Concurrent Renal Cell Carcinoma Diagnosis in a Married Couple: Risk Factors and Unmet Survivorship Needs
Matthew Lee, Liwei Jia, Richard Ahn, Jue Wang

TL;DR
A married couple was diagnosed with kidney cancer in quick succession, highlighting shared risk factors and the need for better support for couples facing cancer together.
Contribution
The study presents a rare case of concurrent RCC in a married couple and emphasizes the need for integrated care models for such patients.
Findings
Both partners shared risk factors like smoking and hypertension.
Occupational exposures may have contributed to their cancer risk.
No hereditary RCC syndromes were identified in the couple.
Abstract
Renal cell carcinoma (RCC) is the most common type of kidney cancer, but it is exceedingly rare for both partners in a married couple to be diagnosed with RCC within a short time frame. This case report describes a married couple who were diagnosed with RCC in close succession, exploring potential risk factors and highlighting the unmet survivorship needs of couples affected by cancer. Both partners shared risk factors, including a history of smoking and hypertension. The case focuses on the role of shared environmental exposures, specifically the wife’s occupation as a house cleaner and the husband’s role as a floor installer, in potentially contributing to carcinogenic risks in occupational settings. However, no hereditary RCC syndromes were identified. This report emphasizes the need for integrated care models that address the unique challenges faced by couples with concurrent cancer…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
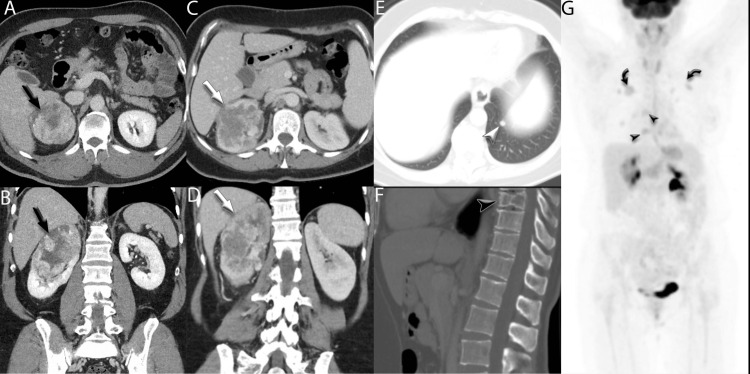 Figure 1
Figure 1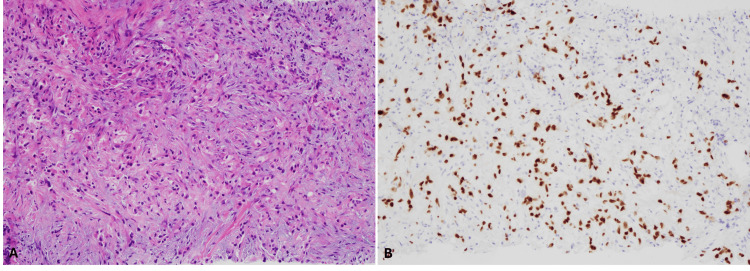 Figure 2
Figure 2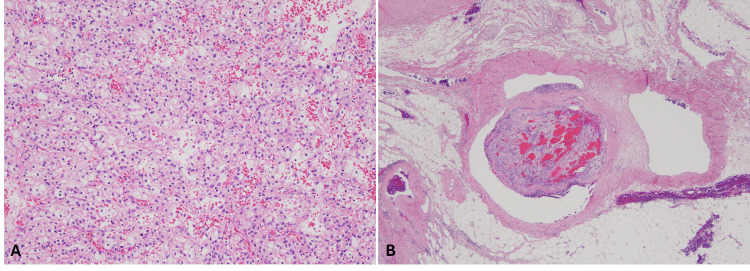 Figure 3
Figure 3| Risk Factor | Wife | Husband |
| Age (years) | 47 | 53 |
| Gender | Female | Male |
| Family History of Renal Cell Carcinoma | No | No |
| Occupation | House cleaner | Floor installer |
| Environmental Exposure | Cleaning agents and environmental toxins | Asbestos, chemicals, and dust from construction materials |
| Hypertension | Present | Present |
| Chronic Kidney Disease | Present | Absent |
| Renal Mass Size | 7 cm | 10.1 cm |
| Metastatic Disease | Present (lung, bone, liver) | Absent |
| Histological Features | Clear cell RCC with sarcomatoid features | Clear cell RCC |
| Systemic Therapy | Multiple lines of systemic therapies | Nephrectomy followed by one year of adjuvant pembrolizumab |
| Radiation Therapy | Received to lungs, spine, and osseous metastatic lesions | None |
| Outcome | Progressive despite therapy | In remission |
| Follow-up | Under intensive care and regular follow-up | Regular follow-up with imaging and lab tests |
| Unmet Survivorship Need | Wife | Husband | Daughter | Son |
| Psychosocial Support | Emotional strain from aggressive disease | Emotional burden from caregiving and health recovery | Emotional distress from witnessing illness | Emotional strain from balancing caregiving and personal life |
| Financial Assistance | Financial burden from treatment and insurance lapses | Limited by caregiving and health-related expenses | Potential financial strain from caregiving duties | Potential financial strain from caregiving duties |
| Palliative Care | Ongoing need for palliative care | No | Needs guidance on supporting the mother’s decline | Needs support in managing both parents' health |
| Treatment Access and Adherence | Interrupted care due to insurance issues | No interruptions, adheres to follow-up care | Managing mother’s treatment adherence | Helps with scheduling and follow-up care |
| Physical Rehabilitation | Yes | Yes | Assists with rehabilitation exercises | Helps with mobility and rehab tasks |
| Caregiver Support | Lack of formal caregiver support | Burden of caregiving while managing personal health | Significant caregiving responsibilities | Shares caregiving duties, potential stress |
