Twin‐peg and single‐peg unicompartmental knee arthroplasty designs show comparable clinical outcomes and radiographic results: A systematic review
Sadra Mohebbi, Yashar Khani, Elias Sadooghi Rad, Mohammadhossein Hefzosseheh, Mahya Aliakbari, Fateme Rezagholi, Amir Mehrvar

TL;DR
This systematic review finds that twin-peg and single-peg unicompartmental knee implants have similar clinical and radiographic outcomes, with no clear superiority for either design.
Contribution
The study systematically compares twin-peg and single-peg UKA designs, providing evidence on their clinical and radiographic performance.
Findings
Both twin-peg and single-peg designs showed comparable clinical outcomes and patient-reported measures.
Twin-peg designs had slightly lower revision rates in some studies, but evidence remains inconclusive.
Radiographic scores varied across studies, with no consistent advantage for either design.
Abstract
This systematic review compares single‐peg and twin‐peg unicompartmental knee arthroplasty (UKA) implant designs with respect to radiographic findings, clinical outcomes and implant longevity. A search strategy was applied to four databases, including PubMed, Scopus, Embase, and Web of Science. Inclusion criteria focused on studies of the twin‐peg and single‐peg designs in the UKA. Two reviewers independently performed screening, data extraction, and quality assessment. Study characteristics, patient demographics, clinical outcomes, revision rate and radiographic differences were extracted. We utilized the Risk of Bias (RoB) 2 tool and Risk of Bias in Non‐Randomized Studies of Intervention to assess the RoB in included studies. Seven studies were included in the final review. Results varied in the case of radiographic scores, clinical outcomes and patient‐reported outcome measures…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
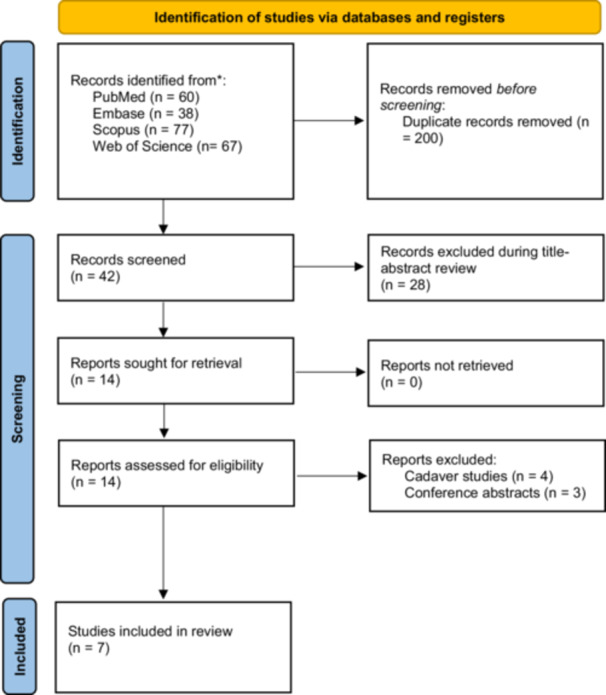 Figure 1
Figure 1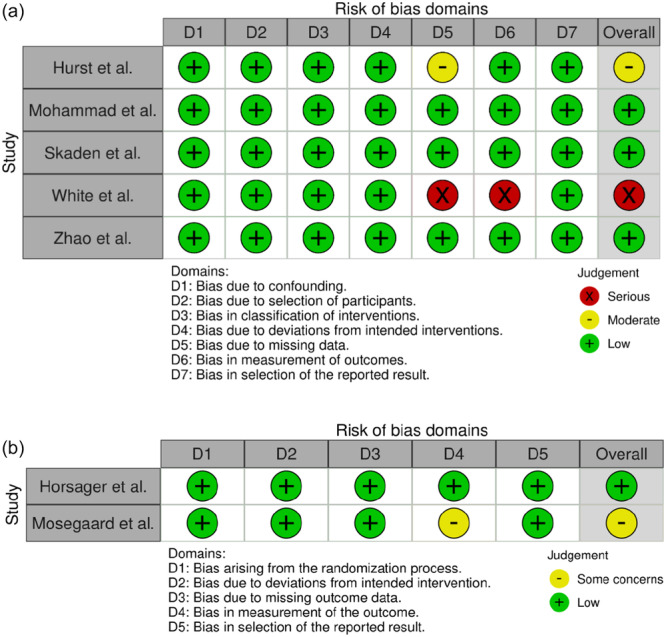 Figure 2
Figure 2| Participants | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Author/year | Country | Study type | Mean age (years) | Sex (female) | Total | Single‐peg | Twin‐peg | Follow‐up (years) | Outcome measures |
| Horsager et al. [ | Denmark, Netherlands | RCT | 63.62 | 32 (40%) | 80 | 29 | 51 | 5 |
Wear‐rate comparison OKS |
| Hurst et al. [ | USA | Cohort | 63.5 | 192 (53%) | 413 | 223 | 190 | N/A | Radiographic differences |
| Mohammad et al. [ | United Kingdom | Cohort | 65 | 2869 (50%) | 5668 | 2834 | 2834 | 3.3 |
Implant Survival Implant revision |
| Mosegaard et al. [ | Denmark | RCT | 63.45 | 32 (40%) | 80 | 29 | 51 | 5 |
Radiographic differences RSA DXA SF‐36 KOOS Implant revision |
| Skaden et al. [ | Norway | Cohort | 65.8 | 3551 (47.7%) | 7444 | 908 | 6536 | 8 |
Implant Survival Implant revision |
| White et al. [ | United Kingdom | Cohort | 67 | 121 (48.5%) | 249 patients (288 implants) | 0 | 288 | 5.1 |
Implant Survival, OKS score AKS‐F score Patient Satisfaction, The Tegner Activity score Knee ROM |
