Left bundle branch area pacing in a case of Steinert’s disease
José M. Sánchez-Moreno, Laura Valverde Soria, Rosa Macías Ruiz, Luis Tercedor, Juan Jiménez-Jáimez, Manuel Molina-Lerma

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
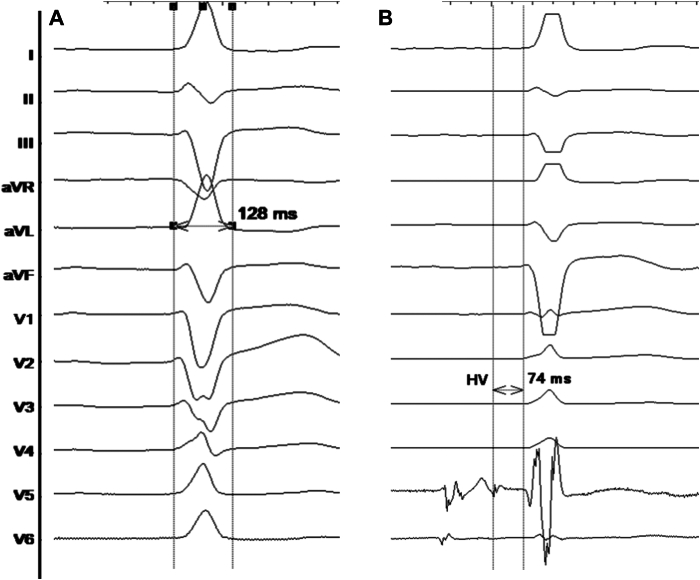 Figure 1
Figure 1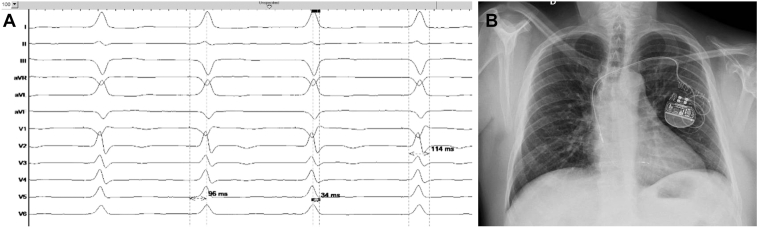 Figure 2
Figure 2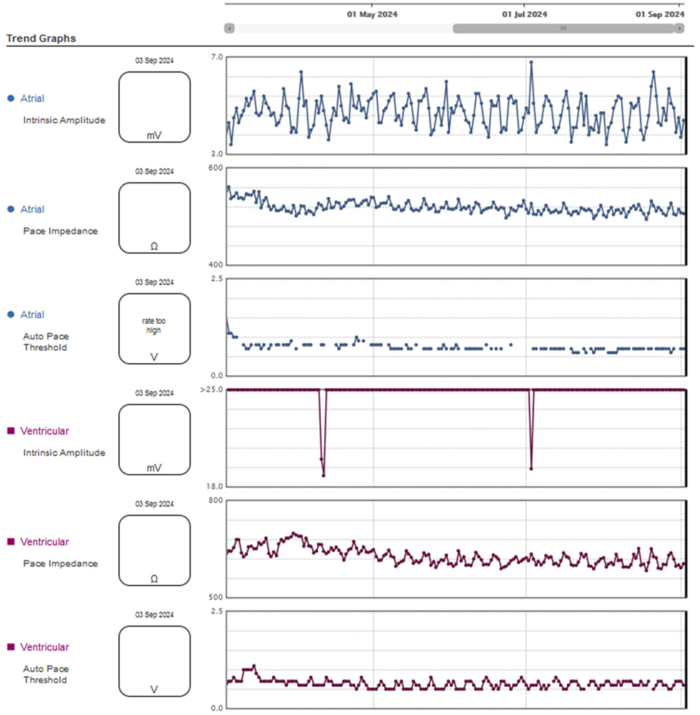 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenetic Neurodegenerative Diseases · Mitochondrial Function and Pathology · Advanced MRI Techniques and Applications
Key Teaching Points
- •Myotonic dystrophy type 1 often presents with cardiomyopathy and conduction disease, especially impairment in the His-Purkinje system.