| Support for Work and Lifestyle | Unable to work | Resumed full-time work despite caregiving strain | Need to adjust work hours for caregiving | Balances work and caregiving duties |
| Communication With the Care Team | Inconsistent communication during treatment gaps due to illness | Regular communication with the care team | Needs clear information on treatment plans | Needs help coordinating care plans |
| Long-Term Monitoring and Follow-Up | Needs extensive follow-up | Routine follow-up for remission surveillance | Needs to help manage health monitoring | Needs assistance with follow-up coordination |
| Health-Related Quality of Life | Decreased due to disease progression | Impacted by caregiving stress | Affected by caregiving stress | Impacted by caregiving responsibilities |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal cell carcinoma treatment · BRCA gene mutations in cancer · Multiple and Secondary Primary Cancers
Introduction
Renal cell carcinoma (RCC) is the most common form of kidney cancer, accounting for approximately 80% of all kidney malignancies and 74,000 new cases in the US each year [1,2]. Although most cases of RCC are sporadic, certain genetic predispositions, environmental exposures, and comorbid conditions can contribute to the development of RCC. The concurrent diagnosis of RCC in a married couple in a short timeframe is an exceptionally rare occurrence, raising questions about potential shared risk factors, disease etiology, and the psychosocial impact on affected couples.
Cancer diagnoses in family members, particularly in spouses, can place significant emotional and physical burdens on individuals and have been associated with increased marital distress [3]. While much focus has been placed on the individual experience of cancer, the unique challenges seen in couples diagnosed with concurrent malignancies are underexplored. The strain in marriage, caregiver responsibilities, financial stability, and emotional well-being can be exacerbated when both partners are affected by malignancy.
This case report aims to explore the rare occurrence of concurrent RCC diagnoses in a married couple, investigating potential shared risk factors and highlighting the unmet survivorship needs that arise in such situations.
Case presentation
A 47-year-old female, employed as a house cleaner, with a past medical history of hypertension and chronic kidney disease, presented to the hospital with gross hematuria and right flank pain. Initial CT imaging revealed a 7 cm lobulated mass in her right kidney along with bilateral pulmonary nodules and spinal lesions in T7, T9, and L3, concerning for metastatic disease (Figure 1).
Radiographic findingsAxial (A) and coronal (B) CT images demonstrating a large, heterogenous right renal mass (black arrows) in a 52-year-old man. No convincing evidence of metastatic disease was seen on CT of the chest, abdomen, or pelvis. Axial (C) and coronal (D) CT images demonstrating a similar heterogeneous right renal mass in a 47-year-old woman (white arrows). Additional findings suspicious for metastatic disease were seen, including a small left lower lobe pulmonary nodule (E, white arrowhead) and a lytic lesion in the T9 vertebral body (F, black arrowhead). PET/CT MIP image from a follow-up three months after baseline demonstrates numerous FDG-avid lesions in the lungs (curved black arrows) and bones (black arrowheads).PET/CT: positron emission tomography/computed tomography; MIP: maximum intensity projection; FDG: fluorodeoxyglucose
A subsequent biopsy of the renal mass in March 2021 confirmed clear cell RCC (ccRCC) with sarcomatoid features, a rare and aggressive subtype. To further assess the extent of disease, a biopsy was performed on the lung nodules, which confirmed that her metastatic disease was also ccRCC (Figure 2).
Pathological findings in a 47-year-old femaleThe biopsy of the lung lesion showed infiltrating tumor cells (A), and the renal origin was confirmed by immunohistochemical stain for PAX8 (B).
