Daratumumab for PRCA after HCT: study and practical considerations from the EBMT Transplant Complications Working Party
Nico Gagelmann, Moniek de Witte, Christophe Peczynski, William Boreland, Annoek E. C. Broers, Edgar Jost, Alexander Kulagin, Albert Esquirol, Simona Sica, Jürgen Kuball, Gerardo Errico, Wolfgang Bethge, Johan Maertens, Friedrich Stölzel, Edouard Forcade, Matthew Collin

TL;DR
This study shows that daratumumab can effectively treat PRCA after blood stem cell transplants, with high response rates and survival, though it requires careful monitoring for side effects.
Contribution
The first international and largest study on daratumumab for PRCA after allogeneic HCT, showing superior response rates compared to other treatments.
Findings
69% of patients achieved transfusion independence at 6 months, increasing to 80% at 12 months.
Hemoglobin and reticulocyte recovery rates were 56% and 78% at 6 months, and 65% and 83% at 12 months.
12-month survival was 81%, with most deaths linked to GVHD or infections.
Abstract
Pure red cell aplasia (PRCA) is a relevant complication after ABO-mismatched allogeneic hematopoietic cell transplantation (HCT). No standard treatment exists, and practice is heterogenous. In this study, we took advantage of an international collaboration to describe characteristics and outcomes of patients receiving daratumumab for PRCA following first allogeneic HCT. We identified 45 patients meeting these criteria (median patient age, 56 years). The median time from HCT to PRCA was 55 days (IQR, 36–116) and all patients were transfusion-dependent at time of daratumumab start. Daratumumab was first-line treatment in 16 patients (36%), most patients (67%) received daratumumab intravenously, and median time from PRCA diagnosis and daratumumab start was 88 days (IQR, 59–219). Incidence of transfusion independence was 69% (95% confidence interval [CI], 52–80%) at 6 months and 80% (95%…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
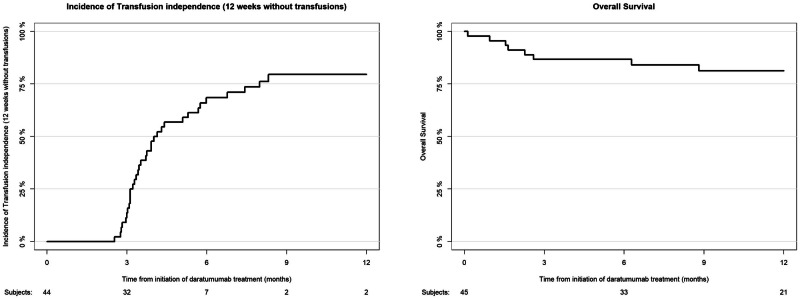 Figure 1
Figure 1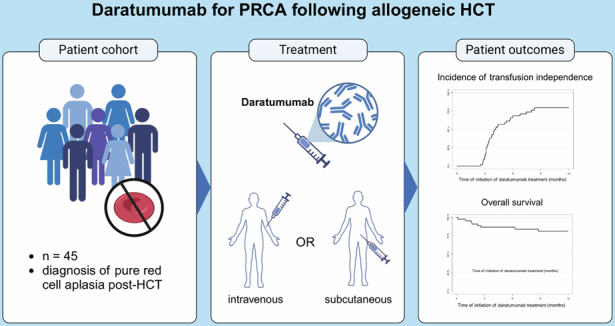 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHematopoietic Stem Cell Transplantation · Chronic Lymphocytic Leukemia Research · Immunodeficiency and Autoimmune Disorders
Introduction
Pure red cell aplasia (PRCA) is a rare but severe complication that can occur following ABO-mismatched allogeneic hematopoietic cell transplantation (HCT) [1]. It is characterized by a selective failure of erythroid progenitors, leading to severe anemia in affected patients [2]. PRCA post-HCT poses significant clinical challenges, often resulting in prolonged dependence on blood transfusions and a reduced quality of life. Despite various therapeutic strategies, including immunosuppressive therapy and donor lymphocyte infusions [3, 4], treatment responses have been inconsistent, highlighting the need for innovative and targeted interventions [5].
