Biomarkers for primary graft dysfunction after lung transplantation: a review of current evidence and future prospects
Li Feng, Kelin Luo, Yu Qiu, Rui Li, Chun Xue, Shuaishuai Xi, Jixian Liu, Yuanmin Pei, Chao Ma

TL;DR
This paper reviews current biomarkers for predicting and diagnosing lung transplant complications, highlighting the need for better diagnostic tools.
Contribution
The paper provides a comprehensive review of recent advances in PGD-related biomarker discovery and emphasizes the need for clinical validation.
Findings
PGD is a major cause of early mortality after lung transplantation.
Multiple biomarker candidates have been identified but lack sufficient predictive power for clinical use.
Integration of biomarkers into clinical practice requires further validation and optimized strategies.
Abstract
Lung transplantation remains the only effective treatment for end-stage lung disease, offering the potential to significantly prolong survival and enhance quality of life for recipients. However, primary graft dysfunction (PGD)-a severe form of lung injury occurring within the first 72 h post-transplantation-constitutes a major cause of early mortality and presents a substantial barrier to the broader clinical adoption of lung transplantation. Biomarkers, defined as specific molecules, cells, or other biological indicators detectable within or outside the body, can reflect physiological states, disease progression, or therapeutic responses. The identification of accurate and reliable biomarkers for the prediction and diagnosis of PGD is therefore critical for improving diagnostic precision and therapeutic outcomes. This review provides a comprehensive overview of recent advances in the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
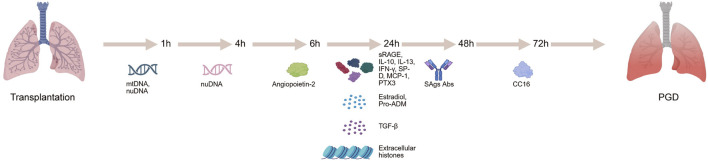 FIGURE 1
FIGURE 1| Biomarker | Biological fucntion | Number of patients | Single/multi-center | Time points of biomarker detection after lung transplantation (/h) | With PGD | Without PGD | Detection method | References |
|---|---|---|---|---|---|---|---|---|
| Plasma Proteins | ||||||||
| sRAGE | Soluble receptor | 317 | multi-center | 24 | 4.3 ng/mL | 1.9 ng/mL | Sandwich ELISA |
|
| IL-10 | Anti-inflammatory cytokine | 80 | single-center | 24 | 3(PGD1)/5.5(PGD2)/10.9(PGD3) pg/mL | 2 pg/mL | ELISA |
|
| IL-13 | Inflammatory cytokine | 80 | single-center | 24 | 0.2(PGD1)/1(PGD2)/0.9(PGD3) pg/mL | 0.7 pg/mL | ELISA |
|
| IFN-γ | Immune response regulator | 80 | single-center | 24 | 5.7(PGD1)/8.4(PGD2)/11.5(PGD3) pg/mL | 4.8 pg/mL | ELISA |
|
| SP-D | Pulmonary surfactant | 80 | single-center | 24 | 3841(PGD1)/4247(PGD2)/3263(PGD3) pg/mL | 6001 pg/mL | ELISA |
|
| CC16 | Secretory protein | 104 | multi-center | 72 | 13.8 ng/mL | 8.2 ng/mL | Sandwich ELISA |
|
| MCP-1 | Chemotactic factor | 108 | multi-center | 24 | 167.95 pg/mL | 103.5 pg/mL | ELISA |
|
| Angiopoietin-2 | Vascular growth stimulator | 119 | multi-center | 6 | 4578 pg/mL | 3218 pg/mL | ELISA |
|
| VEGF | Angiogenesis factor | 150 | single-center | 72 | 584(PGD1)/829(PGD2)/1191(PGD3)/pg/mL | 428 pg/mL | ELISA |
|
| PTX3 | Complement system regulator | 119 | multi-center | 24 | 88.9 ng/mL | 22.7 ng/mL | Sandwich ELISA |