| Zhao et al. [ | China | Cohort | 63.11 | 19 (73%) | 26 | 15 | 11 | 2.1 |
Radiographic differences HSS score WOMAC score OKS score KSS score |
| Study | Clinical outcomes |
|---|---|
| Horsager et al. [ | The twin‐peg implant demonstrated a better improvement in OKS than the single‐peg, but it was not statistically significant. |
| White et al. [ | The twin‐peg knee had better clinical outcomes than the single‐peg knee and offered a high degree of sustained patient satisfaction |
| Zhao et al. [ | The single‐peg implant demonstrated a better HSS, WOMAC and KSS, but there was no statistically significant difference in the radiological scores and functional scores between the double‐peg and single‐peg implants. |
| Mosegaard et al. [ | SF‐36 and KOOS improvements were similar between single‐peg and twin‐peg designs, and twin‐peg was not superior to the single‐peg design. |
| Revision | Survival (%) | ||||||
|---|---|---|---|---|---|---|---|
| Author, year | Total | Twin‐peg, | Single‐peg, | Twin‐peg | Single‐peg | Follow‐up (years) | Note |
| 602 | |||||||
| White et al. [ | 5 | 5 (1.7) | NA | 98 | NA | 9 | – |
| Mohammad et al. [ | 230 | 99 (3.5) | 131 (5.4) | 96.2 | 94.8 | 5 | Sig |
| Mosegard et al. [ | 2 | 1 (2.0) | 1 (3.4) | NA | NA | – | – |
| Skaden et al. [ | 365 | 294 (4.5) | 71 (7.8) | 94 | 92 | 5 | Not sig |
| White (2015) | Mohammad (2019) | Mosegard (2022) | Skaden (2022) | |||||
|---|---|---|---|---|---|---|---|---|
| Twin (%) | Single (%) | Twin (%) | Single (%) | Twin (%) | Single (%) | Twin (%) | Single (%) | |
| Pain | 33.3 | – | 13.4 | 23.2 | – | – | 23.5 | 31.3 |
| Osteoarthritis progression | 50 | – | 37.3 | 26.2 | – | – | 15.5 | 16.7 |
| Instability | 16.7 | – | 10.4 | 6.1 | – | – | 15 | 12.5 |
| Infection | – | – | 7.5 | 7.1 | – | – | 15.2 | 5.2 |
| Aseptic loosening | – | – | 22.4 | 21.2 | 100 | – | 13.4 | 18.8 |
| Luxation | – | – | 6 | 8.1 | – | 100 | 10.7 | 6.2 |
| malalignment | – | – | 3 | 8.1 | – | – | 6.7 | 9.3 |
| Total ( | 6 | – | 67 | 99 | 1 | 1 | 328 | 96 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTotal Knee Arthroplasty Outcomes · Orthopaedic implants and arthroplasty · Orthopedic Infections and Treatments
INTRODUCTION
Total knee arthroplasty (TKA) is a reliable surgical procedure that can relieve pain and improve the function of patients with end‐stage knee osteoarthritis (OA) [1, 8, 29]. Although TKA has demonstrated great outcomes, such as implant survival rates greater than 90%, the procedure is associated with some complications, including aseptic loosening, fracture, instability, and periprosthetic joint infection [3, 20]. Notable improvements in the implant design and technique of unicompartmental knee arthroplasty (UKA) have led to increasing attention in research and clinical practice. Therefore, UKA, only affecting one compartment of the knee, has recently been introduced as a successful and viable treatment for arthritis [18]. On the other hand, some surgeons remain sceptical about the durability and efficacy of this treatment, considering TKA the gold standard treatment for arthritis.