Daratumumab, a human anti-CD38 monoclonal antibody, has emerged as a promising therapeutic option in hematologic disorders due to its potent immunomodulatory effects [6]. Initially approved for multiple myeloma, daratumumab has demonstrated the ability to target CD38-expressing plasma cells and immune regulatory cells, leading to the depletion of pathogenic cell populations. Growing evidence, mainly consisting of single cases or small cohorts, suggests that daratumumab may offer clinical benefit in PRCA cases that are refractory to conventional therapies, given its mechanism of targeting and depleting CD38-positive cells that may contribute to the pathogenesis of PRCA [7–12].
This study aimed to explore the characteristics, efficacy, and safety of daratumumab in the management of PRCA following allogeneic HCT, using data from the first and largest international cohort of patients receiving daratumumab in this setting. Finally, we performed a comprehensive literature review to identify all current evidence and positioned our results within the spectrum of currently published literature to give practical considerations concerning the role of daratumumab as novel treatment option for PRCA following allogeneic HCT.
Methods
Data collection
The data collection process involved several key steps to ensure the integrity, accuracy, and completeness of the dataset. This study used registry data from the European Society for Blood and Marrow Transplantation (EBMT), serving as a comprehensive repository for collecting and analyzing patient, disease, and transplant-related data across Europe and other collaborating regions. First, we utilized the EBMT network to identify centers that treated patients with daratumumab for post-allogeneic HCT PRCA. Next, we gathered relevant clinical and demographic as well as treatment-specific information on patients diagnosed with PRCA following allogeneic HCT and treated with daratumumab in a real-world setting.
The study adhered to the ethical guidelines established by the EBMT and local regulatory bodies and is in accordance with the Declaration of Helsinki. Informed consent had been obtained from all patients as part of their registration in the EBMT database, in accordance with the organization’s ethical standards.
Patient selection and inclusion criteria
An invitation was sent to all of EBMT member centres regularly performing adult allogeneic HCTs in order for them to identify eligible patients, as data on PRCA presence was not routinely collected in the registry. The study has been approved by the local ethics committees and patients gave their consent in accordance with EBMT standard practice. This study is in accordance with the Declaration of Helsinki.
The inclusion criteria comprised adult patients who had undergone first allogeneic HCT and were subsequently diagnosed with PRCA, as defined by standard clinical and laboratory criteria [2]. The selection also required patients to have received daratumumab as part of their therapeutic regimen to address PRCA. Treatment with daratumumab in any line of treatment was accepted. Patients with incomplete records or those with other causes of anemia unrelated to PRCA were excluded from the analysis.
The following variables were collected from the 22 EBMT member centres, who accepted to participate, for each of their eligible patients:
- Demographic information: age (patient and donor), gender (patient and donor), ABO mismatch, rhesus factor (patient and donor) and underlying disease for which HCT was performed.
- Transplant-related data: pre-existing comorbidities, conditioning regimen, disease status at HCT, donor type, cell source, performance status at HCT, CMV status (patient and donor), GvHD prophylaxis, previous autologous transplantation, ex-vivo T-cell depletion and history of graft-versus-host disease (GVHD).
- Therapeutic interventions: previous treatments administered for PRCA, schedule and number of infusions of daratumumab, dosage and route of administration, and concurrent therapies.
- Clinical outcomes: hemoglobin levels and reticulocyte counts pre- and post-treatment, transfusion dependency, adverse events, and patient survival rates.
Study endpoints and statistical analysis
First, we aimed to describe the cohort of patients receiving daratumumab for PRCA, to understand current practices and heterogeneity. Next, we evaluated the outcomes after receiving daratumumab, with particular focus on the main clinical endpoint of transfusion independence (defined as 12 weeks without the need for transfusions). Further endpoints were hemoglobin recovery, reticulocyte recovery, overall survival (OS), and causes of death. OS was defined as time from date of first infusion of daratumumab to latest follow-up or death from any cause.
Probabilities of OS were calculated using the Kaplan–Meier method. Cumulative incidences were used to estimate the endpoints of transfusion independence, hemoglobin recovery and reticulocyte recovery to accommodate for competing risks. Follow-up values were estimated using the reverse Kaplan–Meier method. Statistical analyses were done with R statistical software version 4.1.2.
