Iodine supplementation for pregnancy in Portugal: identification of nutritional composition of iodine containing supplements and characterization of pharmacy dispenses from 2008-2022
Sarai Isabel Machado, Susana Roque, Maria Lopes-Pereira, Maria José Costeira, Patrício Costa, Nuno Borges, Ruben Pereira, Zilda Mendes, António Teixeira Rodrigues, Joana Almeida Palha

TL;DR
This study examines iodine supplement use during pregnancy in Portugal, finding that supplementation duration is below recommended levels despite increased sales.
Contribution
The study provides a detailed characterization of iodine supplement sales and usage patterns among pregnant women in Portugal from 2008 to 2022.
Findings
88% of iodine-containing supplements met the recommended iodine concentration.
Annual sales of iodine supplements increased, reaching 109 µg per day in 2022.
Supplementation duration averaged 4.5 months, far below the recommended 18 months.
Abstract
Iodine is essential for the proper development of the central nervous system. In Portugal, despite of self-reports of iodine supplements intake by pregnant women, iodine deficiency still prevails. This study intended to characterize the pharmacy sales of iodine-containing supplements and their use by women in Portugal. Data from all available supplements with indication for use in the prenatal time, for the period 2008-2022, was obtained from the Portuguese Association of Pharmacies. To infer from the use of iodine supplements by women during preconception, pregnancy and lactation, pharmacy dispenses, between 2019 and 2021, were collected from a sample of female consumers, identified with at least one prescription of iodine-containing supplements. Eighty-eight per cent of the iodine-containing supplements state the recommended iodine concentration. The annual sales increased…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
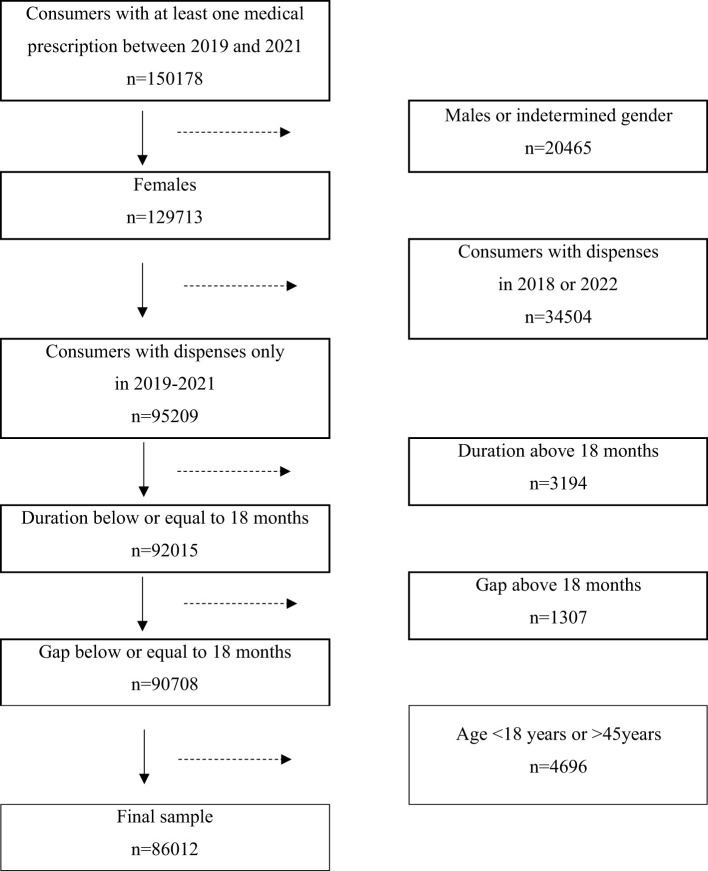 Figure 1
Figure 1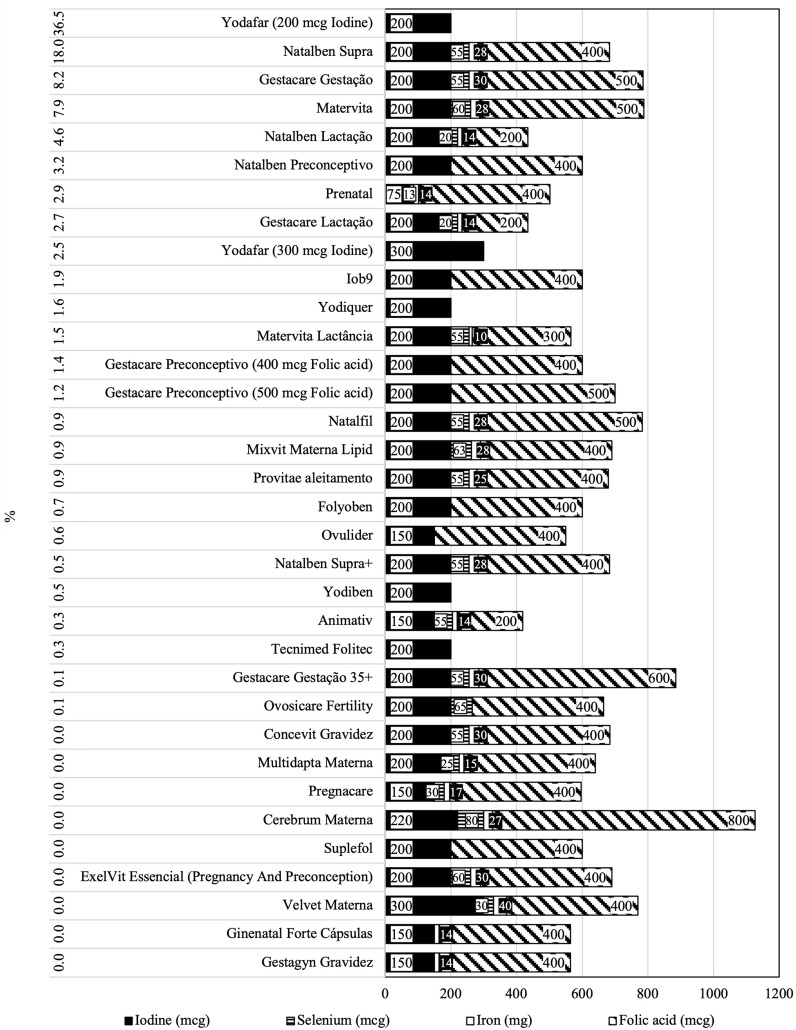 Figure 2
Figure 2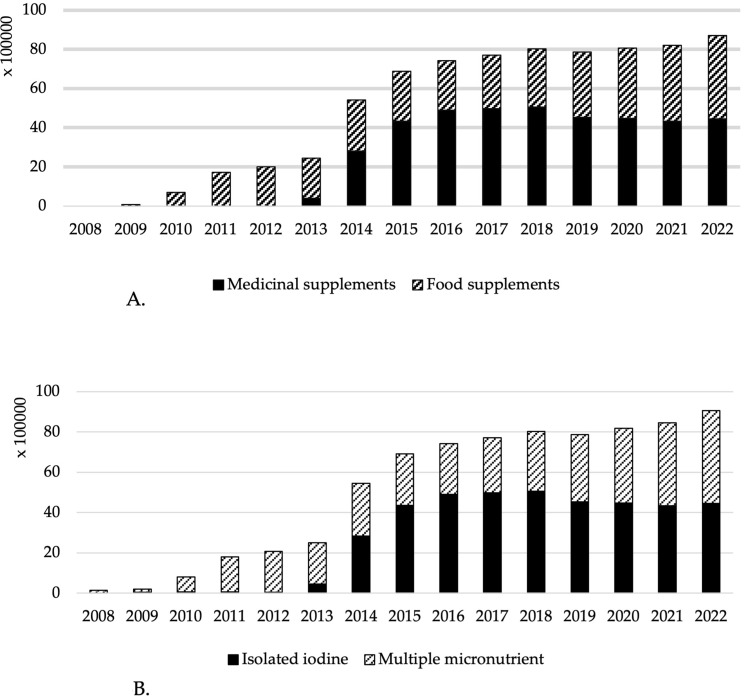 Figure 3
Figure 3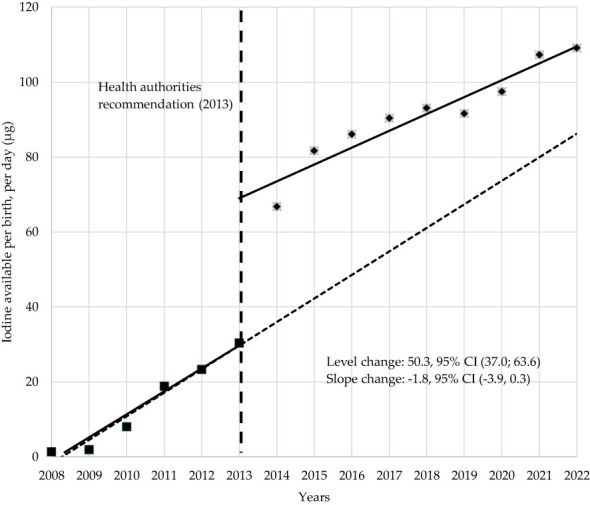 Figure 4
Figure 4| Year | Units sold | Units sold growth | Number of products | Presentations growth | Number of births | Iodine sold per day per birth (μg) | *Including the estimation of sales from pharmacies and mass market (μg) | |
|---|---|---|---|---|---|---|---|---|
| 2008 | 22782 | 1 | 103541 | 1 | – | |||
| 2009 | 22455 | -1% | 3 | 200% | 98430 | 2 | – | |
| 2010 | 57906 | 158% | 6 | 100% | 100280 | 8 | – | |
| 2011 | 104733 | 81% | 9 | 50% | 95823 | 19 | – | |
| 2012 | 108024 | 3% | 9 | 0% | 88969 | 23 | – | |
| 2013 | 122267 | 13% | 15 | 67% | 82064 | 30 | – | |
| 2014 | 232421 | 90% | 18 | 20% | 81591 | 67 | – | |
| 2015 | 282749 | 22% | 22 | 22% | 84584 | 82 | – | |
| 2016 | 303835 | 7% | 24 | 9% | 86281 | 86 | – | |
