A Rare Cause of Submucosal Tumor-like Lesion
Tomoya Nakamura, Yujiro Kawakami, Hiroshi Nakase

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
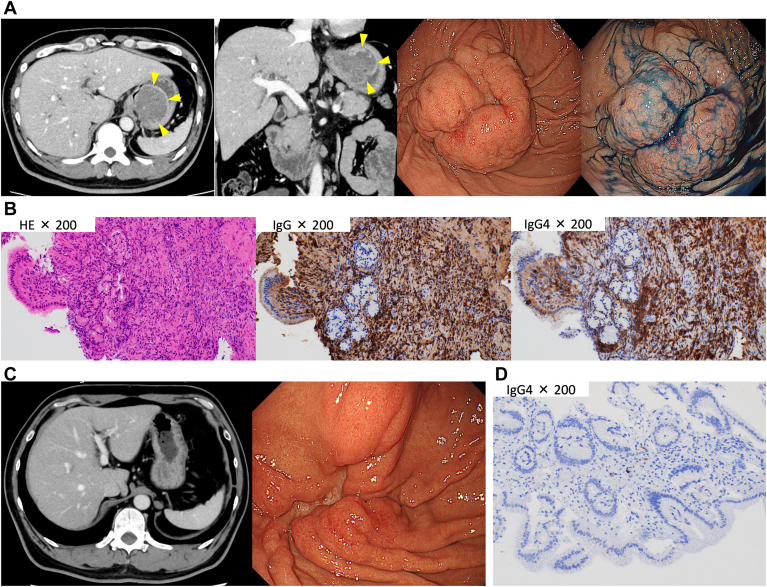 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Tumor Research and Treatment · Metastasis and carcinoma case studies · Gastrointestinal disorders and treatments
A 49-year-old man presented with upper abdominal pain. Laboratory tests revealed normal serum carcinoembryonic antigen and carbohydrate antigen 19-9 levels and elevated serum immunoglobulin G4 (IgG4) levels (1412 mg/dL). Contrast-enhanced computed tomography revealed bilateral submandibular gland enlargement, diffuse pancreatic enlargement, and a 55-mm enhanced mass in the stomach fundus (Figure A). Esophagogastroduodenoscopy revealed a submucosal tumor (SMT)–like lesion with an ulcer in the fundus (Figure A). We performed endoscopic biopsy of the ulcer part of the SMT-like lesion. Histopathology revealed >10 IgG4-positive lymphoplasmacytic cells/high-power field, with an IgG4/immunoglobulin-positive cell ratio of >40% (Figure B). Based on the laboratory, radiological, and pathological findings, the patient was diagnosed with IgG4-related gastrointestinal diseases (IgG4-GIDs). Treatment was initiated with 45 mg of prednisolone daily, with the dosage was tapered gradually. Contrast-enhanced computed tomography and esophagogastroduodenoscopy performed 3 months later revealed drastic shrinkage of the gastric lesion (Figure C). No IgG4-positive plasma cell infiltration was detected in endoscopic biopsy specimens of the lesion (Figure D).
IgG4-GID is associated with morphological changes, including ulcers, strictures, and SMT. Gastrointestinal lesions associated with IgG4-related disease are often misdiagnosed as gastrointestinal stromal tumors based on imaging findings. IgG4-GID is commonly diagnosed postoperatively, with few cases diagnosed through endoscopic biopsy.