|
| Hormones | ||||||||
| Estradiol | Estrogen | 111 | multi-center | 24 | 77.4 pg/mL | 59.6 pg/mL | ELISA |
|
| Pro-ADM | Precursor of adrenomedullin | 100 | single-center | 24 | 3.25 nmol/L | 1.61 nmol/L | An immune time-resolved amplified cryptate emission technology assay |
|
| Cell-free DNA | ||||||||
| cfDNA | Fragmented DNA | 186 | multi-center | NA | 23.7 ng/mL | 12.9 ng/mL | Quantitative PCR |
|
| mtDNA | Mitochondrial DNA | 62 | single-center | 1 | 1874 copies/μL | 1259 copies/μL | Quantitative PCR |
|
| nuDNA | Nuclear DNA | 62 | single-center | 1 | 1895 copies/μL | 675 copies/μL | Quantitative PCR |
|
| nuDNA | Nuclear DNA | 62 | single-center | 4 | 4521 copies/μL | 1764 copies/μL | Quantitative PCR |
|
| %ddcfDNA | Percentage donor-derived cell-free DNA | 99 | multi-center | 72 | 12.2% | 8.5% | An automated shotgun sequencing method |
|
| Immunoreactive Substances | ||||||||
| TGF-β | Cytokine | 279 | single-center | 24 | - | - | ELISA |
|
| SAgs Abs | lung-associated self-antigen antibodies | 317 | multi-center | 48 | - | - | ELISA |
|
| Others | ||||||||
| Extracellular histones | Cytotoxic proteins | 65 | single-center | 24 | 5.882 μg/ml | 2.478 μg/ml | Sandwich ELISA |
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTransplantation: Methods and Outcomes · Renal Transplantation Outcomes and Treatments · Organ Transplantation Techniques and Outcomes
Introduction
Lung transplantation remains an effective treatment for end-stage lung diseases, although its success is often limited by primary graft dysfunction (PGD) (Shah and Diamond, 2018; Young and Dilling, 2019; Avtaar Singh et al., 2023). PGD presents as a severe form of lung injury within the first 72 h after transplantation and is characterized by hypoxemia, pulmonary edema, and decreased pulmonary compliance (Criner et al., 2021). With an incidence rate as high as 30%–50%, PGD is strongly associated with both early and long-term post-transplant mortality (Hunt and Cantu, 2023). Currently, there is a lack of reliable biomarkers and pharmacological treatments for PGD, making early diagnosis and intervention challenging. Therefore, identifying biomarkers that can predict, diagnose, and potentially guide treatment for PGD is a pressing need in the field of lung transplantation.
Biomarkers are substances that reflect physiological or pathological states and can be detected in bodily fluids such as blood, urine, bronchoalveolar lavage fluid (BALF), or organ perfusate to evaluate organ function or injury (Calfee and Ware, 2007; Chacon-Alberty et al., 2022; Hamilton et al., 2017; Nakata et al., 2023). In recent years, advances in molecular biology, proteomics, and metabolomics have led to some progress in identifying potential PGD biomarkers. However, challenges remain, including small sample sizes, inconsistent findings, and a lack of thorough validation.
This review aims to summarize current research on PGD biomarkers, including plasma proteins, hormones, cell-free DNA, and immunoreactive substances. It discusses their advantages, limitations, and potential clinical applications, while also highlighting the challenges and future directions in biomarker discovery for PGD.