| 2017 | 322214 | 6% | 26 | 8% | 85315 | 90 | – | |
| 2018 | 339792 | 5% | 25 | -4% | 86256 | 93 | 94 | |
| 2019 | 333195 | -2% | 24 | -4% | 85963 | 92 | 101 | |
| 2020 | 367202 | 10% | 29 | 21% | 83907 | 98 | 104 | |
| 2021 | 389944 | 6% | 30 | 3% | 78890 | 107 | 117 | |
| 2022 | 423044 | 8% | 28 | -7% | 82987 | 109 | 114 | |
| Sample characterization (n=86012) | M (SD) |
|---|---|
| Age (years) | 32 (6) |
| Number of dispenses | 2 (1) |
| Iodine content per dose (µg) | 206 (5) |
| Supplementation coverage (months) | % women |
| 0-1 | <1% |
| 1-2 | 40% |
| 2-3 | 5% |
| 3-4 | 15% |
| 4-5 | 2% |
| 5-6 | 10% |
| 6-7 | 10% |
| 7-8 | 1% |
| 8-9 | 6% |
| 9-10 | 1% |
| 10-11 | 3% |
| 11-12 | 2% |
| 12-13 | <1% |
| 13-14 | 1% |
| 14-15 | <1% |
| 15-16 | 3% |
| 16-17 | 2% |
| 17-18 | <1% |
| Grand Total | 100% |
- —Foundation for Science and Technology 10.13039/501100019370
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Disorders and Treatments · Neonatal Health and Biochemistry · Vitamin K Research Studies
Introduction
Pregnancy represents a particular time of susceptibility to malnutrition due to increased demands of nutrients (1–3). Therefore, current international recommendations advise the supplementation of folic acid, iron and iodine. Legislation and usage of micronutrient supplementation varies among countries and should be adjusted to target and prevent the risk of deficiencies in each population group (4, 5).
