Electroconvulsive therapy use in New South Wales between 1944 and 1949
Brian Draper, Chanaka Wijeratne

TL;DR
This study examines the use of electroconvulsive therapy in New South Wales from 1944 to 1949, revealing broader clinical applications and consistent gender and mortality patterns.
Contribution
The paper provides historical insight into ECT usage and clinical indications in mid-20th century NSW.
Findings
ECT was used for non-affective and affective psychoses as well as confusional states and non-psychotic disorders.
Better outcomes were observed for depression, anxiety, and confusional states compared to non-affective psychoses.
Mortality remained under 1% and the female-to-male ratio for ECT recipients stayed consistent.
Abstract
To identify clinical and other factors associated with the use of electroconvulsive therapy (ECT) in New South Wales for the period 1944–1949 and to compare with contemporaneous practice. Annual reports of the Inspector-General of Mental Hospitals in NSW (1944/45 to 1948/49) were examined. Seven hospitals reported a total of 8964 courses of treatment during the period. Demographically, 60.6% of patients who received ECT were female, and rural hospitals reported 13.6% of courses. ECT was as likely to be given for non-affective psychoses (37.7%), as for affective psychoses (35.0%). ECT was also administered for confusional states and non-psychotic disorders. Better outcomes were observed for depression, anxiety and confusional states than non-affective psychoses. Recovery rates declined over the study period. Mortality was <1%. The clinical indications for ECT in the mid-twentieth…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
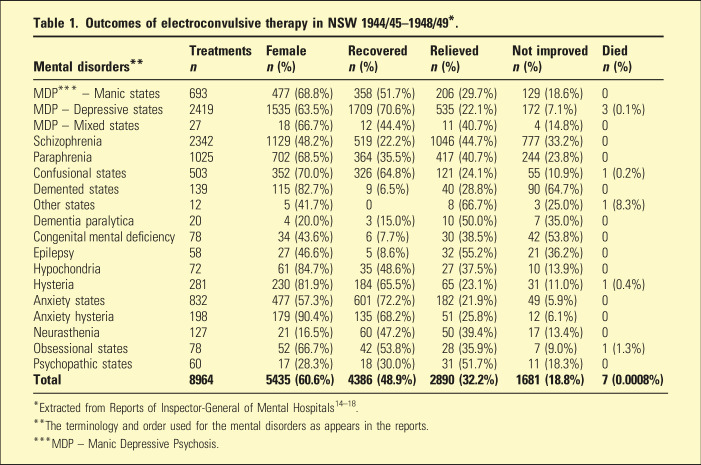 Figure 1
Figure 1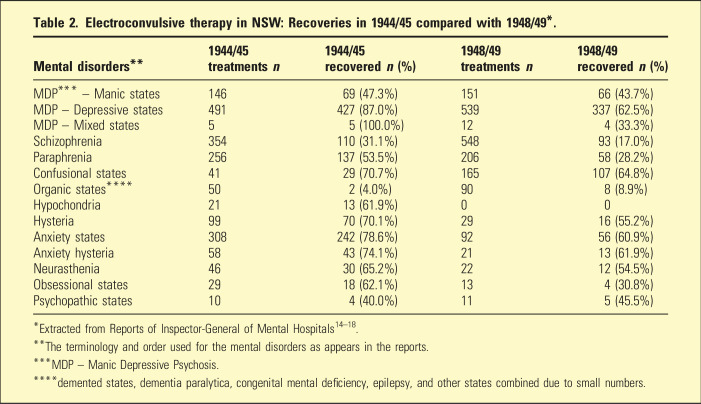 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsElectroconvulsive Therapy Studies · Historical Psychiatry and Medical Practices · Neurology and Historical Studies
Although the origins of electroconvulsive therapy (ECT) can be traced back to the eighteenth century,^ 1 ^ it was the work of Cerletti and Bini in Italy in April 1938 that heralded modern ECT.^ 2 ^ This occurred in the context of there being no effective psychotropic drugs, with alternative treatments for severe psychoses being insulin coma therapy, pentamethylenetetrazol (Cardiazol) convulsion therapy, or psychosurgery, each of which had significant adverse effects.^ 2 ^ Ladislaus von Meduna, who pioneered intravenous Cardiazol convulsion therapy to treat schizophrenia in 1934, had initially used intramuscular camphor which he abandoned due to its inconsistent composition and speed of action.^ 3 ^ By 1940, ECT was being used to treat a wide range of severe mental disorders in North America and Europe,^ 2 ^ sometimes with remarkable results as noted in newspaper reports.^ 4 ^ ECT was regarded as being particularly effective in the treatment of psychoses and during the 1940s this was further narrowed to the affective psychoses, although it was also used more controversially in a range of other conditions including neuroses, personality disorders and anorexia nervosa.^5?–7^
