LOWER TRAPEZIUS TRANSFER FOR IRREPARABLE ROTATOR CUFF TEAR: SYSTEMATIC REVIEW
Guilherme Trigueiro Alarcon, Jyotis Natacha Brito Corbin, Eduardo Misao Nishimura, Luciano Pascarelli, Eiffel Tsuyosho Dobashi

TL;DR
This systematic review shows that lower trapezius transfer surgery improves pain and function in patients with irreparable rotator cuff tears.
Contribution
The study provides a comprehensive evaluation of functional and pain outcomes after lower trapezius transfer for irreparable rotator cuff tears.
Findings
Pain levels significantly decreased from 7.1 to 2.4 on the VAS after surgery.
Functional scores improved from 49.5 to 78.3 using the ASES system.
The results support lower trapezius transfer as an effective surgical option for this condition.
Abstract
To evaluate functional results considering the final stages of function and postoperative pain in patients with irreparable rotator cuff tears undergoing surgical treatment by lower trapezius transfer. A systematic review of the literature was carried out following the PRISMA guidelines without restrictions on language and year of publication. The search was carried out in the following databases: MEDLINE/PubMed, EMBASE, Scopus and Cochrane Central Register of Controlled Trials. The main descriptors used were: "Rotator Cuff" OR "Rotator Cuff Injuries" OR Rotator Cuff Tear. The stages analyzed were pain, range of motion and function. We found 215 articles, of which 12 were included involving 374 participants. There was a statistically significant improvement comparing the pre and postoperative periods. The average intensity of pain was 7.1 and decreased to 2.4 according to the VAS. Using…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
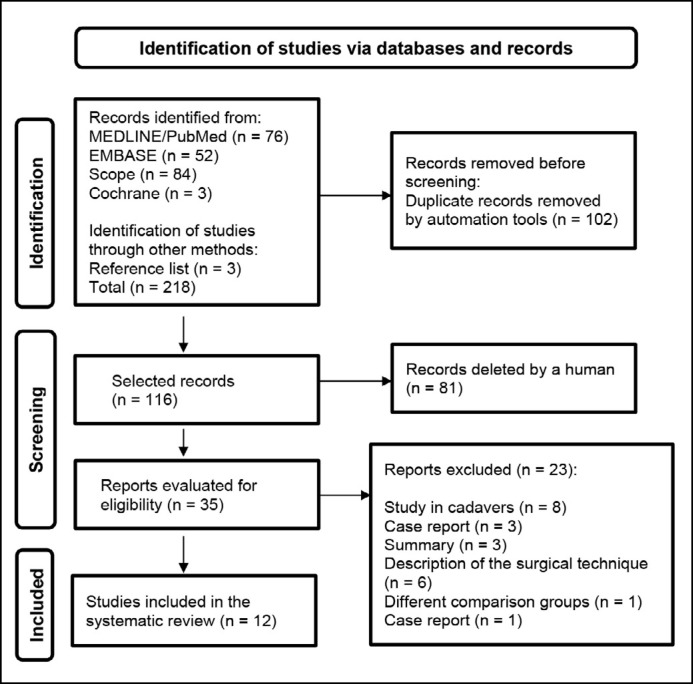 Figure 1
Figure 1| Author/ Year/ Country | Study design/follow-up | Sample size | Average age | Type of injury | Intervention | Comparison group | Type of graft | Instruments | MINORS |
|---|---|---|---|---|---|---|---|---|---|
| Almeida et al., 2023
| Retrospective case series | 10 | 40 and 62 years (mean 51.90) | Irreparable rotator cuff tears | Transfer of the lower trapezius | Pre and Post-operative | Knee flexor tendon grafts (semitendinosus and gracilis) | VAS | 16/12 |
| Baek et al., 2023
| Retrospective case series | 36 | 63.4±5.4 years | Irreparable postero-superior rotator cuff tears in the wrist | Lower trapezius transfer assisted by arthroscopy | Pre and Post-operative | Achilles tendon | VAS | 16/12 |
| Baek et al., 2022
| Cross-sectional retrospective study | 42 | 63.3±5.8 years | Irreparable postero-superior rotator cuff tears in the wrist | Lower trapezius transfer | Pre and Post-operative | Achilles tendon | VAS | 18/24 |
| Baek et al., 2022
| Retrospective case series | 36 | 63.1±65.5 years | Irreparable postero-superior rotator cuff tears | Lower Trapezius Transfer | Pre and Post-operative | Achilles tendon | VAS | 19/24 |
| Bozoğlan al., 2023
| Retrospective case series | 16 | 62±9 years (42-73 years) | Large irreparable rotator cuff tears | Lower trapezius tendon transfer | Pre and Post-operative | Long fibular allograft combined with interpositional repair with fascia lata | VAS | 16/12 |
| Chopra et al., 2023 | Retrospective case series | 19 | 56.7 years (range 29 to 72 years) | Large irreparable rotator cuff tears | Lower trapezius tendon transfer | Pre and Post-operative | Achilles tendon | VAS | 16/12 |
| Marigi et al., 2023