Practical considerations
Practical considerations were identified and developed through a consensus process involving a panel of experts with clinical experience in HCT and use of daratumumab for PRCA. Discussions were informed by clinical experience, study and case data, prevailing practice patterns, and interpretation of available but limited data, recognizing that high-quality evidence was lacking in several key areas. The panel acknowledged current challenges and identified areas of unmet clinical need. Through iterative process, position statements and practical considerations were formulated to guide clinical management and provoke future research. Considerations reflected collective expert opinion and professional judgment rather than formal evidence grading.
Results
Patient, donor, and transplant characteristics
This study included a total of 45 patients who received daratumumab for PRCA after allogeneic HCT (Table 1). Most of the patients were transplanted between 2020 and 2022, and the most frequent indication for allogeneic HCT was acute leukemia (44%) and myelodysplastic syndrome or myeloproliferative neoplasm (27%). Five patients (11%) received a previous autologous transplantation. Most patients (91%) received allogeneic HCT using peripheral blood. Donor types were as follows: matched sibling (18%), matched unrelated (10/10) (53%), mismatched unrelated (<10/10) (22%), and haploidentical (7%). Most patients (93%) did not receive ex vivo T-cell depletion during allogeneic HCT.Table 1. Patient, donor, and transplant characteristics.CharacteristicTotal cohort(n = 45)Patient age in years, median (range)56.2 (25.8–75.8)Donor age in years, median (range)33.2 (16.4–76.3)Patient sex Female35 (77.8%) Male10 (22.2%)Patient blood group O39 (86.7%) A4 (8.9%) B2 (4.4%)Donor blood group A27 (61.4%) B11 (25%) AB4 (9.1%) O2 (4.5%) Unknown1Patient Rhesus Present37 (84) Absent7 (16) Unknown1Donor Rhesus Present37 (82) Absent8 (18)Karnofsky score 90–100%31 (74) <9011 (26) Unknown3HCT-CI 017 (40.5%) 1–212 (28.6%) >213 (31%) Unknown3Transplant indication Acute leukemia20 (44.4%) MDS or MPN12 (26.7%) Chronic leukemia4 (8.9%) Bone marrow failure4 (8.9%) Lymphoma3 (6.7%) Autoimmune disease1 (2.2%) Other1 (2.2%)Disease status at transplant Complete remission22 (50) Stable disease (no change, no response)5 (11) Never treated4 (9) Relapse or progression5 (11) Other8 (19) Unknown1Transplant year, median (IQR)2021 (2020–2022)Donor type Matched unrelated (10/10)24 (53.3%) Matched sibling8 (17.8%) Mismatched unrelated (<10/10)10 (22.3%) Haploidentical3 (6.7%)Graft source Peripheral blood41 (91.1%) Bone marrow4 (8.9%)GVHD prophylaxis ATG-based10 (22) PTCY-based17 (38) Other18 (40)Ex vivo T-cell depletion No42 (93.3%) Yes3 (6.7%)Conditioning intensity Myeloablative26 (57.8%) Reduced19 (42.2%)
The median patient age was 56 years, and median donor age was 33 years. The most frequent patient blood group was O (87%), and the most frequent donor blood group was A (61%). Most patients and donors were male (78 and 84%, respectively).
Intensity of pre-allogeneic HCT conditioning was myeloablative in 58% and reduced in 42% of patients. Total-body irradiation was used as part of the conditioning in 18%. The most frequently used conditioning regimen was busulfan-fludarabine (42%) or busulfan-fludarabine-thiotepa (20%). The most frequent GVHD prophylaxis was cyclosporine A and mycophenolate mofetil (16%).