The patient began systemic therapy with pembrolizumab and axitinib in February 2021. She also underwent radiation therapy to her lungs and spine for symptomatic relief. Despite treatment, she developed progressive metastatic disease. Following a lapse in care due to insurance changes, the patient re-established care in July 2022 and was initiated on lenvatinib and everolimus. Over the following year, she underwent radiation to osseous metastatic lesions in her skull, pelvis, and femur. By July 2023, she transitioned to fifth-line therapy with tivozanib and continues to require intensive care due to the aggressive nature of her condition.
As she battled metastatic disease, her husband, a 53-year-old male, presented to the clinic in November 2022 with a three-month history of unexplained weight loss, fatigue, and intermittent abdominal pain. He had a long-standing history of hypertension and worked as a floor installer. A CT scan revealed a 10.1 cm right renal mass (Figure 1A, 1B). Radical nephrectomy confirmed stage III ccRCC (pT3aN0), with no evidence of lymph node involvement but some perinephric fat invasion (Figure 3).
Pathologic findings at the time of nephrectomy for an 8.7 cm renal mass in a 53-year-old man, husband of the previous patientThe histological evaluation showed clear cell renal cell carcinoma (RCC) with WHO/ISUP (World Health Organization/International Society of Urological Pathology) grade 3 (A). The tumor extended into the segmental branches of the renal vein (B).
The husband received one year of adjuvant pembrolizumab without significant side effects. Post-surgical recovery was uneventful, and his disease was monitored with regular imaging and laboratory tests. He remained in remission with no signs of recurrence or metastasis and was under surveillance. While managing his own recovery, he resumed full-time work while caring for his wife during her intensive treatment, compounding the emotional and physical strain of their concurrent diagnoses.
Both patients, although treated for RCC at different stages, faced significant challenges with the diagnosis and the physical, emotional, and psychological demands of cancer treatment. They had difficulty managing the dual burden of illness and caregiving responsibilities, and the lack of coordinated support for couples dealing with cancer became evident throughout the treatment process. Their adult children, aged 24 and 28, assumed primary caregiving roles, which placed significant emotional, physical, and financial strain on them.
Discussion
This case highlights the rare and complex situation of a married couple who were both diagnosed with RCC within a short time frame. The couple also had very contrasting clinical courses. The wife presented with an aggressive variant of metastatic RCC, and her husband was diagnosed with stage 3 ccRCC within one year. This illustrates the importance of understanding shared and individual risk factors, the psychosocial impact of cancer on couples, and the unmet survivorship needs in such challenging scenarios.
While approximately 90-95% of RCC cases are sporadic, the co-occurrence of RCC in a married couple raises important questions about shared risk factors that may have increased their risk [4]. Several studies have shown that there is a higher incidence of cancer clustering among married couples compared to those who are not couples. A nationwide population-based cohort study in Taiwan found that the risk of cancer clustering among couples was significantly higher than that among those who are not couples, with an incidence of 13.70% in couples versus 11.84% in those who are not couples [5]. Another study conducted in Japan reported that wives whose husbands developed cancer were at an increased risk of developing cancer themselves [6]. Overall, the accumulated evidence indicates that shared environmental exposures, socioeconomic status, lifestyle behaviors, dietary habits, and psychological stress are key factors contributing to the higher incidence of cancer among married couples. However, it's essential to note that these factors may not be deterministic but rather influence the likelihood of cancer development. Further research into these areas is necessary to better understand how shared risk factors among married couples can contribute to cancer incidence. Reporting these cases is crucial for knowledge accumulation in this area, helping guide future research and inform public health strategies. Additionally, this information is vital for health care planning, including cancer survivorship, as it can help tailor more effective prevention and support programs for affected individuals and families.
Interestingly, although smoking is the most recognized risk factor for developing RCC, both our patients were never-smokers [7]. However, both patients had long-standing hypertension, which has been established as a risk factor for RCC in a dose-response relationship [7,8]. This risk factor is particularly important given that both patients had limited access to primary care due to being uninsured, which likely contributed to inadequate hypertension management. Furthermore, both patients are Hispanic Americans, which is an ethnic group found to have nearly three times the odds of developing RCC compared to White Americans [9,10]. Beyond these socioeconomic factors, environmental exposures may have also played a role in the couple’s diagnoses. The husband worked as a floor installer, potentially exposing him to chemicals linked to RCC. For instance, per- and polyfluoroalkyl substances (PFAS) are found in numerous flooring products and have been linked to an increased risk for developing RCC [11]. Also, as a house cleaner, the wife was exposed to numerous cleaning chemicals, such as benzenes, which are a risk factor for RCC [7,12]. Both the husband and wife may have also been exposed to asbestos.
There are studies illustrating an increased risk of developing mesothelioma in family members of workers exposed to asbestos [13]. However, there are mixed results about whether asbestos is a risk factor for RCC [14,15]. There is only one previous case report illustrating a married couple who both developed RCC, and the husband had a long history of asbestos exposure, as he worked as a shipyard worker [16]. Given their occupational risk factors, it is possible that carcinogens from their respective workplaces were transferred through clothing and hair, increasing their risk of developing RCC.