Primary graft dysfunction and biomarkers
Biomarkers are substances that reflect physiological or pathological states, including genes, proteins, metabolites, and cytokines (Lozano-Edo et al., 2022; Lee and Christie, 2011; Suzuki et al., 2013). They can be detected in bodily fluids such as blood, urine, BALF, or organ perfusate, and are used to assess organ function or the extent of injury. PGD is one of the most common complications following lung transplantation, significantly affecting patient survival and quality of life (Wu et al., 2023). As such, identifying reliable biomarkers for the early prediction and accurate diagnosis of PGD remains a critical goal in the field. Despite encouraging progress, most studies on PGD biomarkers have been limited by relatively small sample sizes, and further research is needed to validate these findings for clinical use. Currently, PGD diagnosis primarily depends on the oxygenation index, chest radiographs, and clinical judgment (Sanchez-Gonzalez et al., 2022; Li et al., 2021; Neves et al., 2016). However, these methods often lack sensitivity and specificity, and may not effectively capture the onset or resolution of PGD. The discovery of biomarkers capable of predicting PGD risk, monitoring its progression, and guiding treatment strategies holds substantial clinical promise (Figure 1). Advancing biomarker research could ultimately transform the diagnosis, management, and outcomes of PGD in lung transplant recipients. Table 1 summarizes the detailed information of biomarkers for PGD following lung transplantation.
Identification of biomarkers in primary graft dysfunction can be evaluated at different time points in lung transplantation recipients.
Plasma proteins
Plasma proteins are essential for maintaining homeostasis, facilitating substance transport, supporting immune defense, and regulating coagulation (Christie et al., 2009; Covarrubias et al., 2007; Leon et al., 2009). A retrospective analysis examined the relationship between plasma cytokine levels before and after lung transplantation and the severity of PGD (Frick et al., 2020). Of the 30 proteins tested, eight showed significant differences between patients with mild and severe PGD: IL-6, IL-10, IL-13, eotaxin, G-CSF, IFN-γ, MIP-1α, and SP-D. Notably, IL-10 and IL-13 were associated with prolonged extubation times, extended ICU stays, and longer overall hospitalizations, independent of donor and recipient characteristics. Plasma IL-10 and IFN-γ levels in both donors and recipients correlated positively with PGD incidence and severity, whereas SP-D levels were inversely correlated with PGD severity.
Patients with PGD typically exhibit elevated levels of inflammatory mediators in early post-transplant serum, such as MCP-1, IP-10, IL-1β, IL-2, IFN-γ, and IL-12 (21). Further investigations revealed that PGD-induced inflammation may enhance donor HLA class II antigen expression on the graft, increase antigen presentation, and stimulate donor-specific immune responses (Bharat et al., 2008).
In a multicenter cohort study, protein C and plasminogen activator inhibitor-1 (PAI-1) levels were measured in the plasma of lung transplant recipients (Christie et al., 2007). Those who developed PGD had significantly lower post-transplant protein C levels and higher PAI-1 levels compared to those without PGD. Pre-transplant pulmonary artery systolic pressure was positively correlated with post-transplant PAI-1 levels, potentially linking pulmonary hypertension to PGD development.
Another study collected blood samples from lung transplant recipients before surgery and at 6, 24, 48, and 72 h post-transplant to evaluate plasma ICAM-1 and von Willebrand factor (vWF) levels (Covarrubias et al., 2007). ICAM-1 is a cell adhesion molecule predominantly expressed on the surface of endothelial and immune cells (Singh et al., 2023; Bui et al., 2020; van de Stolpe and van der Saag, 1996). It plays a critical role in the inflammatory response by interacting with integrins on leukocytes, thereby facilitating their adhesion and migration across the endothelium. This process promotes the infiltration of inflammatory cells into injured tissues. vWF is a large glycoprotein synthesized and secreted by endothelial cells (Zanetta et al., 2000; Xiang and Hwa, 2016; Nakhaei-Nejad et al., 2019). It is primarily involved in hemostasis, contributing to blood coagulation and platelet aggregation. ICAM-1 levels were significantly higher in patients with PGD and positively correlated with PGD occurrence. Although vWF levels tended to rise postoperatively, they were not significantly associated with PGD. ICAM-1 levels also correlated with pre-transplant pulmonary artery pressure and recipient diagnosis (Covarrubias et al., 2007).