Characteristics of daratumumab for PRCA
The median onset of PRCA diagnosis following HCT was 55 days (interquartile range [IQR], 36–116 days). All patients were transfusion-dependent upon daratumumab start and needed at least weekly transfusions (Table 2). Daratumumab was used as first-line treatment in 16 patients (36%), while the remaining 29 patients (64%) received other treatments prior to daratumumab start. Of those, 26 (90%) received rituximab, 6 (21%) received cyclosporine A, and 10 (34.5%) received steroids for PRCA.Table 2PRCA and daratumumab characteristics.CharacteristicTotal cohort(n = 45)Time between transplant and PRCA in days, median (range)55 (36–116)Treatments for PRCA before daratumumab29 (64.4%)Rituximab26 (89.7%)Steroids10 (34.5%)Cyclosporine A6 (20.7%)Other^a^9 (31.0%)Patient transfusion dependent at daratumumab start45 (100%)Total number of RBC transfusions 8 weeks before daratumumab, median (IQR)8 (6–10.5)Hemoglobin level at daratumumab start in g/dL, median (range)7.4 (2.4–9.5)Ferritin level at daratumumab start in µg/l, median (range)2707 (1025–7883)Unknown15Time between PRCA and daratumumab start in days, median (range)88 (59–219)Route of administration of daratumumab Intravenous30 (66.7%) Subcutaneous15 (33.3%)Number of daratumumab infusions 14 (9.3%) 214 (32.6%) 33 (7%) 45 (11.6%) 51 (2.3%) 612 (27.9%) 84 (9.3%) Unknown2Schedule of infusions of daratumumab 1× per week28 (62.2%) 1× per 2 weeks5 (11.1%) 1× per month3 (6.7%) Only 1 infusion4 (8.9%) Other5 (11.1%)Duration of daratumumab treatment in days, median (IQR)21 (10–39)^a^Bortezomib in 3 patients, plasma exchange in 4 patients, Darbepoietin in 1 patient, Erythropoietin in 1 patient.
The median time between PRCA diagnosis and daratumumab treatment was 88 days (IQR, 59–219 days), and the median duration of daratumumab treatment was 21 days (IQR, 10–39 days). Daratumumab was given intravenously in 30 patients (67%) or subcutaneously in 15 patients (33%). Infusion schedules were as follows: once per week in 28 patients (62%); once every two weeks in five patients (11%); once every four weeks in three patients (7%); and only given once in four patients (9%). Five patients received other schedules: one patient received infusions at day 1 and 10; one patient received infusions at day 1, 8, and 22 given for two cycles; one patient received one cycle of infusions at day 1, 8, and 22; one patient received an infusion once every week or two weeks for 18 infusions; and one patient received two weekly infusions, two every two weeks, and two monthly. The most frequent dosing of daratumumab was 16 mg/kg bodyweight in 37 patients (82%). Four patients received lower doses (two patients with 8 mg/kg, one patient with 12 mg/kg, and one patient with 13 mg/kg, respectively). The remaining four patients received higher doses.
Efficacy of daratumumab for PRCA
The median follow-up after daratumumab treatment was 17.4 months (95% confidence interval [CI], 11.1–27.3 months) for the total cohort of 45 patients. Incidence of transfusion independence, defined as 12 weeks without transfusions, was 69% (95% CI, 52–80%) at 6 months and 80% (95% CI, 62–90%) at 12 months after daratumumab start. Only one patient had documented PRCA relapse at 39 days after start of daratumumab treatment. Incidence of hemoglobin recovery at 12 months was 65% (95% CI, 48–77%). Incidence of reticulocyte recovery at 12 months was 83% (95% CI, 65–93%).
The overall survival was 87% (95% CI, 77–97%) at 6 months and 81% (95% CI, 70–94%) at 12 months after start of daratumumab treatment (Fig. 1). In total, eight deaths occurred, of which one was caused by a relapse of the original disease and the remaining seven were allogeneic HCT-related. Only one patient died from complications by hemolytic anemia, while the remaining patients died from GVHD and/or co-occurring infections with multiorgan failure.Fig. 1. Cumulative incidence of transfusion dependence and overall survival of the total cohort.In 45 patients, median follow-up was 17.4 months. Transfusion independence was 69% at 6 months and 80% at 12 months, with one PRCA relapse. At 12 months, hemoglobin and reticulocyte recovery were 65 and 83%, respectively. Overall survival was 87% at 6 months and 81% at 12 months, with 8 deaths mostly related to HCT complications.
Safety of daratumumab for PRCA
Serious adverse events associated with daratumumab were observed in seven patients. Among the most frequently reported severe adverse events, classified as Grade 3 or higher according to the Common Terminology Criteria for Adverse Events (CTCAE), were various types of infections. These included SARS-CoV-2 pneumonia, pneumocystis pneumonia, cytomegalovirus (CMV) reactivation, and an unspecified infection, each affecting one patient.
Additionally, one patient experienced severe diarrhea, which was identified as an adverse event directly linked to daratumumab administration. Another case involved an anaphylactic shock, a potentially life-threatening allergic reaction, while yet another patient suffered from severe respiratory failure. These incidents highlight the range of serious complications that can occur in association with daratumumab treatment, underscoring the need for close monitoring and proactive management of such adverse effects.