UKA has shown better kinematics and good long‐term survivorship in many studies; however, the main problem with this technique is its higher revision rates compared to TKA [6, 13, 18]. The higher revision rates have mostly been reported due to aseptic loosening in a Norwegian study [4]. According to data from various studies, aseptic loosening seems to be a global problem, mostly affecting the femoral component of the implant [4, 7]. One of the most frequently used UKA implants is the Oxford UKA (Zimmer Biomet) [23]. The femoral component in the Oxford Phase III implant has a spherical shape, with one anchoring peg inserting into the femoral condyle [23]. In 2003, in an attempt to improve the stable fixation and address the loosening problem, the new Oxford Partial implant was introduced with a twin‐peg design. In order to support the extra peg in this new design, they advanced the femoral component 15° to the anterior, providing further support as a result of the larger surface area [2].
The twin‐peg femoral component is associated with a high‐quality outcome and a low incidence of complications, as evidenced by White et al. However, it has not yet been established how implant design changes, surgical expertise, and surgical technique significantly affect the risk of developing long‐term complications when using the twin‐peg Oxford implant [26, 27, 28]. There are a few mid‐ to long‐term follow‐up studies comparing the single‐peg design and the twin‐peg implants. No previous systematic review has compared clinical outcomes of single‐peg and twin‐peg implant designs, and therefore it is uncertain whether there could be any advantage in terms of outcome to the patient. This study aims to provide a comprehensive, systematic review of the literature. It compares clinical and patient‐reported outcome measures (PROMs) between the twin‐peg and single‐peg UKA implant designs. We hypothesized that the twin‐peg UKA implant designs have better clinical outcomes compared to single‐peg designs.
MATERIALS AND METHODS
Search strategy
This study was conducted based on Preferred Reporting Items for Systematic Reviews and Meta‐analyses (PRISMA) guidelines [19]. The study protocol was pre‐registered on the Open Science Framework using an a priori approach at (https://osf.io/bufyx/). A search strategy was applied to four databases, PubMed, Scopus, Embase and Web of Science, using MeSH keywords. All relevant papers were searched without language restrictions and translated if necessary. The search strategy was as follows: (‘unicompartmental knee arthroplasty’ OR ‘unicompartmental knee replacement’ OR ‘Unicondylar knee arthroplasty’ OR ‘Unicondylar knee replacement’ OR ‘UKA’ OR ‘UKR’) AND (‘twin‐peg’ OR ‘twin‐pegged’ OR ‘twin peg’ OR ‘twin pegged’ OR ‘2‐peg’ OR ‘peg’).
Inclusion and exclusion criteria
Studies were only included if they had compared the twin‐peg with single‐peg designs in patients who had undergone UKA. Studies that performed UKA in human cadaver knees were excluded.
Study selection
Two investigators (SM and YK) independently screened the search results, and studies that were not relevant were excluded. Discrepancies in the included studies were resolved through discussions among the reviewers.
Data extraction
For data extraction, data from all included studies were independently extracted by two investigators (SM and YK) using a pre‐established data extraction form, and any disagreements were resolved through discussion. Study characteristics, such as first author, year of publication, country and study type, were included as part of the extracted data. Furthermore, participant‐related information such as age distribution, gender composition, and the number of knees in each group were recorded. Follow‐up duration and outcome measures were also among the extracted information.
Risk of Bias (RoB) assessment
We evaluated randomized controlled trials (RCTs) using the Cochrane RoB 2 tool [25]. The Risk of Bias in Non‐Randomized Studies of Intervention (ROBINS‐I) tool was used to evaluate non‐RCTs (non‐RCTs) [24]. The bias assessment report was visualized using the Risk‐of‐Bias Visualization (Robvis) tool [14].