CC16, a protein secreted by airway epithelial cells, has been significantly associated with PGD, particularly in recipients without idiopathic pulmonary fibrosis (non-IPF) (Diamond et al., 2011a). Produced by non-ciliated pulmonary epithelial cells, CC16 may serve as a biomarker for epithelial injury (Shah et al., 2014). In a prospective cohort, CC16 levels at 6 h post-transplant were notably higher in PGD patients, and a 15 ng/mL increase in CC16 was linked to a 1.6-fold higher PGD risk. Additionally, MCP-1, a chemotactic protein released by pulmonary epithelial cells, plays a key role in recruiting inflammatory cells and mediating ischemia-reperfusion injury (IRI) (Yoshimura, 2018; Singh et al., 2021; Ferreira et al., 2005). Elevated MCP-1 levels at 24 h post-transplant were positively correlated with PGD risk and severity within 72 h (Shah et al., 2012).
Angiopoietin-2 (Ang2), a vascular growth stimulator involved in angiogenesis, binds to the TIE2 receptor and acts as a negative regulator of the ANG1/TIE2 signaling pathway, modulating endothelial responses to cytokines (Akwii et al., 2019; Scholz et al., 2015; Song et al., 2012; Eklund et al., 2017; Nicolini et al., 2019). In PGD patients, Ang2 plasma levels changed significantly over time, particularly in those with idiopathic pulmonary fibrosis (IPF), but showed no significant association in chronic obstructive pulmonary disease (COPD) patients (Diamond et al., 2017).
Vascular endothelial growth factor (VEGF), a key regulator of vascular permeability, was evaluated preoperatively in lung transplant patients (Guzmán et al., 2023; Shi et al., 2022). VEGF serum levels were significantly higher in patients who developed grade 3 PGD compared to those with lower-grade PGD or healthy controls. Elevated VEGF levels were predictive of more severe PGD outcomes (Krenn et al., 2007).
Long pentraxin-3 (PTX3), a protein involved in complement activation and regulation, has also been linked to PGD (Cieślik and Hrycek, 2012; Chiari et al., 2023). In IPF recipients, PTX3 levels at 6 and 24 h post-transplant correlated positively with PGD risk (Diamond et al., 2011b). Genetic analysis in lung transplant recipients identified two PTX3 gene polymorphisms associated with increased PGD risk (Diamond et al., 2012).
The receptor for advanced glycation end-products (RAGE), a transmembrane protein of the immunoglobulin superfamily, has a soluble form (sRAGE) that includes its extracellular domain (Eva et al., 2022; Yue et al., 2022; Bongarzone et al., 2017). sRAGE levels measured at 6 and 24 h post-transplant were higher in PGD patients. These levels were influenced by right heart pressure and cardiopulmonary bypass and were associated with red blood cell transfusion and bypass usage (Kim T. et al., 2023).
Hormones
Prostaglandin E2 (PGE2) is a hormone-like lipid compound that plays a key role in numerous physiological processes, including smooth muscle contraction and relaxation, vasodilation and vasoconstriction, blood pressure regulation, and the modulation of inflammation (Képes et al., 2023; Cheng et al., 2021; Finetti et al., 2020; Finetti et al., 2023). In a large-scale gene association study, 17 genetic variants were significantly linked to PGD, four of which were located within genes related to the PGE2 pathway (Diamond et al., 2014). One notable variant involved a coding change in the PTGES2 gene, resulting in the substitution of arginine with histidine at position 298, which was associated with an increased risk of PGD. The other three variants were found in the promoter region and first intron of the PTGER4 gene and were associated with a decreased risk of PGD. Functional analysis showed that the rs4434423A variant in PTGER4 influenced the inhibitory function of regulatory T cells.
In another study, plasma estradiol levels were measured before transplantation and at 6 and 24 h post-transplantation to assess their relationship with PGD severity within 72 h after surgery. While no significant differences were found between male and female recipients overall, a positive correlation between estradiol levels at 24 h and PGD severity was observed in male recipients. This association was not present in female recipients (Bastarache et al., 2012).