Discussion
This is the first multicenter international cohort study on the use of daratumumab for PRCA following allogeneic HCT, providing valuable insights into the characteristics and use of daratumumab for managing PRCA. Our cohort of 45 patients illustrates the potential clinical efficacy of daratumumab in reducing transfusion dependence, resulting in promising overall survival for this challenging post-transplant complication.
A notable finding is the high rate of transfusion independence achieved among patients following daratumumab treatment. With a 69% incidence of transfusion independence at 6 months and 80% at 12 months post-daratumumab. This treatment has demonstrated robust clinical efficacy in promoting erythroid recovery in patients with PRCA after allogeneic HCT. This is particularly promising, given that all patients were transfusion-dependent before initiating daratumumab, with some requiring daily transfusions. Most studies and case reports reported fast disappearance of iso-hemaglutinnin in almost all patients, with few cases of persistence and PRCA relapse [7, 8, 12–14]. In comparison to currently published results of daratumumab for PRCA, our incidence of transfusion-independence appeared to be lower (80% [at one-year after start of daratumumab] versus 93%). However, follow-up is still limited and non-responsive cases are often not reported in the literature, leading to publication bias and potentially overestimating treatment efficacy. Furthermore, most case reports had short follow-up, and actual clinical benefit for patients may be better measured by transfusion-free survival with long-term follow-up, since transfusion-dependency is associated with reduced quality of life and significant morbidity [15]. Recent multicenter studies showed evidence of PRCA relapse or persistence in some cases [16]. In line with these reports, our study provides first strong evidence for low relapse rates, but even larger cohorts are needed to better understand mechanisms of non-response and relapse.
Overall, the outcomes related to hemoglobin recovery and overall survival further support the potential of daratumumab as an effective therapeutic option for PRCA. Hemoglobin recovery, achieved in 65% of patients at 12 months, along with an overall survival of 81% at 12 months, suggests that daratumumab not only facilitates transfusion independence but also enhances hematologic recovery and survival in these high-risk patients. Importantly, only one case of PRCA relapse was documented, and only one patient experienced mortality due to hemolytic anemia, indicating durable responses and manageable safety outcomes. This underscores the complexity of managing post-allogeneic HCT complications and the need for ongoing supportive care and monitoring in this patient population.
In terms of infections, as CD38 is expressed at the surface of activated CD4+T cells, this study cannot rule out that daratumumab might have played a role in predisposing patients to infections, such as pneumocystis or viral infections [16, 17].
The relatively rapid median onset of PRCA following allogeneic HCT (55 days) underscores the need for early and effective intervention, which daratumumab appears to provide for the majority of patients. Daratumumab can induce complete response and transfusion-independence even after a single application. Furthermore, the alternative of subcutaneous application may offer patients and physicians alike to act timely where PRCA treatment is indicated.
To the best of our knowledge, this is the largest report of patients receiving daratumumab even as first-line treatment for PRCA, with promising responses compared with historical cohorts. A systematic literature review was conducted to evaluate the current role of daratumumab for PRCA. Relevant studies were identified through a comprehensive search of PubMed, with no language or publication date restrictions to ensure an inclusive dataset. Search terms included “daratumumab,” “pure red cell aplasia,” “PRCA,” “CD38 monoclonal antibody,” and “transplantation,” combined with Boolean operators. A qualitative synthesis of findings was conducted due to heterogeneity in study design and outcome reporting across studies, identifying 15 articles describing a total of 46 patients (Table 3) [7–9, 11–13, 16, 18–26]. Only 5 studies reported more than one patient. Most frequent administration route in case reports was intravenous, while the two largest studies to date included more patients with subcutaneous daratumumab. Synthesized response