- •In patients with neuromuscular diseases, such as myotonic dystrophy type 1 and any second- or third-degree atrioventricular block, with or without symptoms, permanent pacing is indicated.
- •Left bundle branch area pacing could be a feasible and more physiological pacing alternative in patients with Steinert’s disease.
Introduction
Myotonic dystrophy type 1 (DM1), or Steinert’s disease, is a neuromuscular myotonic disorder involving the endocrine system, central nervous system, eyes, gastrointestinal system, and heart, and is associated with the presence of abnormal expansion of a cytosine-thymine-guanine trinucleotide repeat on chromosome 19q13.3.1 DM1 often presents with cardiomyopathy and conduction disease, especially impairment in the His-Purkinje system.2
Permanent pacing is indicated in patients with neuromuscular diseases, such as DM1, and any second- or third-degree atrioventricular block, with or without symptoms. In asymptomatic cases with HV interval >70 ms, a pacemaker implantation may be recommended in spite of the lack of evidence.3 Conduction system pacing (CSP), including His bundle pacing (HBP) and left bundle branch area pacing (LBBAP), which encompasses left bundle branch pacing, left fascicular pacing, and left ventricular septal pacing,4 has been accepted as a feasible and safe pacing strategy for those requiring antibradycardia treatment,5 even in the case of infra-Hisian block, demonstrating significantly reduced adverse clinical outcomes.6
There is increasing interest in physiological pacing techniques that directly activate the specialized conduction system. With LBBAP, the lead is implanted slightly distal to the His bundle and is screwed deep in the interventricular septum, ideally to capture the left bundle branch.
Case report
A 50-year-old man with DM1, first-degree atrioventricular block and left bundle branch block, which did not fulfill the Strauss criteria,7 with QRS duration of 128 ms (Figure 1A) was referred for electrophysiological study. He had no history of syncope, palpitations, or documented arrhythmias. Transthoracic echocardiography showed normal biventricular ejection fraction without any pathologic findings. A pathologic HV interval of 74 ms was observed (Figure 1B). Therefore, pacemaker implantation was indicated.Figure 1A: Basal QRS complex with left bundle branch block morphology (duration 128 ms). B: HV interval measured (74 ms) in the electrophysiological study.
Following local anesthesia, double left axillary vein puncture was performed. A SelectSecure™ MRI SureScan™ Model 3830 pacing lead (Medtronic, Minneapolis, MN) was inserted with the support of a preshaped catheter (model C315HIS, Medtronic) in the left ventricle septum, achieving nonselective left bundle branch pacing (left ventricular activation time of 96 ms and interpeak interval of 34 ms). Pacing threshold, impedance, and mean R-wave amplitude were 0.8 V at 0.4 ms, 934 Ω, and >25 mV, respectively. Afterwards, the atrial lead was placed into the right atrial appendage. Electrocardiography showed a paced QRS duration of 114 ms with unipolar pacing (Figure 2A). DDD mode was programmed. No periprocedural complications were observed and chest radiograph showed adequate lead position with no signs of acute pneumothorax (Figure 2B). At follow-up visits, the patient remained asymptomatic, ejection fraction was preserved, and pacemaker parameters remained stable (Figure 3).Figure 2A: Paced QRS complex after nonselective left bundle branch pacing with a left ventricular activation time of 96 ms and an interpeak interval of 34 ms. B: Anteroposterior radiograph chest view demonstrating the lead position in the basal septum.Figure 3. Remote monitoring after 6-month follow-up.