Pro-adrenomedullin (pro-ADM), a precursor of adrenomedullin (ADM), has been identified as a potential biomarker in various acute conditions such as sepsis, acute heart failure, cardiac arrest, and stroke (Liang et al., 2023; Hagag et al., 2011; Spoto et al., 2023; Zelniker et al., 2023; Ishiyama et al., 2023). It reflects the rapid breakdown of ADM in circulation. In a prospective study of lung transplant recipients, pro-ADM levels were measured at 24, 48, and 72 h following ICU admission (Riera et al., 2016). Findings indicated that pro-ADM levels were strongly correlated with PGD severity and positively associated with ICU mortality. Patients with PGD grade 3 exhibited significantly higher pro-ADM levels at 72 h. Furthermore, pro-ADM levels measured at 24 h could predict the development of PGD grade 3 by 72 h. The predictive value of pro-ADM for ICU mortality surpassed that of PGD grading alone, and combining both enhanced prognostic accuracy. Elevated pro-ADM levels were strongly linked to early graft dysfunction and post-transplant mortality.
Endothelin-1 (ET-1) is a potent peptide hormone known for its vasoconstrictive and proliferative effects and plays a critical role in the pathogenesis of various pulmonary diseases (Banecki and Dora, 2023; Salama et al., 2010). In a study analyzing lung tissue and serum samples from lung transplant donors and recipients, both ET-1 mRNA expression in lung tissue and serum ET-1 concentrations were positively correlated with the severity of PGD(65).
Follistatin-like protein 1 (FSTL1) is a secretory glycoprotein involved in multiple biological functions, including the regulation of myocardial ischemia-reperfusion injury, airway remodeling, and inflammatory responses (Veraar et al., 2022; Kim DK. et al., 2023; Chiou et al., 2019). In a prospective cohort of bilateral lung transplant recipients with end-stage lung disease, post-transplant elevations in plasma FSTL1 levels were identified, showing significant associations with the incidence and clinical severity of PGD(66).
Cell-free DNA
Cell-free DNA (cfDNA) refers to the free DNA fragments existing in the extracellular environment (Valpione et al., 2018; Mattox et al., 2023). It mainly originates from apoptosis, necrosis, inflammatory responses, and tumor cells. Present in bodily fluids such as blood, saliva, and urine in the form of short fragments, cfDNA is characterized by its diverse sources, fragmentation, and short half-life (Bruhm et al., 2025; Hu et al., 2021; Sherwood and Weimer, 2018). Under normal physiological conditions, the concentration of cfDNA in the bloodstream of healthy individuals remains relatively low. However, in conditions that accelerate cell turnover, such as acute or chronic inflammation, cfDNA levels can rise significantly. Given its short half-life-typically less than one to two hours-cfDNA can serve as a real-time biomarker for disease. By distinguishing between donor- and recipient-specific single nucleotide polymorphisms (SNPs), the origin of circulating cfDNA can be determined, enabling the detection of donor-derived cfDNA. This has potential applications in identifying graft injury following transplantation (Magnusson et al., 2022; Li and Liang, 2023; Zou et al., 2017; Keller and Agbor-Enoh, 2021; Balasubramanian et al., 2024; Ju et al., 2023; Keller et al., 2022a; Keller et al., 2024; Kim et al., 2024; Keller et al., 2022b; Zhang et al., 2024; Keller MB. et al., 2022).
In lung transplant recipients, cfDNA levels are almost twice as high as those observed in healthy individuals, primarily originating from innate immune cells involved in inflammatory responses (Keller and Agbor-Enoh, 2022). Elevated cfDNA levels prior to transplantation are associated with a heightened risk of post-transplant pulmonary edema (such as PGD) and mortality. These levels also show potential in predicting both early and long-term complications, such as PGD, chronic lung allograft dysfunction (CLAD), and death, making cfDNA a promising molecular tool for risk stratification in transplant recipients (Keller et al., 2024; Keller and Agbor-Enoh, 2022).