| Retrospective cohort comparison | 104 | 56.8 ± 7.9 years | Irreparable rotator cuff tears | Assisted by Arthroscopy Trapezius transfer | Pre and Post-operative | Achilles tendon | VAS | 17/24 |
| Elhassan et al., 2020
| Retrospective case series | 41 | 52 years (range 37-71 years) | Massive and irreparable postero-superior rotator cuff tear | Transfer of the lower trapezius | Pre and Post-operative | Achilles tendon | (1) VAS | 16/10 |
| Stone et al., 2020
| Retrospective case series | 15 | 52 years (age range 31-62 years) | Irreparable posterior-superior rotator cuff tears | Lower trapezius tendon transfer | Pre and Post-operative | Achilles tendon | VAS | 16/11 |
| Woodmass et al., 2020
| Retrospective case series | 8 | 53 years | Chronic massive posterior-superior rotator cuff tear | Arthroscopy-assisted lower trapezius tendon transfer | Pre and Post-operative | Achilles tendon | VAS | 18/24 |
| Valenti e Werthel et al., 2018
| Retrospective case series | 14 | 62 years (age range 50 to 70 years) | Irreparable posterior-superior rotator cuff tear | Transfer of the lower trapezius | Pre and Post-operative | Semitendinosus tendon | VAS | 16/12 |
| Elhassan et al., 2016
| Retrospective case series | 33 | 53 years (variation from 31 to 66 years) | Massive and irreparable postero-superior rotator cuff tear | Transfer of the lower trapezius | Pre and Post-operative | Achilles tendon | (1) VAS | 16/11 |
| Study | Pre-operative | Post-operative | ||||
|---|---|---|---|---|---|---|
| Pain | Range of motion | Function | Pain | Range of motion | Function | |
| Almeida et al., 2023
| 7,9 | Mean lateral rotation 31° | ASES function | 2.5 | Mean lateral rotation improved by 51° | ASES function 75.24±3.59 (p < 0.001) |
| Baek et al., 2023
| 4,5±1,2 | Forward elevation 134°±42° | ASES function | 1.4±0.7 (p < 0.001) | Frontal elevation 160°±30° (p=0.007) | ASES Function 83.7 ± 8.2 (p <0.001) |
| Baek et al., 2022
| 4,3 ± 1,6 | Active frontal elevation | ASES Function 55.8±16.7 | 1.7 ± 1.3 (p < 0.001) | Active frontal elevation | ASES function |
| Baek et al., 2022
| 4,5±61,8 | Active frontal elevation | ASES function | 1.3±61.0 (p < 0.001) | Active front elevation. | ASES function |
| Bozoğlan et al., 2023
| 6,1±1,1 | Active forward flexion 109°±24.7° | Constant - Murley score | 2.4±1.35 (p=0.007) | Active flexion advance 144°±22.21° in the postoperative period (p=0.005) | Constant - Murley score |
| Chopra et al., 2023 | 5,9±2 | Elevation | ASES function | 1.8±2 (p<0.001) | Elevation | ASES function |
| Marigi et al., 2023
| 6,2±2,5 | Front lift strength | Quick DASH score | 1,1±2,0 | Front lift strength | Quick DASH score |
| Elhassan et al., 2020
| 6 | Forward flexion 67° | Quick DASH score | 2 (p<0.001) | Forward flexion 133° (p<0.001) | Quick DASH score 18 (p<0.001) |
| Stone et al., 202024 | NR | Active elevation 98° | NR | NR | Active elevation 144° (P < 0.0001) | NR |
| Woodmass et al., 2020
| 2,85 | Forward flexion 101° | ASES function 12.5 | 1.17 | Forward flexion 146° (p = 0.031) | ASES function |
| Valenti e Werthel et al., 2018
| 7 | Flexion of 150° | Constant - Murley score | 2 (p<0.001) | Flexion 160° | Constant-Murley score |
| Elhassan et al., 2016
| NR | Flexion of 70° | Quick DASH score | NR | Flexion of 120° | Quick DASH score |
| Pre ASES | Post ASES | Avarege difference | Avarege difference | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Study or Subgroup | Significant | SD | Total | Significant | SD | Total | IV, Aleatory, IC95% | IV, Aleatory, IC95% | |