rate over all reports (except the present one) with >1 patient was 87%, and most responses occurred early after a median of two doses. In contrast, all case reports showed response in each patient.Table 3. Current reports on daratumumab for PRCA.PublicationNDiagnosisPrior treatmentsDosingDosesTreatment start from HCT in daysResponseWeverling et al.14AML, MDS, MPN, SCD, lymphomarituximab (43%), DLI (29%), bortezomib (7%)1800 mg SC1–660–298993% (defined by achievement of reticulocytosis), no relapseLongval et al.11AML, MDS, MPN, SAA, DADA2rituximab, EPO, thrombopoietin receptor agonist7 with IV and 4 with SCMedian of 3Median of 25591% (defined by transfusion independence)Giammarco et al.6Hematological diseasesrituximab, EPO, thrombopoietin receptor agonist1800 mg SC2NA83% (defined by transfusion independence)Frioni et al.3NREPO, plasma exchange, rituximab1800 mg SC2–8100–1802 responses, 1 with no response after 8 dosesDesai et al.3AA, AMLTapering of IS, IVIG, rituximab, steroids, plasma exchange, bortezomib2 IV and 1 SC4–6180–730100%Chapuy et al.1MDStapering of IS, steroids, rituximab, darbepoetin16 mg/kg IV6390After first doseBathini et al.1SAATapering of IS, Steroids, rituximab, bortezomib16 mg/kg IV4411After first doseRautenberg et al.1AMLTapering of IS, rituximab16 mg/kg IV2206After second doseSalas et al.1AATapering of IS, rituximab, steroids, plasma exchange bortezomib16 mg/kg IV6700After 6^th^ doseHenig et al.1Chronic neutropeniaTapering of IS, rituximab, bortezomib16 mg/kg IV5320After 4^th^ doseYates et al.1DOCK8 deficiencyTapering of IS16 mg/kg IV3397After third doseMartino et al.2AML, MDSNR16 mg/kg IV2, 3205, 270After first and second doseAsawapanumas et al.1AMLTapering IS16 mg/kg IV1146After first doseWu et al.1MDSTapering IS, rituximab16 mg/kg IV3209After second doseDeng et al.1AMLTapering IS, plasma exchange, interferon, MSC16 mg/kg IV52701After second doseDovern et al.1SCDNone1800 mg SC460After second doseIV intravenous, SC subcutaneous, IS immunosuppression, MSC mesenchymal stem cells, IVIG intravenous immunoglobulins, MDS myelodysplastic neoplasm, AML acute myeloid leukemia, SCD sickle cell disease, AA aplastic anemia, MPN myeloproliferative neoplasm, NR not reported.
Daratumumab’s mechanism of targeting CD38 on immune cells, particularly on plasma cells that may contribute to PRCA pathogenesis, likely plays a key role in its therapeutic effect. This immunomodulatory function is especially relevant in our cohort, where 93% of patients received in vivo T-cell depletion, a factor often associated with increased risk of PRCA due to reduced immune regulation [27]. The effective use of daratumumab in patients already heavily pretreated for PRCA, including 64% who had received alternative therapies like rituximab, cyclosporine A, and steroids, also highlights its potential role as a valuable second-line or salvage therapy when conventional treatments fail to yield desired outcomes.
However, the high number of patients that died of GvHD suggests that while daratumumab effectively targets PRCA, it does not mitigate all allogeneic HCT-related risks, particularly those associated with immune reconstitution and GVHD. This finding highlights the need for further studies to investigate combination and frontline strategies that may complement daratumumab’s efficacy while also addressing GVHD and infection risks.
PRCA following allogeneic HCT exerts a profound and multifaceted impact on patient quality of life, compounding the already demanding post-transplant recovery period. The near-universal transfusion dependence seen in this cohort reflects a daily reality of physical fatigue, reduced functional capacity, and frequent hospital visits that disrupt personal and social routines. Patients often experience emotional distress from prolonged uncertainty and delayed engraftment, especially when PRCA proves refractory to initial immunosuppressive therapies. The median 88-day delay before initiating daratumumab underscores a period of clinical vulnerability that severely diminish overall well-being. Additionally, the psychological toll of needing continuous transfusions and facing the risk of iron overload or alloimmunization can erode a patient’s sense of autonomy and long-term hope. While daratumumab ultimately restored transfusion independence in most cases, the interim period of symptomatic anemia, hospital dependence, and anxiety about transplant failure defines PRCA as a condition with heavy physical and psychosocial burdens that extend well beyond its hematologic profile.