RESULTS
Selection process of studies
After conducting a search strategy in databases, a total of 242 articles were initially found. After the removal of duplicate articles, 42 unique studies remained. Only studies that compared the single‐peg and twin‐peg implants were retained during title and abstract screening. Following this screening, 14 articles that met the inclusion criteria were proceeded to full‐text review. Finally, full‐text screening was conducted to select studies that met all inclusion criteria. Three studies were conference abstracts, four were cadaveric studies, which were excluded, and ultimately, seven studies were included in this systematic review (Figure 1).
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta‐Analysis.
Study characteristics
The study designs in the seven final articles varied, with two RCTs and five cohort studies [9, 10, 15, 16, 23, 27, 30]. Outcome measures assessed in the studies included implant survival and revision, radiographic differences, as well as patient‐reported outcome questionnaires such as the Oxford Knee Score (OKS), American Knee Society Functional (AKS‐F) score, Western Ontario and McMaster Universities Osteoarthritis score (WOMAC), the Knee Society Score (KSS) and Hospital for Special Surgery (HSS). The study characteristics of these seven final articles included in the systematic review study are summarized in Table 1.
RoB of included studies
The RoB evaluation of the studies using the ROBINS‐I and ROB‐2 checklists demonstrated four low RoB, two moderate RoB and one severe RoB. The reason for this severe RoB in this study was the external control group and the reason for the moderate RoB in two studies was inadequate strategies to manage the missing data. The bias assessment report was illustrated in Figure 2. This shows an overall medium‐quality study.
Risk of bias (RoB) assessment based on ROBINS‐I (a) and RoB‐2 (b). ROBINS‐I, risk of bias in non‐randomized studies of intervention.
Radiographic comparison
Three studies evaluated radiographic scores and measurements in single‐peg and twin‐peg UKA [10, 16, 30]. In these three studies, positioning in the femoral component was the most commonly assessed. Besides that, Hurst et al. assessed alignment in the tibial component [10]. Correlations between functional scores and prosthesis position were also evaluated in the Mosegaard et al. and Zhao et al. studies [16, 30]. Although Hurst et al. [10] demonstrated superior alignment in twin‐peg design, Mosegaard et al. [16] and Zhao et al. [30] found no significant difference in radiological scores.
Clinical outcomes
Seven studies were included in this study. Studies varied in the assessed scores, and some used several PROMs. OKS was the most commonly used PROM in the four studies [9, 16, 27, 30]. Besides OKS, White et al. reported AKS‐F, range of knee motion (ROM), and the Tegner Activity [27], Zhao et al. reported HSS, WOMAC, and KSS [30], and Mosegaard et al. reported KOOS and SF‐36 [16]. Overall results in regard to PROMs were summarized in Table 2.
Implant performance
The comparison of single‐peg and twin‐peg implants shows varying survival and revision rates. The survival of implants was illustrated in three studies [15, 23, 27]. In these studies, excellent survival of twin‐peg prostheses was reported. However, Skaden found no significant differences between the two designs 5 years after the operation [16]. The revision rate was reported in four studies, and data for 638 revisions were provided [15, 16, 23, 27]. Major causes of revision included pain, OA progression, instability, infection, luxation, malalignment and aseptic loosening, which included at least 70% of all revision causes in all cases in this study. Revision rates and major revision causes are presented in Tables 3 and 4. Twin‐peg implants have marginally lower revision rates.
DISCUSSION
The most important findings of this systematic review are that twin‐peg and single‐peg UKA designs demonstrate comparable clinical outcomes, PROMs and radiographic results, with no conclusive evidence supporting the superiority of one design over the other. While some studies suggested advantages for twin‐peg designs regarding component positioning and slightly lower revision rates, these differences were inconsistent across all included studies.
The investigations of radiographic outcomes in Mosegaard et al. and Zhao et al. revealed no significant differences in femoral component positioning between the single‐peg and twin‐peg designs [16, 30], but Horsager et al. showed a significant difference [9]. The reason for this controversy is that Horsager et al. measured radiographic outcomes in the short term, but the other two studies had mid‐ to long‐term follow‐up times. This is consistent with findings of previous research by D'Ambrosi et al., which found that design modifications did not significantly affect radiographic outcomes [2].
