Gross hematuria in an immunocompromised male - A case report
Kenneth Cintrón Cartagena, Gustavo Christian Colón, Merary Nazario Pérez, Jaime Matta, Adrian Santana Parachini, Javier Castillo Ortiz

TL;DR
A rare case of Merkel cell carcinoma metastasizing to the bladder in an immunocompromised Hispanic male is reported, highlighting the use of narrowband imaging for diagnosis.
Contribution
This is the first reported case of MCC bladder metastasis in a Puerto Rican immunocompromised male and the first to use narrowband imaging for MCC bladder diagnosis.
Findings
MCC metastasis to the bladder is exceedingly rare and presents unique diagnostic challenges.
Narrowband imaging was used for the first time in MCC bladder metastasis diagnosis.
The case underscores the importance of considering rare metastatic sites in MCC patients.
Abstract
Merkel cell carcinoma (MCC) is a rare, aggressive neuroendocrine skin cancer with a high propensity for metastasis. While MCC has been reported in various organs, its metastasis to the bladder is exceedingly uncommon. Bladder infiltration in MCC presents a unique diagnostic and therapeutic challenge in Urology. Only few have been described worldwide, and no cases have been reported in Hispanic males. This is the first published case of an immunocompromised Hispanic patient with MCC metastasis to the bladder and to our knowledge, the first case report worldwide to include narrowband imaging (NBI) in the diagnostic algorithm of MCC to the bladder. We report the case of a 53-year-old immunocompromised Puerto Rican male diagnosed with metastatic MCC. The patient had previously developed MCC with metastasis to the inguinal lymph nodes and received treatment. Later management involved…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
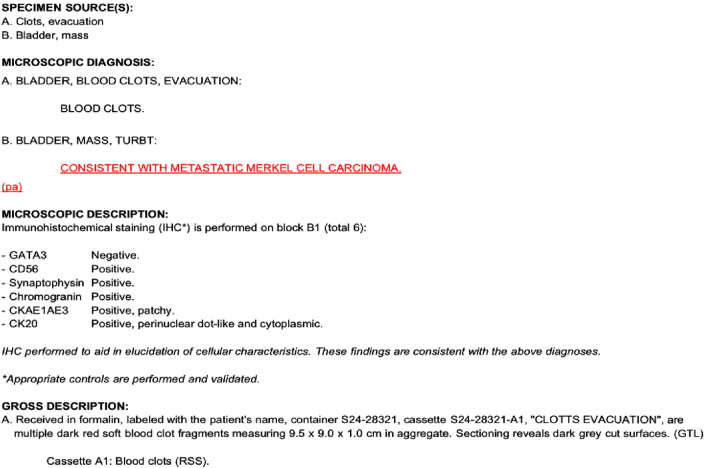 Figure 1
Figure 1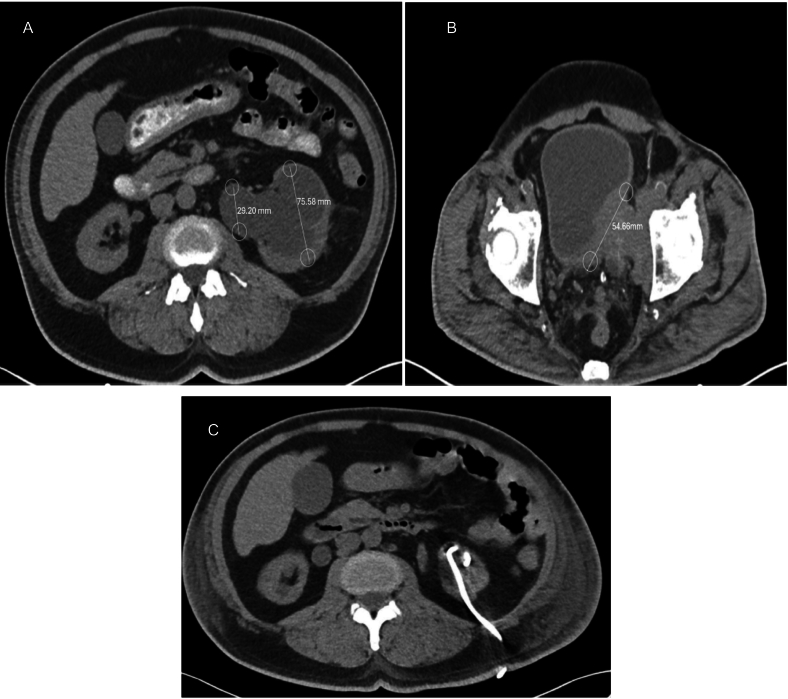 Figure 2
Figure 2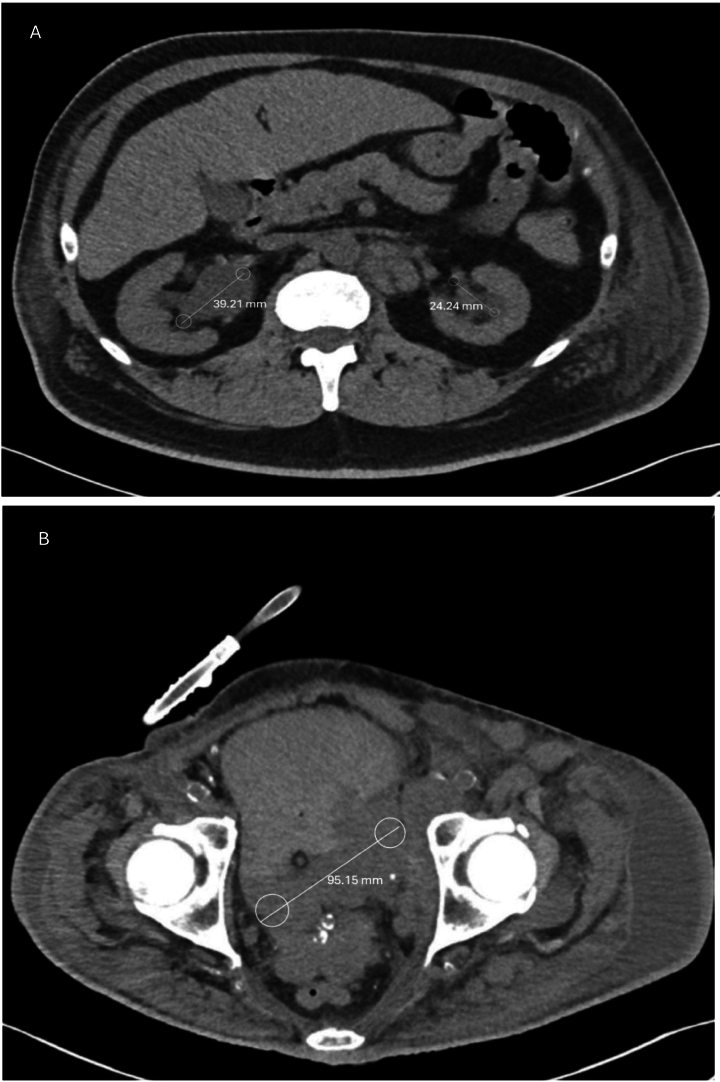 Figure 3
Figure 3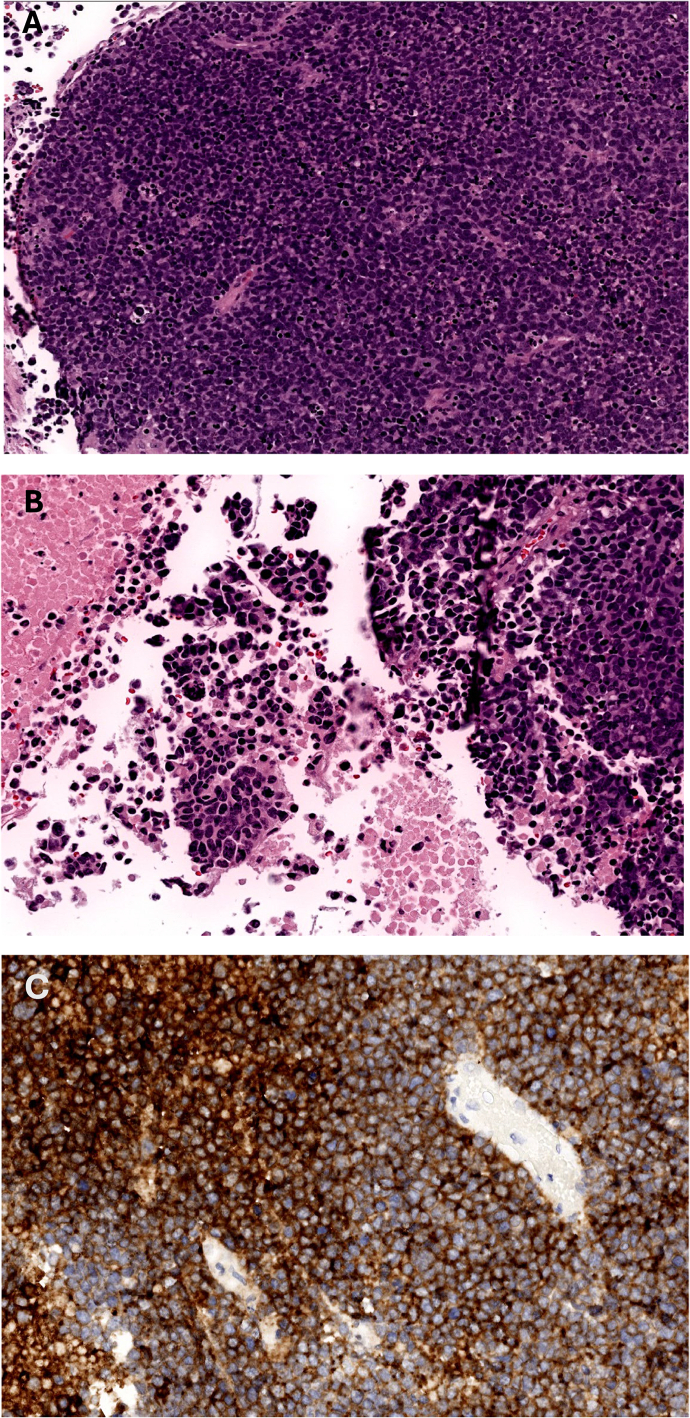 Figure 4
Figure 4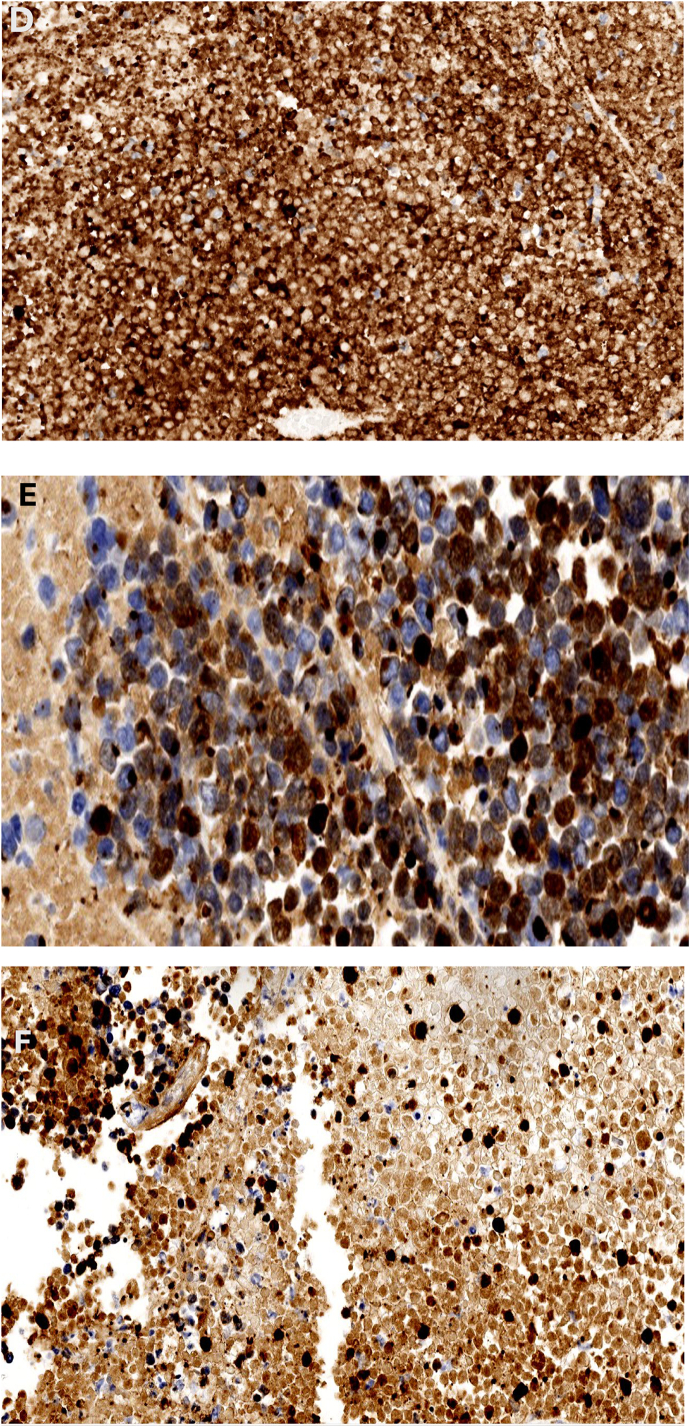 Figure 5
Figure 5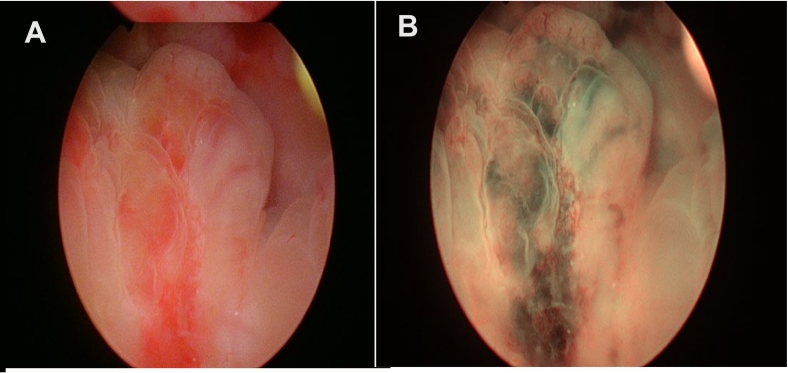 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPolyomavirus and related diseases · Urinary and Genital Oncology Studies · Bladder and Urothelial Cancer Treatments
Introduction
1
