) and death from RCC (HR = 1.86; 95%CI = 1.19-2.92) [19]. These findings are difficult to extrapolate to patients in the metastatic setting and those with a more esoteric PNS, such as hypertrichosis.
Regardless, early detection of RCC by any sign or symptom significantly impacts patient outcomes. In the United States from 2014-2020, the five-year relative survival rate for patients with localized renal cancer was 93.3% (95%CI 92.9-93.6). This is compared to a five-year relative survival of only 18.2% (95%CI 17.5-18.9) for those with distant metastases [20]. Overall median survival for patients with metastatic RCC is 22 months (95%CI 20.2-26.5), though this has improved significantly with the advent of modern immune checkpoint and tyrosine kinase inhibitors [6,21].
Conclusions
This case highlights the importance of pausing to consider more insidious etiologies when faced with an unusual mucocutaneous finding. Occult malignancy should be considered in patients who develop atypical hair growth patterns, especially those of advanced age. Further investigation is needed to elucidate the immunomodulatory mechanisms by which RCC and other cancers trigger the development of trichomegaly.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cancer statistics, 2023 CA Cancer J Clin Siegel RL Miller KD Wagle NS Jemal A 17487320233663352510.3322/caac.21763 · doi ↗ · pubmed ↗
- 2Epidemiology of renal cell carcinoma Eur Urol Capitanio U Bensalah K Bex A 74847520193024379910.1016/j.eururo.2018.08.036PMC 8397918 · doi ↗ · pubmed ↗
- 3Challenges of early renal cancer detection: symptom patterns and incidental diagnosis rate in a multicentre prospective UK cohort of patients presenting with suspected renal cancer BMJ Open Vasudev NS Wilson M Stewart GD 010202010.1136/bmjopen-2019-035938 PMC 722329232398335 · doi ↗ · pubmed ↗
- 4Clinical stage migration and survival for renal cell carcinoma in the United States Eur Urol Oncol Patel HD Gupta M Joice GA Srivastava A Alam R Allaf ME Pierorazio PM 343348220193127777110.1016/j.euo.2018.08.023 · doi ↗ · pubmed ↗
- 52004 WHO classification of the renal tumors of the adults Eur Urol Lopez-Beltran A Scarpelli M Montironi R Kirkali Z 7988054920061644220710.1016/j.eururo.2005.11.035 · doi ↗ · pubmed ↗
- 6Renal cell carcinoma: a review JAMA Rose TL Kim WY 1001101033220243919654410.1001/jama.2024.12848 PMC 11790279 · doi ↗ · pubmed ↗
- 7Incidence and clinical relevance of paraneoplastic syndromes in patients with renal cell carcinoma Urol Oncol Moldovan T Boynton D Kuperus J 39239741202310.1016/j.urolonc.2023.06.01537537025 · doi ↗ · pubmed ↗
- 8Cutaneous paraneoplastic syndromes Semin Diagn Pathol Wick MR Patterson JW 2112283620193073699410.1053/j.semdp.2019.01.001 · doi ↗ · pubmed ↗