| Almeida et al., 2023
| 26.63 | 7.34 | 10 | 75.24 | 3.59 | 10 | 23.3% −48.61 [−53.67, −43.55] |
| |
| Baek et al., 2022
| 57.1 | 13.4 | 36 | 83.7 | 8.2 | 36 | 23.2%-26.60 [-31.73,-21.47] | ||
| Bael et al., 2022
| 55.8 | 16.7 | 42 | 82.7 | 8.6 | 42 | 23.0%-26.90 [−32.58, −21.22] | ||
| Baek et al., 2023
| 47.2 | 17.3 | 36 | 84.8 | 67.6 | 36 | 12.3% −37.60 [−60.39, −14.81] | ||
|
|
|
| |||||||
| Heterogeneity: Tau² = 138.61; Chi² = 47.17, df = 4 (P <0.00001); I² = 92% | |||||||||
| Test for overall effect: Z = 5.70 (P<0.00001) | |||||||||
| Test for subgroup differences: Not Applicable | |||||||||
|
| |||||||||
| Pre VAS | Post VAS | Avarege difference | Avarege difference | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study or Subgroup | Significant | SD | Total | Significant | SD | Total | Weight | IV, aleatory, IC 95% | IV, aleatory, IC 95% | |
| Almeida et al., 2023
| 7.9 | 0.74 | 10 | 2.2 | 2.2 | 10 | 13.20% | 5.70 [4.26, 7.14] |
| |
| Baek et al., 2022
| 4.3 | 16 | 42 | 1.7 | 1,3 | 42 | 18.30% | 2.6 [1.98, 3.22] | ||
| Baek et al., 2022
| 4.5 | 61.8 | 36 | 1.3 | 61 | 36 | 0.10% | 3.20 [-25.17, 31.57] | ||
| Baek et al., 2023
| 4.5 | 1.2 | 36 | 1.4 | 0,7 | 36 | 19.10% | 3.10 [2.65 3.55] | ||
| Bozoglan et al., 2023
| 6.1 | 1.1 | 16 | 2.4 | 1,35 | 16 | 17.00% | 3.70 [2.85, 4.55] | ||
| Marigi et al., 2023
| 6,2 | 2.2 | 72 | 1.1 | 2 | 72 | 18,00% | 5.10 [4.41, 5.79] | ||
|
|
|
| ||||||||
| Heterogeneity: Tau² = 1.04; Chi² = 41.66, df = 6 (P < 0.00001); I² = 86% | ||||||||||
| Test for overall effect: Z = 8.66 (P < 0.00001) | ||||||||||
| Test for subgroup differences: Not applicable | ||||||||||
|
| ||||||||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder Injury and Treatment · Shoulder and Clavicle Injuries · Orthopedic Surgery and Rehabilitation
INTRODUCTION
The topic involving the management of massive and irreparable rotator cuff tears is considered challenging, as surgical outcomes have not yet been definitively clarified. Some authors note a high failure rate in evaluating results.^ 1,2 ^ However, in clinical practice, the therapeutic indication is based on the following criteria, such as the rupture of two or more tendons, the duration of symptoms being longer than 6 months, tendon retraction greater than 5 cm, and a fatty infiltration grade of 3 according to the Goutallier classification, to indicate surgical intervention.^ 3 ^
In irreparable tears of the subscapularis, supraspinatus, and infraspinatus muscles, patients present significant dysfunction and pain. Thus, functional restoration and pain reduction are considered paramount,^ 4 ^ particularly in patients who are not candidates for shoulder arthroplasty due to age or high-level activity. Therefore, tendon transfers are considered surgical options with superior effects when performing reconstruction of the deficient rotator cuff.^ 2,5 ^ Recently, the orthopedic literature has highlighted that the lower trapezius transfer (LTT) warrants attention in the treatment of posterosuperior rotator cuff tears, particularly when associated with weakness in external rotation and signs of relapse in external rotation.^ 6 ^ Therefore, researchers have shown increasing interest in investigating the effects of this transfer to treat deficiencies in degenerative shoulder conditions.^ 7 ^ We know that, initially, LTTs were indicated to restore external rotation surgically in the treatment of brachial plexus paralysis.