Insulin and Cardiazol were introduced in New South Wales (NSW) in 1937–38 for the treatment of schizophrenia. The NSW Inspector-General of Mental Hospitals noted in his annual report in 1939 that insulin treatment was limited by the need for additional staff and Cardiazol was showing promising results.^ 8 ^ Indeed, Dr S Evan Jones examined the results of Cardiazol therapy for the period 1937 to 1941 and found that 61% of manic depressive states and 29% of schizophrenia cases recovered.^ 9 ^ By 1940 stocks of Cardiazol in NSW were exhausted, and although Phrenazol was being used in its place with good results in schizophrenia and other psychoses, this proved the precipitant to NSW procuring two ECT machines to replace or partially replace Cardiazol.^ 10 ^
The first ECT machine in Australia was built by Dr Hugh Birch at Parkside Hospital, Adelaide in 1941.^ 11 ^ In NSW, the first ECT machines were imported from England in July 1942 and used at Callan Park Hospital, with early success reported in the newspapers in October 1942.^12,13^ Australian research into the use of ECT first appeared in 1948 when Bostock and Phillips from Brisbane published an overview of the use of ECT in the Medical Journal of Australia, including the outcomes of the treatment of 100 cases of anxiety and depression from the Brisbane General Hospital.^ 14 ^ There is no other published Australian research that examined ECT use and its outcomes in the 1940s.
In this study, the statewide use of ECT in NSW in the period 1944–1949 is examined from information published in the annual reports of the Inspector-General of Mental Hospitals in NSW. The aims are to describe the mental disorders for which ECT was used in this period, the treatment outcomes obtained for each disorder, sex differences in the use of ECT, and whether the use of ECT, and the outcomes obtained, changed over the period of the study and compared with contemporary practice.
Methods
The Inspector-General of Mental Hospitals in NSW, under the requirements of the Lunacy and Inebriates Act 1937, presented an Annual Report to the NSW Parliament with details of the provision of mental health services in NSW. The reports are available in the State Library of NSW. Between 1945 and 1949, these reports included tables with non-identifiable details of the provision of ECT in the previous financial year, including the hospitals where it was used, the mental disorders it was used for, the sex of the patient and the treatment outcomes. There was no information about patient age, the number of ECT treatments administered in a course, the specific characteristics of ECT, the manner in which consent was obtained, or socio-economic factors.^15???–19^
Patient sex, the frequency and outcomes of treatment (recovered, relieved, not improved, died) of ECT use in each mental disorder were determined. Comparison of treatment effectiveness was calculated by the proportions in each outcome category for each disorder. Comparison of the use of ECT in each hospital was made regarding the types of mental disorders treated. Treatment use and outcomes over time were examined.
Ethical approval was obtained from the University of NSW Human Research Ethics Committee (iRECS7225).
