Multimodality imaging of ischaemia with non-obstructive coronary artery disease in a patient with coronary artery ectasia: a case report
Masatoki Nakaza, Yukihiro Watanabe, Keishi Suzuki, Akira Shibata, Masashi Ogawa, Tetsuro Sekine

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
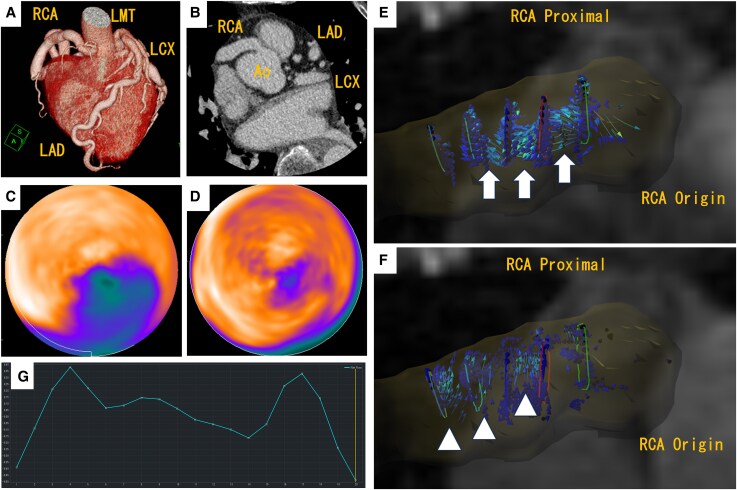 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKawasaki Disease and Coronary Complications · Coronary Artery Anomalies · Cardiac Imaging and Diagnostics
A 76-year-old woman was hospitalized for heart failure. Echocardiography demonstrated a preserved left ventricular ejection fraction of 62%, but wall motion abnormalities were detected in the inferior wall. Coronary computed tomography angiography showed coronary artery ectasia (CAE) in three arteries without significant stenosis (Figure 1A and B). 13N-ammonia positron emission tomography imaging revealed rest perfusion defect with larger stress perfusion defect in the inferior and inferoposterior wall, which indicates myocardial infarction with concomitant myocardial ischaemia (Figure 1C: polar map stress and D: polar map rest). The myocardial blood flow reserve in each of the three arterial territories decreased, particularly in the right coronary artery (RCA) territory at 1.43. Four-dimensional flow coronary magnetic resonance imaging revealed slow and turbulent flow in the proximal RCA [Figure 1E and F: forward flow (white arrow) and backward flow (white arrowhead)]. Coronary flow volume (time-averaged flow volume) in the RCA was 0.15 mL/s in one cardiac cycle (Figure 1G: coronary flow velocity waveform).^1^ A similar, albeit less pronounced, flow pattern was observed in the left main trunk (measured value, 0.38 mL/s).
Coronary artery ectasia is defined as a diffuse or focal dilatation of the epicardial coronary artery and has gained increasing recognition for its association with non-obstructive coronary artery disease;^2^ however, its underlying pathophysiology remains poorly understood. This case demonstrated pronounced epicardial coronary flow disturbances in the RCA accompanied by myocardial ischaemia and coronary microvascular dysfunction in the perfusion territory. These findings highlight the key role of the combination of epicardial flow disturbances and microvascular dysfunction in the pathogenesis of myocardial ischaemia in patients with CAE.^3^
We used a SIGNA Architect 3.0T MRI system (GE Healthcare) and GTFlow software (GyroTools) for 4D flow MRI analysis. The detailed scan parameters were as follows: repetition time/echo time = 4.0/2.7 ms; flip angle = 13°; voxel size = 1.3 × 1.3 × 2.0 mm³; temporal resolution = 83 ms; velocity encoding = 50 cm/s; 20 cardiac phases; HyperKat acceleration (acceleration factor = 8); and navigator-based respiratory gating with a respiratory compensation acceptance ratio of 25%.
Consent: Written informed consent was obtained from the patient for the publication of this case report and the accompanying images.
Funding: None declared.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Blanken CPS, Schrauben EM, Peper ES, Gottwald LM, Coolen BF, van Wijk DF, et al Coronary flow assessment using accelerated 4D flow MRI with respiratory motion correction. Front Bioeng Biotechnol 2021;9:725833.34869250 10.3389/fbioe.2021.725833 PMC 8634777 · doi ↗ · pubmed ↗
- 2Eyuboglu M, Eyuboglu C. Coronary artery ectasia in the pathophysiology of myocardial infarction with nonobstructive coronary arteries. Am J Cardiol 2022;171:28–31.35287947 10.1016/j.amjcard.2022.01.043 · doi ↗ · pubmed ↗
- 3Akyürek O, Berkalp B, Sayin T, Kumbasar D, Kervancioğlu C, Oral D. Altered coronary flow properties in diffuse coronary artery ectasia. Am Heart J 2003;145:66–72.12514656 10.1067/mhj.2003.48 · doi ↗ · pubmed ↗