Clinical outcomes evaluated using various PROMs showed mixed findings. In some studies, such as those conducted by Horsager et al., Zhao et al. and Mosegaard et al., some improvements in twin‐peg implants compared to single‐peg implants were reported, but they were not statistically significant. On the other hand, White et al. indicated significant improvements in clinical scores, but the possible reason for that is an external single‐peg group as the control group, which may result in some bias [27]. This aligns with the findings by Murray and Parkinson, who highlighted that while newer implant designs show promise, they often do not demonstrate substantial clinical benefits over established designs in broad patient populations [18].
The twin‐peg design offered a slight advantage in terms of implant survivorship and revision rates. Multiple included studies reported lower revision rates for twin‐peg implants, and Mohammad et al. found significant differences in the revision rate between these two implants [15]. In contrast, Skaden et al. did not find statistically significant differences in survival rates. This indicates that while the twin‐peg design could have some advantages, it does not always result in improved clinical performance [23]. Differences in surgical technique, patient demographics, and follow‐up time in the studies can explain this different outcome.
According to the RoB assessment, many included studies categorized as moderate quality, but the methodological heterogeneities, such as differences in study designs, patient populations, outcome measures, scoring systems and follow‐up durations, made it difficult to reach a definitive conclusion. Also, in many primary studies, the differences between these two implant designs in terms of different scores and other clinical outcomes were not identified as significant, which indicates that other variables besides the implant design may influence patient outcomes. Generally, in different studies, the twin‐peg design has seemed to have some advantages and also lower revision rates compared to the single‐peg design, but the improved clinical outcomes are not consistent for all individuals regarding clinical improvements. Therefore, surgeons need to consider patient‐specific variables, such as preoperative knee function, activity level and comorbidities, when choosing between single‐peg and twin‐peg implant designs. Also, future research should be conducted with a longer follow‐up duration and RCTs with a larger sample size to increase the certainty of the evidence of the long‐term benefits of the twin‐peg design and optimize UKA outcomes.
Since the 1970s, the cemented Oxford UKA has been in clinical use, yielding good clinical outcomes [17]. The cementless UKA was introduced in an attempt to improve the fixation of the implant and lower the revision rate, which is mainly due to aseptic loosening. The difference between the cementless and cemented implants is the porous titanium having a hydroxyapatite coating, which is placed on a small additional peg on the femoral component [11]. Comparing different implants regarding their fixation method and design at the same time is challenging. Among the seven studies included in this study, three compared twin‐peg designs concerning cement [9, 16, 23]. Comparing the uncemented twin‐peg to the cemented twin‐peg, we discovered a greater chance of revision for periprosthetic fracture, infection and polyethylene wear for the uncemented design [12, 23]. However, Horsager et al. found no significant differences in polyethylene wear between cemented and cementless twin‐peg UKAs and also no comparison was made between cemented or cementless single‐peg designs [9]. Periprosthetic fracture has been reported as the most common cause of revision in the cementless version of twin‐peg [23]. Nevertheless, the results of this study provide the basis for additional studies, including prospective RCTs comparing cementless and cemented implant fixation in each design group and also with each other.
In our study, we only included clinical studies, but the literature also included cadaver studies. To give examples, Reiner conducted two studies in 2014 and 2018 [21, 22]. In the study conducted in 2014, he found no significant difference between the stability of the two designs of femoral components with respect to micromotion or subsidence under cyclical loading. In the study year 2018, it was determined that the maximum load to failure was higher in the twin‐peg group compared to the single‐peg group, which can be explained by the additional peg, which leads to stronger implant fixation at the cement‐bone interface [21, 22]. In Eckert et al.'s 2022 study, the single‐peg showed higher compression at 70° flexion, whereas the twin‐peg design showed higher compression at 115°, and the probable reason for that may be the increasing surface contact and distribution of forces might increase mechanical stability at higher degrees of flexion (115°) with the twin‐peg design. In contrast, the single‐peg design may not distribute forces as effectively, resulting in higher compression at lower flexion angles (70°). Also, X‐displacement was significantly higher for the single‐peg at 115°, which is probably due to the fact that in the case of single‐peg designs, additional anchoring points in the knee structure may be insufficient to provide sufficient stability when the knee is flexed at higher angles [5].
This systematic review helps surgeons choose between twin‐peg and single‐peg UKA designs based on patient‐specific factors and surgical goals. Twin‐peg designs showed slightly better component positioning and lower revision rates, but overall evidence did not strongly favour one design. Both designs provide significant pain relief and functional improvement, with no clear superiority in patient satisfaction. However, surgeons should be cautious about the slightly higher risk of aseptic loosening with single‐peg designs, especially in patients with poor bone quality or requiring long‐term durability.