Portuguese women of childbearing age and pregnant were identified as iodine deficient in 2009 (6, 7). This led the health authorities, in 2013, to recommend daily iodine supplementation of 150-200 µg, in the form of potassium iodide during conception, pregnancy and lactation (8). Despite of over 70% of women in the Azores Islands, Covilhã and Minho region and 56% in Porto, reporting compliance with the supplement recommendation, pregnant women are still iodine deficient (median urinary iodine concentration below 150 µg/L) (9–12). These findings are concerning, given the need of iodine for the synthesis of thyroid hormones, which are essential for the proper development of the central nervous system (13) and for children to achieve their full intellectual performance (14). Iodine is mainly obtained through diet (mostly dairy products and seafood) (15) and iodine content in food depends on the geographic locations and production/agricultural practices (16). To maintain adequate intake and prevent iodine deficiency, many countries adopted food fortification strategies, particularly through iodized salt, currently covering 89% of households worldwide (17, 18). In Portugal, iodized salt is mandatory in the school age children’s canteens, which seems not to have been adopted (19). As for the general population, iodized salt is voluntary and represent a minor contributor to iodine intake, corresponding to only 11% of total salt sales (20). Irrespectively of the policy on iodized salt, iodine supplementation is recommended to pregnant women, given the higher requirements of iodine as the production of thyroid hormones increases (17).
The evidence on the lack of efficacy of supplementation measures in ensuring adequate iodine intake in Portuguese pregnant women raised questions about compliance and on whether timing of initiation is sufficient to recover iodine storages and promote an adequate status during pregnancy. To obtain evidence for whether additional health policy recommendations are needed, the present study characterizes the composition, availability, and yearly sales (2008 to 2022) of iodine-containing supplements in Portuguese pharmacies. In addition, from medically prescribed supplement dispenses to women, a cohort of female was identified to estimate the duration of iodine-containing supplements intake.
Methods
Characterization of iodine-containing supplements composition, availability, and evolution of sales from 2008 to 2022
Data from iodine-containing supplements sold in Portuguese pharmacies from 2008 to 2022 was provided by the Centre for Health Evaluation and Research, National Association of Pharmacies, that encompasses 94% of the Portuguese pharmacies. Supplements were classified as “medicinal supplements” (can only be sold in pharmacies, some of which requiring medical prescription, and are regulated by the National Authority of Medicines and Health Products) or as “food supplements” (can also be sold in the mass market and are regulated by the General Directorate for Food and Veterinary). All iodine-containing supplements with indication for use during the prenatal time, except those in liquid presentation (such as enteral feeding formulas as they usually target malnutrition), were considered. Data was retrieved from 2008 to 2022 sales on community pharmacies (iodine containing “medicinal” and “food” supplements) and mass market (for the 15 most sold iodine-containing “food supplements”). The share of mass market sales was provided by the company Health Market Research (it contains data mostly from onsite sales) (the information retrieved does not distinguish online from onsite sales).
Information on the products (composition on iodine, iron, folic acid and selenium; posology and dosage form) was obtained from the summary of product characteristics and, whenever necessary, complemented through the human medicinal products database (National Authority of Medicines and Health Products, I.P.) and web search.
Total iodine sold was calculated using iodine-containing supplement sales multiplied by the number of dosages per unit sold and the respective iodine content. Assuming that all iodine supplements sold are intended for women in preconception, pregnant, and/or lactating, an estimation was made for iodine sold per birth, per day. The number of births each year was retrieved from the National Institute of Statistics.