Analysis of perfusate from donor lungs at one and 4 hours of perfusion revealed significantly higher levels of cfDNA-including mitochondrial DNA (mtDNA) and nuclear DNA (nuDNA)-in lungs that later developed severe PGD (grade 3) within 72 h after transplantation, particularly those from donation after circulatory death (DCD) donors. While cfDNA shows promise as a predictive marker for PGD, its diagnostic accuracy still requires further refinement (Kanou et al., 2021).
In a prospective study involving lung transplant recipients, plasma samples collected on days 1, 3, and 7 post-transplantation revealed that patients who developed PGD had elevated levels of percentage donor-derived cell-free DNA (%ddcfDNA). These levels correlated positively with the severity of PGD. Furthermore, PGD patients with higher %ddcfDNA levels were at increased risk for developing CLAD. Notably, %ddcfDNA levels in PGD patients who progressed to CLAD were approximately double those in PGD patients who did not develop CLAD (Keller et al., 2021).
Immunoreactive substances
Surfactant protein A (SP-A) is a key pulmonary surfactant involved in immune defense and the regulation of inflammation in the lungs (D'Ovidio et al., 2013; Depicolzuane et al., 2021; King and Chen, 2020). Low expression of SP-A mRNA in donor lungs has been significantly associated with reduced post-transplant survival. After transplantation, recipients with low SP-A mRNA levels show decreased SP-A concentrations in BALF, elevated levels of IL-2 and IL-12, and an increased incidence of rejection episodes (D'Ovidio et al., 2013).
Elevated levels of CCR5 and its ligands have been observed in both mouse and human models of ischemia-reperfusion injury (IRI). CCR5-positive natural killer (NK) cells accumulate in the lungs and airways, exhibiting markers of maturity and tissue residency. The CCR5 antagonist maraviroc has been shown to reduce NK cell migration to the airways, decrease pulmonary vascular permeability, improve oxygenation, and lower the incidence and severity of PGD (Santos et al., 2023).
Dectin-1, a C-type lectin receptor, plays a role in recognizing and activating a variety of ligands, including β-glucans, endogenous damage-associated molecular patterns (DAMPs), and fungal pathogen-associated molecular patterns (PAMPs) (Ochoa et al., 2023; Drummond et al., 2022; Yang et al., 2023). It is involved in modulating inflammatory responses and immune tolerance. A specific Dectin-1 mutation (Y238X) has been linked to acute rejection after lung transplantation, increased lymphocyte proportions in BALF, the development of bronchiolitis obliterans syndrome (BOS) (Calabrese et al., 2019). Additionally, levels of transforming growth factor-beta (TGF-β) increase during PGD and are associated with BOS development. Immunohistochemistry has revealed TGF-β expression in epithelial cells, interstitial cells, and macrophages in transplanted lungs, suggesting that TGF-β may serve as a critical mediator linking PGD and BOS, and could potentially function as a biomarker for both conditions (DerHovanessian et al., 2016).
In a large cohort of lung transplant recipients, patients were grouped by underlying conditions-such as COPD, IPF, and cystic fibrosis (CF)-to investigate the relationship between antibodies against lung-associated self-antigens (SAgs) and PGD. The highest pre-transplant positivity rates for SAg antibodies were observed in the IPF and CF groups. Recipients with pre-existing SAg antibodies exhibited higher rates of PGD and elevated serum levels of inflammatory cytokines (Tiriveedhi et al., 2013).
Type V collagen (col(V)), primarily located at the apex of lung epithelial cells, has been shown to induce complement-dependent cytotoxicity (Mak et al., 2016; Iwata et al., 2008; Zaffiri et al., 2019). In lung transplant recipients, high pre-transplant plasma levels of anti-col(V) antibodies have been significantly associated with severe PGD following surgery. Lung-restricted autoantibodies (LRAs) are recognized as important pathogenic contributors to PGD, with mechanisms involving IL-1β-mediated increases in pulmonary vascular endothelial permeability and activation of the complement cascade. These findings offer promising targets for preventive and therapeutic strategies (Yang et al., 2022).