Results
In the five financial years covered in these reports, there were seven hospitals reporting their use of ECT – Broughton Hall (5 years), Orange (5 years), Callan Park (4 years), Gladesville (4 years), Morisset (4 years), Parramatta (4 years), and Kenmore (2 years). Most of the treatment courses were undertaken at Broughton Hall (n = 4590, 51.2%), followed by Callan Park (n = 1214, 13.5%), Gladesville (n = 1152, 12.9%), Parramatta (n = 806, 9.0%), Morisset (n = 690, 7.7%), Orange (n = 357, 4.0%) and Kenmore (n = 167, 1.9%). The combined data for the five financial years is presented in Table 1. ECT was as likely to be given for non-affective psychoses (schizophrenia and paraphrenia) (37.7%) as for affective psychoses (manic depressive psychosis – depression, mania and mixed) (35.0%).Table 1.Outcomes of electroconvulsive therapy in NSW 1944/45–1948/49*.Mental disordersTreatments nFemale n (%)Recovered n (%)Relieved n (%)Not improved n (%)Died n (%)MDP* – Manic states693477 (68.8%)358 (51.7%)206 (29.7%)129 (18.6%)0MDP – Depressive states24191535 (63.5%)1709 (70.6%)535 (22.1%)172 (7.1%)3 (0.1%)MDP – Mixed states2718 (66.7%)12 (44.4%)11 (40.7%)4 (14.8%)0Schizophrenia23421129 (48.2%)519 (22.2%)1046 (44.7%)777 (33.2%)0Paraphrenia1025702 (68.5%)364 (35.5%)417 (40.7%)244 (23.8%)0Confusional states503352 (70.0%)326 (64.8%)121 (24.1%)55 (10.9%)1 (0.2%)Demented states139115 (82.7%)9 (6.5%)40 (28.8%)90 (64.7%)0Other states125 (41.7%)08 (66.7%)3 (25.0%)1 (8.3%)Dementia paralytica204 (20.0%)3 (15.0%)10 (50.0%)7 (35.0%)0Congenital mental deficiency7834 (43.6%)6 (7.7%)30 (38.5%)42 (53.8%)0Epilepsy5827 (46.6%)5 (8.6%)32 (55.2%)21 (36.2%)0Hypochondria7261 (84.7%)35 (48.6%)27 (37.5%)10 (13.9%)0Hysteria281230 (81.9%)184 (65.5%)65 (23.1%)31 (11.0%)1 (0.4%)Anxiety states832477 (57.3%)601 (72.2%)182 (21.9%)49 (5.9%)0Anxiety hysteria198179 (90.4%)135 (68.2%)51 (25.8%)12 (6.1%)0Neurasthenia12721 (16.5%)60 (47.2%)50 (39.4%)17 (13.4%)0Obsessional states7852 (66.7%)42 (53.8%)28 (35.9%)7 (9.0%)1 (1.3%)Psychopathic states6017 (28.3%)18 (30.0%)31 (51.7%)11 (18.3%)0 Total
8964
5435 (60.6%)
4386 (48.9%)
2890 (32.2%)
1681 (18.8%)
7 (0.0008%) *Extracted from Reports of Inspector-General of Mental Hospitals^14???–18^.**The terminology and order used for the mental disorders as appears in the reports.***MDP – Manic Depressive Psychosis.
The use of ECT in some types of mental disorders mainly occurred at Broughton Hall – anxiety hysteria (100%), hypochondria (100%), hysteria (99.6%), anxiety states (98.3%), neurasthenia (97.6%), psychopathic states (91.7%) and epilepsy (60.3%). There were no consistent patterns of change over time in the use of ECT across the hospitals for various mental disorders. For example, the use of ECT for schizophrenia declined at Broughton Hall, Morisset and Parramatta, while it increased at Orange, Callan Park and Gladesville. In their first year of ECT use, Kenmore (37 courses) and Orange (27 courses) gave ECT for demented states with poor outcomes, then much less in later years. In contrast Gladesville had no initial use of ECT for demented states, but by 1948/49 gave 20 courses.