Iodine compliance assessment from anonymized individual-level dispenses data of iodine-containing supplements
Given that iodine supplementation is recommended for preconception, pregnancy, and lactation, we considered that aggregated data from pharmacy dispenses could help clarify for how long the supplements were being taken. For that, anonymized data on pharmacy dispenses of iodine-containing supplements, obtained between 2018 and 2022, associated to consumers with at least one prescription of iodine-containing supplements was collected.
Inclusion criteria
Female consumers with dispenses of iodine-containing supplements with at least one prescription, between 2019 and 2021.
Exclusion criteria
Pharmacy dispenses of consumers with undetermined gender or males. Consumers with iodine-containing supplement dispenses in 2018 and/or 2022 (due to the possibility of underestimating the duration of supplementation, as they could be taking supplements in 2017 and 2023, for which we did not have data). Consumer identifiers with more than one attributed tax identification number to prescriptions (without univocal relation, and therefore not possible to distinguish individual consumers). Consumers younger than 18 or older than 45 years of age (considered outside the childbearing age). Consumers with dispenses of iodine supplements for periods longer than 18 months (since these could be taken iodine supplements for reasons other than pregnancy). Consumers with time gaps between dispenses above 18 months (since these could constitute more than one pregnancy).
Upon application of the exclusion criteria to the initial 150178 consumers, the final sample comprised 86012 women (Figure 1). From each woman retrieved through a medical prescription, all other iodine-containing supplement sales were also obtained, irrespectively of whether associated with another prescription or not. Iodine availability and estimated supplementation coverage in months were assessed by the sum of units dispensed, iodine content of the supplement purchased, and dosage form.
Flowchart of the study cohort.
Statistical analysis
The descriptive analysis of supplements was performed using Microsoft^®^ Excel for Mac, Version 16.83, and statistical analysis was conducted using IBM SPSS, 29.0 for Mac. Data was analyzed for normality using the Shapiro-Wilk test, skewness, kurtosis coefficients, and histogram. An interrupted time series analysis, presented as a segmented linear regression, was conducted to assess iodine supplement sales before and after 2013, the year in which the recommendation for iodine supplementation to women during preconception, pregnancy and lactation, was issued in Portugal (21, 22). Statistical significance was considered for a p-value below 0.05.
Results
Characterization of iodine-containing supplements composition, availability and sales
From 2008 to 2022 sales, 34 iodine-containing supplement presentations were identified, 28 of which were classified as “food supplements” (27 multiple micronutrient formulation and 1 isolated iodine formulation) and 6 as “medicinal supplements” (3 multiple micronutrient formulation and 3 isolated iodine formulation). The nutritional composition of all iodine-containing supplements is presented in Figure 2, sorted by the percentage of total sales. Eighty eight percent of all supplements presented iodine content within the recommendations (150 - 200 µg). Three supplements had iodine content above recommendations (220, 300, and 300 µg, two classified as “food supplements” and one as “medicinal supplement”) and one had iodine content below the recommendations (75 µg, classified as “medicinal supplement”). Of the 30 multiple micronutrients supplements, 97% also had folic acid, 73% iron and 70% selenium in their composition. The 15 most sold iodine-containing “food supplements” represented 78% of iodine-containing food supplements sales in pharmacies. Of these 15 iodine-containing “food supplements”, 89% of sales were attributed to pharmacies and 11% to mass market.
Nutritional composition in iodine, folic acid, iron and selenium, sorted by best-selling iodine -containing supplements in percentage sales.
The sales were next stratified based on formulation and requirement of prescription. While before the recommendation (2013) of the health authorities on the supplementation to women during preconception, pregnancy and lactation, isolated iodine represented a minute fraction of the iodine sales, it rapidly increased thereafter, reaching 49% of total sales in 2022 (Figure 3A). Of notice, before the recommendation in 2013, most sales were from “food supplements”, and “medicinal supplements” sales greatly increased thereafter, reaching 53% of total iodine-containing supplement sales in 2022 (Figure 3B).