Genetic studies have identified a variant (rs3168046) in the Toll-interacting protein (TOLLIP) gene that is significantly associated with PGD, as well as with plasma levels of plasminogen activator inhibitor-1 (PAI-1) (Cantu et al., 2016). Additionally, two IL-17 receptor (IL-17R) gene variants (rs882643 and rs2241049) have been linked to increased risk of PGD, with carriers of the risk genotypes more likely to experience higher PGD grades within the first 48 h post-transplantation (Somers et al., 2015).
Others
Extracellular histones are a novel class of highly tissue-damaging molecules released during cell death and the formation of neutrophil extracellular traps (NETs). These molecules exhibit diverse biological activities, including cytotoxic effects, promotion of inflammation, and enhancement of platelet aggregation (Jin et al., 2020; de Vries et al., 2023; Zhong et al., 2023). Following lung transplantation, extracellular histone levels increase significantly, particularly in patients who develop PGD. In vitro studies have shown that serum collected within 24 h post-transplantation from patients with high extracellular histone levels is markedly toxic to human pulmonary artery endothelial cells (HPAECs) and stimulates cytokine production in human monocytic cell lines (THP1). These effects are largely mitigated by heparin or anti-histone antibodies (Jin et al., 2020).
Telomere length in airway epithelial cells has also been associated with PGD severity (Greenland et al., 2023). In one analysis of lung transplant recipients, a negative correlation was observed between telomere length in airway epithelial cells and the severity of PGD within the first few weeks after transplantation. Further evidence suggests that PGD may contribute to telomere dysfunction, thereby enhancing immune activation. Telomere impairment in airway epithelial cells may represent a mechanistic link between PGD and the later development of CLAD (Spahn et al., 2015).
The transient receptor potential vanilloid 4 (TRPV4) channel in endothelial cells has emerged as a key mediator of lung IRI. Inhibition or genetic deletion of TRPV4 significantly improves pulmonary function, reduces pulmonary edema and inflammatory cell infiltration, and lowers levels of inflammatory cytokines. These findings suggest that TRPV4 channels may serve as promising therapeutic targets for preventing PGD after lung transplantation (Kuppusamy et al., 2023; Weber et al., 2020).
Limitations and future prospects
Although numerous biomarkers associated with PGD have been identified, most current studies are limited by small sample sizes and a lack of multicenter validation. Therefore, there is an urgent need for further research to identify biomarkers with high sensitivity and specificity, and to develop standardized detection methods and diagnostic criteria.
PGD is a dynamic and evolving condition, with biomarker levels fluctuating over time to reflect different pathophysiological mechanisms and prognostic implications. Thus, determining the optimal timing and frequency for biomarker collection, as well as defining clinically relevant thresholds, is crucial for early prediction and real-time monitoring. However, threshold values for biomarkers vary across studies, which may be due to differences in sample sizes, study designs, detection methods, and patient populations. The biomarkers highlighted in this review offer advantages such as higher sensitivity, stronger specificity, and the ability to guide therapeutic adjustments. For instance, cytokines like IL-10 and IL-13 show significantly elevated levels in early post-transplant serum and are closely associated with PGD severity. These changes often precede the appearance of clinical symptoms, enabling physicians to identify high-risk patients before PGD fully develops. Additionally, certain biomarkers are closely linked to the pathogenesis of PGD and demonstrate high specificity. For example, SP-A, which plays a key role in pulmonary immune defense and inflammation regulation, has been shown to correlate with reduced post-transplant survival when expressed at low levels in donor lungs. Such biomarkers, directly involved in the pathogenesis of PGD, more accurately reflect post-transplant pathological states and reduce the risk of misdiagnosis.