Merkel cell carcinoma (MCC) is a rare and aggressive skin cancer originating from cutaneous neuroendocrine Merkel cells due to sun exposure or immune-mediated pathways [1]. It has a low incidence, with about 2500 new cases diagnosed annually in the U.S. [1]. MCC has a poor prognosis, particularly in metastatic stages, due to its rapid growth and high metastatic potential [2]. The condition primarily affects Caucasians over 50 years of age with a history of significant sun exposure, chronic immune suppression, or Merkel cell polyomavirus (MCPyV) infection [2]. Clinically, MCC presents as a firm, erythematous nodule on sun-exposed skin [3]. The antibody titer to the MCPyV oncoprotein serves as a biomarker for treatment response in some patients [4]. MCC is often misdiagnosed as other malignancies, such as basal cell carcinoma, squamous cell carcinoma, malignant melanoma, lymphoma, or small cell carcinoma, highlighting the need for accurate immunohistochemical analysis [5]. Key markers like cytokeratin 20 (CK20) and neuron-specific enolase distinguish MCC from other skin cancers [6].
MCC commonly metastasizes to fascia, muscle, and bone, but genitourinary tract metastasis, particularly to the bladder, is exceedingly rare, documented only four times [7]. Treatment typically includes surgery, radiation therapy, and chemotherapy, with immunotherapy emerging as a promising option for metastatic cases [8]. Checkpoint inhibitors targeting the PD-1/PD-L1 pathway have improved survival rates, but prognosis remains poor, with a five-year survival rate of 18 % for metastatic MCC [9]. Early detection and a multidisciplinary approach are crucial to improving outcomes. The American Joint Committee on Cancer (AJCC) classifies MCC staging using the TNM system, where advanced stages correlate with decreased survival rates [10]. The National Cancer Data Base reports five-year survival rates ranging from 80 % (Stage IA) to 20 % (Stage IV) [11]. Limited literature exists on MCC metastasizing to the bladder [[12], [13], [14], [15]], highlighting the need for clinical awareness when evaluating bladder tumors, particularly in immunocompromised patients. This case report presents a rare instance of MCC metastasizing to the bladder, emphasizing its clinical presentation, diagnostic challenges, and treatment.