(A) Iodine sold (µg) per day attributed to medicinal supplements and food supplements from 2008 to 2022. (B) Iodine sold (µg) per day attributed to multiple micronutrient or isolated iodine formulas from 2008 to 2022.
Unitary sales, iodine sold, and year-over-year growth are presented in Table 1. The highest year-over-year unitary iodine-containing supplement sales growth was observed in 2010 and 2014 (158% and 90%, respectively). Iodine sold per day covers an estimated 56% of the recommendation requirements (114 vs. 200 µg/day) for the births of 2022 (Table 1).
To understand the influence of the health authorities’ recommendations on iodine supplementation, a separate analysis was made, before and after 2013 (Figure 4). In the year of the recommendation, 2013, a significant estimated 50.3 µg/day per birth increase was observed (p < 0.001, CI 95% = [37.0; 63.6]. No differences were found regarding the growth trend before and after the 2013 (p = 0.088, CI 95% = [-3.9; 0.3]). The growth trend from 2008 to 2022 indicates that iodine available increased each year an estimated 6.3 µg/day per birth (p < 0.001, CI 95% = [4.4; 8.1]).
Segmented regression of iodine available, per birth, per day, before and after 2013.
Duration of iodine-containing supplements intake
From the sample of 86012 women (Table 2), between 2019 and 2021, the median duration of supplementation was of 4.5 months (IQR = 5.0). Eighty three percent of women dispenses did not cover the expected duration of pregnancy (9 months), and less than 1% had iodine available for the recommended period of 18 months (3 months before conception, 9 months of pregnancy, and 6 months during lactation) (5).
Discussion
This study shows that availability of iodine-containing supplements in pharmacies increased throughout the years, particularly after the recommendation by the national health authorities, in 2013, for iodine supplementation to women during preconception, pregnancy, and lactation. Most presentations have iodine content within the recommended content per serve (150 - 200 µg). Despite of a great variety of presentations categorized as “food supplements”, most iodine sold is in the format of “medicinal supplements” and require medical prescription. Interestingly, with respect to formulation, the multiple micronutrient supplements have now a similar contribution to iodine sold as isolated iodine supplements (51% and 49%, respectively). This is in accordance with information reported by Portuguese pregnant women (9). Of notice, most multiple micronutrients supplements also contained folic acid, iron and selenium, elements well described to be relevant during pregnancy. In Portugal, there seems to be adequacy in folic acid (supplementation is well implemented), and in selenium (23), while iron deficiency is still prevalent (24). To highlight that both selenium and iron availability are known to affect thyroid function and modulate the response to iodine prophylaxis (25).
When considering the overall annual sales, and the number of births, the total amount of iodine sold from supplements per day, per birth, reached a maximum of 114 µg/day in 2022, which is quite below the proposed for supplementation (200 µg/day). The contribution of iodine from supplements, together with dietary intake, should reach 250 µg/day during pregnancy and lactation, as recommended by the World Health Organization United Nations Children’s Fund-UNICEF) and the Iodine Global Network (26). Globally, there was an increase in iodine-containing supplement sales and estimated iodine sold per birth, since 2008, with two major highs in 2010 (the year after the first studies reporting iodine deficiency in pregnant Portuguese women) and 2014 (the year after the recommendation on iodine supplementation by the national health authorities). Supplement sales have now stabilized.
Analysis from the cohort obtained from pharmacy dispenses show that compliance with the recommendation is partial; less than 1% of women take iodine-supplements during the suggested 18 months, with a median of 4.5 months of duration (5, 8). Women are therefore likely to initiate supplementation when already pregnant and/or interrupt supplementation before the end of lactation. This is in accordance with the data presented for the Porto region of Portugal, where only 56% of women reporting the use of iodine-containing supplements initiated intake earlier than the sixth week of pregnancy (11). The data also supports the hypothesis that women may terminate iodine supplement intake by the end of the first trimester, which is the time when folic acid intake is generally completed (27). Of notice, a shorter than expected period of iodine-supplement may justify that the urinary iodine levels remain low in Portuguese pregnant women, despite of the reported over 70% compliance with iodine supplementation (9, 10, 12). Irrespectively of the reason, women are not being adequately informed on and/or to the adequate timings for iodine supplementation. This calls for the need of literacy campaigns to health professionals (28) and to women (29). The observation that pharmacy sales cover around 89% of iodine prenatal food supplement sales in the country creates an opportunity to promote literacy campaigns in that setting.