The outcomes of ECT declined over time. Combining all diagnostic groups, 1195 (59.2%) recovered and 425 (21.1%) were relieved in 1944/45, while 651 (34.3%) recovered and 884 (46.6%) were relieved in 1948/49. There was no change in the proportion that did not improve which was 19% in both years and the number of deaths did not change. Recoveries in specific mental disorders are presented in Table 2. At Gladesville Hospital in 1948/49 it was noted that 152 patients (49.8%) had previous courses of ECT, the only information available on this issue.Table 2.Electroconvulsive therapy in NSW: Recoveries in 1944/45 compared with 1948/49*.Mental disorders1944/45 treatments n1944/45 recovered n (%)1948/49 treatments n1948/49 recovered n (%)MDP* – Manic states14669 (47.3%)15166 (43.7%)MDP – Depressive states491427 (87.0%)539337 (62.5%)MDP – Mixed states55 (100.0%)124 (33.3%)Schizophrenia354110 (31.1%)54893 (17.0%)Paraphrenia256137 (53.5%)20658 (28.2%)Confusional states4129 (70.7%)165107 (64.8%)Organic states****502 (4.0%)908 (8.9%)Hypochondria2113 (61.9%)00Hysteria9970 (70.1%)2916 (55.2%)Anxiety states308242 (78.6%)9256 (60.9%)Anxiety hysteria5843 (74.1%)2113 (61.9%)Neurasthenia4630 (65.2%)2212 (54.5%)Obsessional states2918 (62.1%)134 (30.8%)Psychopathic states104 (40.0%)115 (45.5%)*Extracted from Reports of Inspector-General of Mental Hospitals^14???–18^.**The terminology and order used for the mental disorders as appears in the reports.***MDP – Manic Depressive Psychosis.****demented states, dementia paralytica, congenital mental deficiency, epilepsy, and other states combined due to small numbers.
Discussion
The main finding of this study is that the clinical indications for the early use of ECT in NSW differed from contemporary practice in NSW 2013 to 2022. Although in both eras ECT was most frequently prescribed for depression, in the 1940s a higher proportion of cases had non-affective psychoses (paraphrenia/schizophrenia – 37.6%) compared with contemporary practice (schizophrenia, schizoaffective and schizophrenia-related disorders – 24.7%), perhaps not surprising at a time when there were no antipsychotic drugs.^ 20 ^ In contrast, the sex ratio was almost identical to contemporary practice,^ 20 ^ as was the mortality rate,^ 21 ^ although it is unclear for what time period after ECT mortality was reported.
The effective use of ECT in anxiety states and other non-psychotic disorders, which might seem unusual to current practitioners, had an evidence base in the 1940s–50s, with good results being reported, including from Australia.^7,14,22^ This was an era where the main treatment for these disorders was psychodynamic psychotherapy, a treatment modality unsuitable for some patients and not accessible for many. It is noteworthy that nearly all the ECT for these conditions was given at Broughton Hall, a hospital predominantly for voluntary patients, and thus with a different patient population to the other mental hospitals.
Nevertheless, psychiatric diagnoses were marred by a lack of reliability and standardisation in the mid-twentieth century. It is possible that some patients with non-melancholic, non-psychotic depressive disorder or agitated depression were misdiagnosed with anxiety states such as hysteria and neurasthenia, which may explain the high response rate for anxiety disorders. ECT remains an indication for non-psychotic depressive disorder.^ 23 ^ In addition, having a ‘manic depressive psychosis’ diagnosis did not mean that the patient was psychotic during the episode. Another possibility is that ECT was used for ‘diagnostic-curative purposes’, especially to differentiate between psychogenic and organic disorders in presentations of pain or seizures, and the belief that some patients concealed psychotic symptoms that would be uncovered by ECT, like with the use of pentothal.^ 14 ^
That 64.8% of patients with confusional states were reported as having recovered after ECT is surprising given the lack of evidence supporting the efficacy of ECT for delirium.^ 24 ^ The most likely reason is that patients with mood or psychotic disorders and altered consciousness or disorientation were described as ‘confused’, which in older patients might be due to a comorbid cognitive disorder. Delirious mania is another example of a diagnostic category with such mixed features.^ 25 ^
The use of ECT in other organic disorders including dementia had, not unexpectedly, poor outcomes. While the data does not indicate the reason ECT was used, it is likely that it was used to treat behavioural or psychotic features of these disorders, as was reported for treating severe depression and agitation in dementia paralytica in 1953 and more recently in severe behavioural disturbances in people with dementia.^26,27^
Better outcomes occurred in the affective than non-affective psychoses, as had been reported in studies from the United States in 1945 and 1948.^22,28^ While there was no information about relapse rates, that around half of the patients receiving ECT at Gladesville Hospital in 1948/49 had previous courses of ECT suggests that over time recovery was not sustained. In addition, the reduced effectiveness of ECT in 1948/49 compared with 1944/45 is consistent with a higher proportion of treatments being given to relapses.