Case report
2
A 53-year-old Hispanic/Latino Puerto Rican male presented with left-sided flank pain, dysuria, urinary dribbling, frequency, and hematuria. His medical history included hypertension, diabetes mellitus, chronic kidney disease (CKD), anal cancer (HPV-related), MCC, and HIV infection. Surgical history included right-sided Mediport catheter placement, right knee MCC excision, inguinal lymph node excision, and open surgery for stone removal. Diagnosed with HIV in 1991, he adhered to Darunavir/cobicistat and Dolutegravir therapy, with a CD4 count between 200 and 300 cells/mm^3^.
During the COVID-19 pandemic, the patient developed a red papule above the knee, which enlarged significantly before being biopsied and diagnosed as MCC. Subsequent imaging revealed metastasis to the right inguinal lymph nodes. He underwent chemotherapy with etoposide/cisplatin and radiation therapy (RT) in December 2020, followed by pembrolizumab from December 2022 to November 2023. Due to disease progression, avelumab was initiated in December 2023. A recent CT scan indicated left hydronephrosis caused by a 5.47 cm obstructing bladder mass extending into the left lower pelvis, shown in Fig. 1, with associated soft tissue thickening in the right abductor muscle encased the right common femoral artery and vein.Fig. 1(A–C) NOV 10 2024.Fig. 1
A percutaneous nephrostomy tube (PCNT), shown in Fig. 1, was placed due to complete ureteral obstruction, leading to renal decompression. Three weeks later, the patient was readmitted with gross hematuria, urinary dribbling, and right-sided flank pain. A CT scan showed unchanged bladder mass size but increasing right-sided hydronephrosis. Subsequent imaging revealed significant tumor growth to 9.51 cm, shown in Fig. 2. Laboratory tests showed normochromic normocytic anemia, hyperkalemia, and worsening CKD, with creatinine rising from 4.5 to 5.5 mg/dL over two weeks.Fig. 2(A–B) (1).Fig. 2
A three-way Foley catheter with manual constant irrigation was placed for clot evacuation and urinary retention relief. Transurethral bladder resection of the tumor (TURBT) was performed using general anesthesia. Gross examination revealed a 9.5 × 9.0 × 1.0 cm dark red soft tissue mass with necrotic debris. Microscopic analysis identified small round basophilic cells with a high nucleus-to-cytoplasm ratio, dispersed chromatin, and decreased cytoplasm, consistent with neuroendocrine tumors, shown all in Fig. 3. Immunohistochemical staining confirmed MCC, with tumor markers positive for Chromogranin, CD56, Synaptophysin, Cytokeratin AE1/AE3, and CK20 [15]. CD 56 shown in Fig. 3C, Synaptophysin shown in Fig. 3D, Cytokeratin AE1/AE3 shown in Fig. 3E CK20 positivity confirmed its Merkel cell origin, shown in Fig. 3F. Pathology report in Table 1.Fig. 3(A–F) November 10.Fig. 3. Table 1Pathologic Result from Bladder Tumor Resection.Table 1
Discussion
3
This case represents an exceptionally rare instance of MCC metastasizing to the bladder. Literature review suggests this is the first case diagnosed via narrow-band imaging (NBI). NBI contributed to diagnosis via improved visualization of vascular structures, which allowed for more efficient resection. NBI also aided in differentiation from other bladder lesions based on hypervascularity and mucosal changes in bladder epithelium. NBI findings are shown in Fig. 4, showing findings before (4A) and after (4B) visualization. Histopathology confirmed the diagnosis, with MCC displaying small, round cells, mitotic figures, and necrosis, consistent with aggressive neuroendocrine carcinoma [16]. Immunohistochemical markers confirmed MCC's epithelial and neuroendocrine origin, with CK20 further verifying its Merkel cell lineage [17].Fig. 4(A–B) November 10.Fig. 4
Previous case reports describe chemotherapy regimens using vinblastine and cisplatin or carboplatin and etoposide for palliative care [[12], [13], [14]]. Current guidelines from the National Comprehensive Cancer Network (NCCN) recommend systemic therapy and RT for distant MCC metastases [18]. Immunotherapy, particularly checkpoint inhibitors like pembrolizumab, has demonstrated durable responses [19]. The combination of platinum-based chemotherapy and topoisomerase inhibitors, such as cisplatin/etoposide, remains a standard approach [18]. Surgery may be beneficial for symptom control in metastatic MCC [18].