While the present study focused on the treatment of PRCA after HCT, prevention of PRCA, particularly in the setting of major ABO mismatch, remains a clinical challenge, but several strategies have been proposed to mitigate its risk. For instance, decrease of isoagglutinin titers by in vivo immunoadsorption before allogeneic HCT does not only lack severe complication but also leads to a reduction in demand of RBC transfusion after engraftment and may reduce the incidence of PRCA in these patients [28]. Furthermore, use of a standardized pretransplant isoagglutinin reduction strategy including donor-type secretor plasma infusions is both safe and efficient in preventing progenitor cell infusion-associated hemolysis and is associated with low rates of post-transplant PRCA [29]. Post-transplant strategies, such as early tapering of immunosuppression or the use of rituximab in high-risk mismatched transplants, have also been proposed to facilitate donor erythroid engraftment. Furthermore, graft manipulation techniques like CD34+ selection or T-cell depletion may impact the risk, though data remain inconclusive. Despite these efforts, no standardized preventive protocol exists, and approaches are typically tailored based on institutional experience and individual patient risk factors.
We acknowledge limitations of the present study. We did not have systematic data on antibody titers before and after daratumumab treatment, as well as detailed data on dosing and timing of treatment lines other than daratumumab (such as cyclosporine A, rituximab, steroids). The application schedule and dosing of daratumumab varied significantly, reflecting the individualized approach often needed in complex allogeneic HCT patients. The most common dosing regimen, 16 mg/kg, administered weekly, aligns with standard daratumumab dosing in other hematologic indications. Another option in addition to daratumumab could be the other anti-CD38 antibody isatuximab that showed activity in a case report [30]. To address its potential, a randomized trial is currently recruiting participants to investigate the efficacy of isatuximab after a “watch and wait” phase in ABO-mismatched PRCA (NCT05559827). Last, recent reports descriped successful treatment of PRCA in major ABO-mismatched allogeneic HCT with single agent BTK inhibition such as with ibrutinib [31]. In our cohort, none of the patients received BTK inhibition and future studies should focus on novel treatment sequences in non-responders as well as identification of subgroups that may benefit from individual treatment approaches.
In conclusion, this study demonstrates that daratumumab may be a promising treatment option for PRCA following allogeneic HCT, with the ability to reduce transfusion dependency, support hemoglobin recovery, and improve survival. Future research should focus on optimizing and harmonizing dosing and administration schedules, as well as exploring combination therapies to further reduce post-allogeneic HCT complications and enhance patient outcomes in this vulnerable population.
Earlier daratumumab use, standard dosing, and possibly fewer prior therapies seem associated with better outcomes, while delayed treatment and severe infections, and yet unknown complex transplant variables may worsen prognosis and influence treatment adherence. Based on this, we provided expert positions suggesting the early use and first-line treatment, especially for patients with severe anemia, rapid clinical decline, or contraindications to standard immunosuppressive therapies (Table 4). By adhering to these considerations, clinicians can maximize the therapeutic benefits of daratumumab while minimizing risks, develop studies, ultimately improving outcomes and quality of life for patients with PRCA following allo-HCT.Table 4. Practical considerations.Patient selection: ◦ Use daratumumab early in transfusion-dependent PRCA, especially within 2–3 months post-HCT. ◦ Consider first-line use in patients with severe anemia, rapid clinical decline, or contraindications to standard immunosuppressive therapies. • Administration and dosing: ◦ Preferred regimens: ▪ IV infusion: 16 mg/kg weekly for 4–6 doses. ▪ SC injection: 1800 mg weekly, offering similar efficacy with greater convenience. ◦ Reassess response after 2–4 doses; consider extending to 8 doses if needed. • Monitoring and supportive care: ◦ Employ full infection prophylaxis and monitor for CMV reactivation and other infections. ◦ Use premedications to prevent infusion reactions; monitor closely during initial doses. ◦ Coordinate care with transplant and infectious disease teams to manage GVHD and infection risks. • Follow-up and long-term care: ◦ Monitor hemoglobin and reticulocyte counts biweekly for 3 months, then quarterly for 1 year. ◦ Be vigilant for PRCA relapse; re-treatment with daratumumab may be considered if necessary. • Therapeutic positioning: ◦ Prioritize daratumumab over rituximab in settings requiring rapid hematologic response. ◦ Consider combination approaches or alternative anti-CD38 agents for refractory or relapsed PRCA.
The reference list from the paper itself. Each links out to its DOI / PubMed record.