A recent systematic review reported that LTT improves clinical outcomes in patients with irreparable rotator cuff tears. It presents a similar complication and reoperation rate when compared with other surgical alternatives in this group of patients.^ 7,8 ^ What motivated the authors of this research was the absence of secondary studies evaluating the functional outcomes of surgical treatment. Therefore, this study aims to evaluate the functional results of LTT, considering functional aspects and pain in the pre and postoperative periods of patients with irreparable rotator cuff tears.
MATERIALS AND METHODS
This systematic review was conducted according to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses – PRISMA.^ 9 ^
Data Sources and Searches
To assist in the search for scientific publications of intervention studies, a clinical question was formulated based on the strategy defined by the PICO acronym.^ 10 ^ Therefore, we determined that: P = patients with irreparable rotator cuff injuries; I = interventions with the lower trapezius transfer; C = intervention comparing preoperative and postoperative results; O: the outcomes analyzed were pain and function by the ASES system in the pre and postoperative periods.
For pain assessment, we considered studies that used the Visual Analog Scale (VAS).^ 11 ^ For shoulder range of motion measurements, we considered studies that used a goniometer, and for shoulder function assessment, we considered studies that used the following questionnaires: Constant-Murley Score,^ 12 ^ American Shoulder and Elbow Surgeons (ASES)^ 13 ^ or Quick Disabilities of Arm, Shoulder & Hand (Quick DASH score).^ 14 ^
A researcher formulated the electronic search strategy in the databases MEDLINE/PubMed, EMBASE, Scopus, and Cochrane Central Register of Controlled Trials. Additionally, additional articles that could be included were searched in the reference lists of eligible studies.
The search terms used in the database searches were combined with the Boolean operators "AND" and "OR". The terms for the searches were as follows: Arthroplasty; Coracohumeral Impingement; Coracohumeral Impingement Syndrome; Coracohumeral Impingement Syndromes; Cuff Injury; Glenoid Labral Tear; Glenoid Labral Tears; Glenoid, Rotator Cuff Injury; Injuries; Injury; Orthopedic Procedures; Replacement, Shoulder; Rotator; Rotator Cuff; Rotator Cuff Injuries; Rotator Cuff Tear; Rotator Cuff Tear Arthropathy; Rotator Cuff Tears; Rotator Cuff Tendinitides; Rotator Cuff Tendinitis; Rotator Cuff Tendinosis; Rotator Cuff Tendinosis; Rotator Cuff, Coracohumeral Impingement; Rotator Cuff, Labral Tear; Shoulder; Shoulder Fractures; Shoulder Impingement Syndrome; Shoulder Injuries; Shoulder Joint; Shoulder Pain; Shoulder Prosthesis; Tear, Glenoid Labral; Tear, Rotator Cuff; Tears, Glenoid Labral; Tears, Rotator Cuff; Tendinitis, Rotator Cuff; Tendinosis, Rotator Cuff; Tendinosis; Tendinosis, Rotator Cuff.
The inclusion criteria for the studies were: (1) studies with individuals who underwent LTT for irreparable rotator cuff injury; (2) individuals of both sexes; (3) studies in any language; (4) without restrictions regarding the year of publication. The criteria for exclusion of articles were: (1) studies conducted on cadavers; (2) publication in the form of conference abstract, letter, editorial, case report; (3) literature reviews; (4) systematic reviews; (5) LTT for brachial plexus injury; (6) studies comparing LTT with other techniques.
The screening of articles was conducted using the Rayyan software, which enables a rapid selection of eligible studies.^ 15 ^ The evaluations of titles, abstracts, and the full reading of the articles were conducted by two researchers independently. Any discrepancies in the identification of articles were resolved among the research team members. After the full reading of the old ones, the following information was collected: authors and year of publication, study design, follow-up time, country where the study was conducted, sample size, average ages, intervention, and outcome results (pain, range of motion, and function).
The electronic search was conducted between January and February 2024.
Quality assessment of the studies
The analysis was performed by scoring the Methodological Index for Non-Randomized Studies (MINORS) score, which comprises eight items for non-comparative studies and 4 additional items for comparative studies.^ 16 ^
Compliance with Ethical Guidelines
This original article was based on previously published studies; therefore, it did not involve the direct extraction of data from study participants.
RESULTS
A total of 215 articles were identified in the databases used in this study, and three additional articles were selected through searches of the references of the included studies. 102 duplicate articles and 81 were excluded through the screening of titles and abstracts. Thus, we conducted a full reading of 35 articles, of which 12 were included in the qualitative synthesis.^ 17–28 ^ (Figure 1 illustrates the flowchart for selecting studies).