This patient's treatment aligned with NCCN guidelines for metastatic MCC. Checkpoint inhibitors (CPIs) are now frontline therapies for advanced MCC, showing promising results [19]. Staging using the TNM system classified this case as Stage IV, correlating with a poor prognosis [18]. Immunosuppression due to HIV infection likely contributed to MCC progression, as HIV-positive individuals have a 13-fold increased risk of MCC compared to the general population [20]. This association underscores the aggressive nature of MCC in immunocompromised individuals and the importance of early detection and tailored therapy.
Conclusion
4
This case highlights the rarity of MCC metastasizing to the bladder and underscores the importance of a multimodal management approach. Clinicians should consider MCC in the differential diagnosis of bladder masses, particularly in immunocompromised patients. Further research is needed to improve treatment strategies for distant MCC metastases. Vigilance and early intervention remain crucial for improving patient outcomes.
CRediT authorship contribution statement
Kenneth Cintrón Cartagena: Study concept, writing the paper, data collection, data analysis and interpretation
Gustavo Christian Colón: Writing the paper, data collection, data analysis
Merary Nazario Pérez: Writing the paper, data collection, data analysis
Jaime Matta: Writing the paper, data collection
Adrian Santana Parachini: Study concept, interpretation of data
Javier Castillo Ortiz: Writing the paper, study concept, data analysis, data interpretation
Consent
For this case report, informed consent was performed and patient signed consent form to carry out this case report. Evidence is available for review by editor upon request.
Ethical approval
Approved by IRB at local institution. IRB Protocol Number: 2408212354.
Sources of funding
No funding used to write this case report.
Guarantors
Kenneth Cintron Cartagena
Gustavo Christian Colon
Registration of research studies
This case report is not a “first in man” study.
Declaration of competing interest
No conflict of interests to report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Paulson K.G.Park S.Y.Vandeven N.A.Lachance K.Thomas H.Chapuis A.G.Nghiem P.Merkel cell carcinoma: current US incidence and projected increases based on changing demographics J. Am. Acad. Dermatol.783201845746310.1016/j.jaad.2017.10.02829102486 PMC 5815902 · doi ↗ · pubmed ↗
- 2Lewis C.W.Qazi J.Hippe D.S.Lachance K.Patterns of distant metastases in 215 Merkel cell carcinoma patients: implications for prognosis and surveillance Cancer Med.9420201374138210.1002/cam 4.278131883234 PMC 7013053 · doi ↗ · pubmed ↗
- 3Paulson K.G.Lewis C.W.Redman M.W.Simonson W.T.Lisberg A.Ritter D.Nghiem P.Viral oncoprotein antibodies as a marker for recurrence of Merkel cell carcinoma: a prospective validation study Cancer 123820171464147410.1002/cncr.3047527925665 PMC 5384867 · doi ↗ · pubmed ↗
- 4Schrama D.Ugurel S.Becker J.C.Merkel cell carcinoma: recent insights and new treatment options Curr. Opin. Oncol.242201214114910.1097/CCO.0b 013e 32834 fc 9fe 22234254 · doi ↗ · pubmed ↗
- 5Kervarrec T.Tallet A.Miquelestorena-Standley E.Houben R.Schrama D.Gambichler T.Guyétant S.Diagnostic accuracy of a panel of immunohistochemical and molecular markers to distinguish Merkel cell carcinoma from other neuroendocrine carcinomas Mod. Pathol.324201949951010.1038/s 41379-018-0155-y 30349028 · doi ↗ · pubmed ↗
- 6Becker J.C.Stang A.De Caprio J.A.Cerroni L.LebbéC.Veness M.Nghiem P.Merkel cell carcinoma Nat. Rev. Dis. Primers.320171707710.1038/nrdp.2017.7729072302 PMC 6054450 · doi ↗ · pubmed ↗
- 7Yer J.G.Storer B.E.Paulson K.G.Relationships among primary tumor size, number of involved nodes, and survival for 8044 cases of Merkel cell carcinoma J. Am. Acad. Dermatol.704201463764310.1016/j.jaad.2013.11.03124521828 PMC 3959572 · doi ↗ · pubmed ↗
- 8Trinidad C.M.Torres-Cabala C.A.Prieto V.G.Aung P.P.Update on eighth edition American Joint Committee on Cancer classification for Merkel cell carcinoma and histopathological parameters that determine prognosis J. Clin. Pathol.725201933734010.1136/jclinpath-2018-20550430636696 · doi ↗ · pubmed ↗