The study presents some limitations. When overall sales alone are considered, the total iodine intake value can be overestimated, since men and non-pregnant women were not excluded (even though analysis focused on supplements targeting women during preconception, pregnancy and lactation). When the data is considered based on the dispenses, actual intake and compliance could have been overestimated since women may purchase iodine supplements without fiscal number or individual healthcare identifier. Sales of iodine-containing supplements do not assure that women will take them; in such circumstance the data presented may be overestimated. No additional information, such as on health status, living conditions, or preconception/pregnancy/lactating status, which could influence the purchasing behavior.
Conclusion
This study contributes to the evidence that iodine intake by women during preconception, pregnancy and lactation is not achieving the levels considered sufficient. Altogether, the current evidence in Portugal supports the national health authorities to implement additional measures to ensure adequate iodine intake to women who intend to become pregnant, pregnant and through lactation. These include universal salt iodization and literacy campaigns to women, health professionals and the public.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hanson MA Bardsley A De-Regil LM Moore SE Oken E Poston L. The International Federation of Gynecology and Obstetrics (FIGO) recommendations on adolescent, preconception, and maternal nutrition: “Think Nutrition First. Int J Gynaecol Obstet. (2015) 131 Suppl 4:S 213–53. doi: 10.1016/S 0020-7292(15)30023-0 26433230 · doi ↗ · pubmed ↗
- 2World Health Organization. WHO recommendations on antenatal care for a positive pregnancy experience. Geneva: World Health Organization (2016).28079998 · pubmed ↗
- 3Killeen SL Donnellan NO’Reilly SL Hanson MA Rosser ML Medina VP. Using FIGO Nutrition Checklist counselling in pregnancy: A review to support healthcare professionals. Int J Gynecology Obstetrics. (2023) 160:10–21. doi: 10.1002/ijgo.14539 PMC 1010832436635083 · doi ↗ · pubmed ↗
- 4Doru B Hockamp N Sievers EHülk PLücke T Kersting M. Adherence to recommendations for nutrient supplementation related to pregnancy in Germany. Food Sci Nutr. (2023) 11:5236–47. doi: 10.1002/fsn 3.v 11.9 PMC 1049457537701189 · doi ↗ · pubmed ↗
- 5TuncalpÖRogers LM Lawrie TA Barreix M Peña-Rosas JP Bucagu M. WHO recommendations on antenatal nutrition: an update on multiple micronutrient supplements. BMJ Glob Health. (2020) 5. doi: 10.1136/bmjgh-2020-003375 PMC 739401732732247 · doi ↗ · pubmed ↗
- 6Costeira MJ Oliveira P Ares Sde Escobar GM Palha JA. Iodine status of pregnant women and their progeny in the Minho Region of Portugal. Thyroid. (2009) 19:157–63. doi: 10.1089/thy.2008.0249 18976166 · doi ↗ · pubmed ↗
- 7Limbert E Prazeres S Sao Pedro M Madureira D Miranda A Ribeiro M. Iodine intake in Portuguese pregnant women: results of a countrywide study. Eur J Endocrinol. (2010) 163:631–5. doi: 10.1530/EJE-10-0449 20643757 · doi ↗ · pubmed ↗
- 8Direção-Geral da Saúde (DGS). Aporte de iodo em mulheres na preconceção, gravidez e amamentação. In: Aporte de iodo em mulheres na preconceção, gravidez e amamentação (Lisboa: Direção-Geral da Saúde) (2013).