This systematic review has several limitations that should be acknowledged. First, the included studies exhibited methodological heterogeneity, including variations in study designs, patient demographics, outcome measures, and follow‐up durations, which made it challenging to draw definitive conclusions. Second, the RoB assessment revealed that some studies had moderate to severe RoB, potentially affecting the reliability of the findings. Third, the small number of included studies (n = 7) and the lack of long‐term follow‐up data in many of them limited the ability to assess the durability and long‐term performance of the twin‐peg and single‐peg designs. Additionally, the focus on Zimmer Biomet implants may limit the generalizability of the findings to other UKA designs. Finally, the absence of RCTs with large sample sizes further restricts the strength of the evidence.
CONCLUSION
The study compared single‐peg and twin‐peg UKA designs, finding no clinical differences. While some studies showed twin‐peg designs were better in positioning and alignment, no significant differences were found. Functional outcomes showed improvements in both designs, but no clear preference was found.
AUTHOR CONTRIBUTIONS
All authors contributed substantially to this study. Also, all authors read and approved the final manuscript. Amir Mehrvar was the supervisor and formed the research question. Study selection, risk of bias assessment and data extraction: Sadra Mohebbi and Yashar Khani. Preparation of the first draft of the paper: Mohammadhossein Hefzosseheh and Mahya Aliakbari. Critical revision of the first draft: Elias Sadooghi Rad and Sadra Mohebbi. Designing the methodological aspects of the study: Fateme Rezagholi and Yashar Khani.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
ETHICS STATEMENT
The ethics statement is not available.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Canovas F , Dagneaux L . Quality of life after total knee arthroplasty. Orthop Traumatol Surg Res. 2018;104(1S):41–46.10.1016/j.otsr.2017.04.01729183821 · doi ↗ · pubmed ↗
- 2D'Ambrosi R , da Silva MJSV , Moura JLM , Mariani I , Serrao LD , Di Feo F , et al. Radiographic and clinical evolution of the Oxford unicompartmental knee arthroplasty. J Knee Surg. 2023;36(3):246–253.34520561 10.1055/s-0041-1731718 · doi ↗ · pubmed ↗
- 3Delanois RE , Mistry JB , Gwam CU , Mohamed NS , Choksi US , Mont MA . Current epidemiology of revision total knee arthroplasty in the United States. J Arthroplasty. 2017;32(9):2663–2668.28456561 10.1016/j.arth.2017.03.066 · doi ↗ · pubmed ↗
- 4Dyrhovden GS , Lygre SHL , Badawy M , Gøthesen Ø , Furnes O . Have the causes of revision for total and unicompartmental knee arthroplasties changed during the past two decades? Clin Orthop Relat Res. 2017;475(7):1874–1886.28299718 10.1007/s 11999-017-5316-7PMC 5449334 · doi ↗ · pubmed ↗
- 5Eckert JA , Bitsch RG , Sonntag R , Reiner T , Schwarze M , Jaeger S . The primary stability of the femoral component in cemented single and twin peg Oxford unicompartmental knee arthroplasty under adverse conditions. Bone Joint Res. 2022;11(2):82–90.35124977 10.1302/2046-3758.112.BJR-2020-0507.R 2PMC 8882328 · doi ↗ · pubmed ↗
- 6Ekhtiari S , Bozzo A , Madden K , Winemaker MJ , Adili A , Wood TJ . Unicompartmental knee arthroplasty: survivorship and risk factors for revision: a population‐based cohort study with minimum 10‐year follow‐up. J Bone Joint Surg Am. 2021;103:2170–2176.34547009 10.2106/JBJS.21.00346 · doi ↗ · pubmed ↗
- 7Furnes O , Espehaug B , Lie SA , Vollset SE , Engesæter LB , Havelin LI . Failure mechanisms after unicompartmental and tricompartmental primary knee replacement with cement. J Bone Joint Surg. 2007;89(3):519–525.17332100 10.2106/JBJS.F.00210 · doi ↗ · pubmed ↗
- 8Ho KKW , Lau LCM , Chau WW , Poon Q , Chung KY , Wong RMY . End‐stage knee osteoarthritis with and without sarcopenia and the effect of knee arthroplasty—a prospective cohort study. BMC Geriatr. 2021;21(1):2.33397330 10.1186/s 12877-020-01929-6PMC 7784022 · doi ↗ · pubmed ↗