Furthermore, monitoring biomarker fluctuations allows clinicians to more precisely assess PGD severity and progression, facilitating timely therapeutic adjustments. For example, elevated levels of circulating cfDNA are strongly associated with both the occurrence and severity of PGD, as well as an increased risk of CLAD. By measuring cfDNA levels, physicians can identify patients at risk of developing CLAD in advance and implement appropriate preventive or therapeutic strategies.
Given the complexity and heterogeneity of PGD, a single biomarker may be insufficient for accurate diagnosis or prognosis. Therefore, combining and integrating multiple biomarkers may improve diagnostic precision. Advanced analytical approaches, such as multivariate statistical analyses and machine learning, can support the development of composite scoring systems or predictive models. Currently, most biomarker detection methods rely on ELISA and quantitative PCR, which are cost-effective and easily implemented. However, detection methods for some emerging biomarkers are still under development.
Biomarkers not only serve diagnostic and prognostic roles but may also act as therapeutic targets. Future research should focus on elucidating the functional roles, regulatory mechanisms, and detection strategies of these biomarkers, paving the way for effective prevention and treatment strategies for PGD.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Akwii R. G.Sajib M. S.Zahra F. T.Mikelis C. M. (2019). Role of angiopoietin-2 in vascular physiology and pathophysiology. Cells 8 (5), 471. 10.3390/cells 8050471 31108880 PMC 6562915 · doi ↗ · pubmed ↗
- 2Avtaar Singh S. S.Das De S.Al-Adhami A.Singh R.Hopkins P. M.Curry P. A. (2023). Primary graft dysfunction following lung transplantation: from pathogenesis to future frontiers. World J. Transpl. 13 (3), 58–85. 10.5500/wjt.v 13.i 3.58 PMC 1003723136968136 · doi ↗ · pubmed ↗
- 3Balasubramanian S.Richert M. E.Kong H.Fu S.Jang M. K.Andargie T. E. (2024). Cell-free DNA maps tissue injury and correlates with disease severity in lung transplant candidates. Am. J. Respir. Crit. Care Med. 209 (6), 727–737. Epub 2023/12/20. 10.1164/rccm.202306-1064 OC 38117233 PMC 10945061 · doi ↗ · pubmed ↗
- 4Banecki KMRM Dora K. A. (2023). Endothelin-1 in Health and disease. Int. J. Mol. Sci. 24 (14), 11295. 10.3390/ijms 241411295 37511055 PMC 10379484 · doi ↗ · pubmed ↗
- 5Bastarache J. A.Diamond J. M.Kawut S. M.Lederer D. J.Ware L. B.Christie J. D. (2012). Postoperative estradiol levels associate with development of primary graft dysfunction in lung transplantation patients. Gend. Med. 9 (3), 154–165. 10.1016/j.genm.2012.01.009 22361838 PMC 3374892 · doi ↗ · pubmed ↗
- 6Bharat A.Kuo E.Steward N.Aloush A.Hachem R.Trulock E. P. (2008). Immunological link between primary graft dysfunction and chronic lung allograft rejection. Ann. Thorac. Surg. 86 (1), 189–195. ; discussion 96-97. 10.1016/j.athoracsur.2008.03.073 18573422 PMC 2790810 · doi ↗ · pubmed ↗
- 7Bongarzone S.Savickas V.Luzi F.Gee A. D. (2017). Targeting the receptor for advanced glycation endproducts (rage): a medicinal chemistry perspective. J. Med. Chem. 60 (17), 7213–7232. 10.1021/acs.jmedchem.7b 00058 28482155 PMC 5601361 · doi ↗ · pubmed ↗
- 8Bruhm D. C.Vulpescu N. A.Foda Z. H.Phallen J.Scharpf R. B.Velculescu V. E. (2025). Genomic and fragmentomic landscapes of cell-free DNA for early cancer detection. Nat. Rev. Cancer 25, 341–358. 10.1038/s 41568-025-00795-x 40038442 PMC 13003562 · doi ↗ · pubmed ↗