Discussion
It is widely accepted that conduction disease observed in patients with DM1 is commonly due to impairment in the His-Purkinje system. However, its pathogenesis is not clear. Although histologic studies of the heart in DM1 are scarce, common findings are interstitial fibrosis and fatty infiltration of the myocardium.8 A possible concern regarding CSP feasibility in these patients might be the risk of inefficient pacing because of severe conduction disease distal to the stimulation point. Nonetheless, previous published studies suggest otherwise since the target in LBBAP is more distal and broader than that in HBP.9 It has been demonstrated that HBP and LBBAP can effectively improve cardiac function by successfully correcting left bundle branch block in patients with heart failure.10 Postulated mechanism for these findings are source-sink mismatch, where an increase in source power can facilitate depolarization of distal tissue, and virtual electrode polarization, where an electrical stimulus generates regions of depolarization or hyperpolarization around the electrode tip, which in turn creates potential pathways for propagation through excitation of previously refractory tissue.11
Our experience with LBBAP in a patient with DM1 does not differ when using this approach in patients with left bundle branch block related to other conditions. In a recent systematic review and meta-analysis,12 patients with indications for cardiac resynchronization therapy followed up for 6–27 months presented better clinical and functional outcomes with CSP than conventional biventricular pacing. Hence, LBBAP could also be a feasible and more physiological pacing alternative for patients with DM1. However, long-term follow-up is needed to ensure its safety and durability because progressive degeneration of conduction system disease is described in DM1. To our knowledge, this is the first published case of LBBAP in a patient with DM1, and more evidence is needed to clarify the best pacing strategy for this subgroup of patients.
Disclosures
The authors have no conflicts of interest to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pelargonio G.Dello Russo A.Sanna T.De Martino G.Bellocci F.Myotonic dystrophy and the heart Heart 8820026656701243391310.1136/heart.88.6.665PMC 1767476 · doi ↗ · pubmed ↗
- 2Arbustini E.Di Toro A.Giuliani L.Favalli V.Narula N.Grasso M.Cardiac phenotypes in hereditary muscle disorders: JACC state-of-the-art review J Am Coll Cardiol 7220182485250610.1016/j.jacc.2018.08.218230442292 · doi ↗ · pubmed ↗
- 3Glikson M.Nielsen J.C.Kronborg M.B.2021 ESC guidelines on cardiac pacing and cardiac resynchronization therapy Eur Heart J 422021342735203445543010.1093/eurheartj/ehab 364 · doi ↗ · pubmed ↗
- 4Burri H.Jastrzebski M.CanoÓ.EHRA clinical consensus statement on conduction system pacing implantation: endorsed by the Asia Pacific Heart Rhythm Society (APHRS), Canadian Heart Rhythm Society (CHRS), and Latin American Heart Rhythm Society (LAHRS)Europace 252023120812363706184810.1093/europace/euad 043PMC 10105878 · doi ↗ · pubmed ↗
- 5Jastrzębski M.Kiełbasa G.Cano O.Left bundle branch area pacing outcomes: the multicentre European MELOS study Eur Heart J 432022416141733597984310.1093/eurheartj/ehac 445PMC 9584750 · doi ↗ · pubmed ↗
- 6Tan E.S.J.Soh R.Lee J.Y.Clinical outcomes in conduction system pacing compared to right ventricular pacing in bradycardia JACC Clin Electrophysiol 9202399210013675245310.1016/j.jacep.2022.10.016 · doi ↗ · pubmed ↗
- 7Strauss D.G.Selvester R.H.Wagner G.S.Defining left bundle branch block in the era of cardiac resynchronization therapy Am J Cardiol 10720119279342137693010.1016/j.amjcard.2010.11.010 · doi ↗ · pubmed ↗
- 8Mahadevan M.S.Yadava R.S.Mandal M.Cardiac pathology in myotonic dystrophy type 1Int J Mol Sci 2220211187410.3390/ijms 222111874 PMC 858435234769305 · doi ↗ · pubmed ↗