Although emotional strain is common among cancer patients and family members, this couple’s experience was uniquely complex given their simultaneous diagnoses and contrasting disease courses. Among patients with RCC, married patients have better outcomes than widowed and single patients [17]. The reason is likely multifactorial, from stronger financial resources to better support systems. However, this protective effect may not extend to married couples when both partners are simultaneously battling malignancy. The wife experienced persistent anxiety and fear, which worsened as her disease progressed through multiple lines of therapy and when her husband was subsequently diagnosed with RCC. In contrast, the husband’s disease was surgically treated with a favorable prognosis. This dynamic caused the husband to struggle with feelings of guilt and self-blame. Although feelings of guilt and self-criticism are common in cancer patients, his feelings of guilt were intensified, as he felt his occupational exposures may have contributed to both of their illnesses [18]. Their experience highlights the unique emotional toll that emerges when married partners both face cancer diagnoses.
This case also highlights significant challenges in survivorship care for families navigating concurrent cancer diagnoses. While recovering from his nephrectomy, the husband returned to full-time work and was also managing the care of his wife. However, coordinating follow-up appointments proved difficult given the husband’s full-time work schedule, his own medical treatments, and his wife’s ongoing treatments. Although the wife utilized individual counseling services, there were no integrated counseling programs designed to support both partners through their concurrent diagnoses. Family and couples therapy can reduce distress and improve coping for both cancer patients and caregivers, and the need for joint therapy may be even greater when the caregiver is also managing their own concurrent cancer diagnosis [19]. The couple also faced significant financial strain due to their inability to work during their treatments. The wife experienced a lapse in insurance during a critical time of disease progression, but she was able to receive care after being approved for a financial assistance program at a safety-net hospital. Financial counseling and assistance programs are essential for families navigating concurrent cancer diagnoses. As seen by their challenges, a coordinated survivorship plan that incorporates joint counseling, same-day follow-up care, practical caregiver support strategies, and financial counseling is essential for couples dealing with concurrent cancer diagnoses.
Conclusions
In conclusion, this case report highlights the diagnosis of renal cell carcinoma (RCC) in a married couple within a span of one year, shedding light on the potential role of shared environmental exposures, lifestyle behaviors, and other contributing factors in the development of cancer among married couples. While these factors are not deterministic, they likely influence the increased likelihood of cancer in this case. The report emphasizes the importance of documenting such cases to enrich our understanding of cancer incidence in couples and contributes to the accumulation of knowledge in this area. Moreover, the findings underscore the significance of considering these shared risk factors in health care planning, especially in cancer survivorship programs, to better support individuals and families affected by RCC and other cancers. Further research is necessary to explore the intricate relationship between these factors and cancer development, paving the way for more effective prevention and treatment strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Renal cell carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up Ann Oncol Escudier B Porta C Schmidinger M 7067203020193078849710.1093/annonc/mdz 056 · doi ↗ · pubmed ↗
- 2Clinical review on the management of metastatic renal cell carcinoma JCO Oncol Pract Tran J Ornstein MC 1871961820223452949910.1200/OP.21.00419 · doi ↗ · pubmed ↗
- 3Cancer-related psychosocial challenges Gen Psychiatr Wang Y Feng W 035202210.1136/gpsych-2022-100871 PMC 954083436311374 · doi ↗ · pubmed ↗
- 4Kidney cancer: links between hereditary syndromes and sporadic tumorigenesis Semin Diagn Pathol Alchoueiry M Cornejo K Henske EP 174120243800865310.1053/j.semdp.2023.11.002 · doi ↗ · pubmed ↗
- 5Time-dependent risks of cancer clustering among couples: a nationwide population-based cohort study in Taiwan BMJ Open Wang JY Liang YW Yeh CC Liu CS Wang CY 08201810.1136/bmjopen-2017-018968 PMC 585523529467133 · doi ↗ · pubmed ↗
- 6Excess concordance of cancer incidence and lifestyles in married couples (Japan): survival analysis of paired rate data Cancer Causes Control Izumi S Imai K Nakachi K 5515581520041528063410.1023/B:CACO.0000036162.86921.09 · doi ↗ · pubmed ↗
- 7Environmental and modifiable risk factors in renal cell carcinoma Urol Oncol Navai N Wood CG 2202243020122238599310.1016/j.urolonc.2011.10.001 · doi ↗ · pubmed ↗
- 8Obesity, hypertension, and the risk of kidney cancer in men N Engl J Med Chow WH Gridley G Fraumeni JF Jr Järvholm B 1305131134320001105867510.1056/NEJM 200011023431804 · doi ↗ · pubmed ↗