Although the proportion of patients who received ECT in each of the seven hospitals is unknown, the marked variation in the number of treatment courses is noteworthy. More than half of all courses were administered in Broughton Hall, a voluntary admission clinic which may have attracted more people of higher socio-economic status, a non-clinical predictor of access to ECT in the current day.^ 20 ^
The three hospitals which were least likely to report ECT were the only hospitals outside of Sydney, collectively accounting for 13.6% of all courses, although the Commonwealth Census of 1947 reported 28% of the NSW population was rural dwelling.^ 29 ^ Whilst this does suggest a geographical disadvantage for receiving ECT, it may simply have reflected the slower spread of information about a new treatment in that era.
Finally, whilst there is no information about the manner in which treatment was administered in NSW in the 1940s, it would be expected to have been similar to that used in Queensland in the same period.^ 14 ^ Apprehensive or restless patients were given a mixture of potassium bromide, chloral hydrate and paraldehyde for sedation during treatment; others received paraldehyde immediately before treatment to minimise post-ictal agitation. In the absence of muscle relaxants, a wardsman firmly pressed down on the patient’s shoulders, one nurse held down the arms and another the jaw to ensure the mouthguard remained stable. For most patients, electrode placement was over the frontal areas and the electrical dose delivered was 140 V over 0.3 seconds. Whilst subsequent research on the use of bilateral electrode placements using ultra-brief pulse-width has been limited, current ECT guidelines have warned that such treatment is of relatively low efficacy.^ 30 ^
Some limitations to this study include the lack of information regarding patient age, the number of treatments received in each course, the way ECT was administered, and how many had a previous ECT course.
In conclusion, this study documents the early use of ECT in NSW, the broader range of mental conditions for which it was prescribed compared with contemporary practice, the declining effectiveness of treatments over the 5-year period, and that better outcomes were obtained for affective than non-affective psychoses.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Harms E . The origin and early history of electrotherapy and electroshock. Am J Psychiatr 1955; 111: 932–933.14376664 · pubmed ↗
- 2Lebensohn ZM . The history of electroconvulsive therapy in the United States and its place in American psychiatry: a personal memoir. Compr Psychiatr 1999; 40: 173–181.10.1016/s 0010-440x(99)90000-710360611 · doi ↗ · pubmed ↗
- 3Mccrae N . A violent thunderstorm’: Cardiazol treatment in British mental hospitals. Hist Psychiatr 2006; 17: 67–90.10.1177/0957154 X 0606172317153475 · doi ↗ · pubmed ↗
- 4Anonymous (1942) Mental patients cured by shock. February 2. Newcastle: Newcastle Sun, p 2-P 2.
- 5Androp S . Electric shock therapy in the psychoses: convulsive and subconvulsive methods. Psychiatr Q 1941; 15: 730–749.
- 6Alexander GH . Electroconvulsive Therapy: a five year study of results. J Nerv Ment Dis 1953; 117: 244–250.13070038 · pubmed ↗
- 7Gallinek A . Controversial indications for electric convulsive therapy. Am J Psychiatr 1952; 109: 261–266.12985995 · pubmed ↗
- 8Inspector-General of Mental Hospitals . Report of the inspector-general of mental hospitals New South Wales for the year ended 30th june 1938. Legislative assembly NSW 1939. Sydney NSW: Thomas Henry Tennant, Acting Government Printer.