PRISMA flowchart of the study selection process.
Ten studies were classified as retrospective case series,^ 17,18,20–24,26–28 ^, one retrospective cohort study,^ 25 ^ and one study using a retrospective crossover design.^ 19 ^ These studies were conducted in Brazil,^ 17 ^ South Korea,^ 18–20 ^ Turkey,^ 21 ^ United States^ 22–26,28 ^ and France.^ 27 ^ The twelve studies included a total of 374 participants, with an average age of 61 years (ranging from 40 to 73 years). The participant demographics were as follows: 241 (64.4%) were male, and 133 (35.6%) were female. The average postoperative follow-up time was 22 months, ranging from 6 to 70 months.
The main indications for surgery were persistent pain, failure of conservative treatment,^ 17–20,22 ^ massive rotator cuff tear identified on MRI, association with fatty infiltration (Goutallier grade III or IV),^ 23–25,28 ^ presence of intact subscapularis^ 28 ^ and teres minor tendons, and limitation of active range of motion.^ 17–20,22 ^ Other criteria found in the studies were: arthritic changes by Hamada criteria grade 0, 1, 2;^ 19,28 ^ patients without neurological diseases;^ 19 ^ absence of glenohumeral osteoarthritis on X-rays (Hamada <3); no limitation of passive range of joint movements;^ 21 ^ and patients with deltoid muscle paralysis.^ 25 ^
The average MINORS score was 11.5 (range from 10 to 12) for non-comparative studies and 18 (range from 17 to 19) for the included comparative studies (Table 1).
Ten studies assessed pain using the EVA scale in the pre and post-operative periods.^ 17–23,25,27,28 ^ These studies indicated that there was a significant reduction in pain after surgical intervention. After evaluating the results, we observed a statistically significant improvement when comparing the pre and post-operative periods. The average pain intensity was 7.1 and decreased to 2.4 according to the EVA. Using the ASES system, the result improved positively where the initial average was 49.5 (poor result) and final was 78.3 (good result).
Table 2 summarizes the pre- and post-operative results, considering pain, ROM, and function, as assessed by ASES scales,^ 17–20,22,28 ^ the Constant-Murley Score,^ 21,27 ^ and the Quick DASH score.^ 23–25 ^ There was a statistically significant improvement during outpatient follow-up (p < 0.05).
Statistical analysis
The population size and the mean and standard deviation values for EVA pre-intervention and post-intervention, as well as the ASES score pre-intervention and post-intervention, were subjected to meta-analysis, and the results were expressed as mean differences. The percentage of variability attributable to heterogeneity among the studies was estimated using the I² statistic, with a p-value of less than 0.05 considered statistically significant.
Heterogeneity was classified based on I² values as follows: 25% low heterogeneity, 50% moderate heterogeneity, and 90% high heterogeneity. A random effects model was used, and meta-analyses were performed with a 95% confidence interval (CI).
All statistical analyses were performed using the Cochrane Revman software.
Table 3 shows that there was a difference in the average ASES function before and after the intervention, indicating an improvement in function after treatment. Similarly, Table 4 also shows that there was a difference in the average pain levels before and after the intervention, indicating a reduction in pain after treatment.
DISCUSSION
This review included 12 studies,^ 17–28 ^ compiling a total of 374 whose results showed a significant reduction in pain and improvement in joint mobility of the affected shoulders after LTT surgery, the subject of this study.
Initially, the first studies conducted using this technique employed experimental designs on the hemithorax of fresh-frozen cadavers. These studies mainly investigated the biomechanics of this intervention to assess the range of motion of the shoulder joint. This provides a greater restoration of external shoulder rotation compared to the transfer of the latissimus dorsi.^30^ Moreover, the LTT determines a significant decrease in superior and anteroposterior translation. It also causes a peak of subacromial contact pressure at 0°, 30°, and 60° of shoulder abduction. The LTT efficiently prevents the loss of abduction movement and the superior migration angle of the humeral head. Therefore, we agree with the authors who argue that the LTT can sufficiently restore glenohumeral kinematics, potentially leading to better postoperative functional outcomes.
In 2016, a study conducted on 32 patients demonstrated that, after an average follow-up of 47 months, there was a significant improvement in pain, function, and range of motion of the shoulder. In patients with more than 60° of preoperative flexion, the gain in shoulder range of motion was significantly greater. External rotation improved in all patients, regardless of the loss of extension observed in the preoperative period.^ 24 ^
Overall, studies have shown good clinical and surgical results.^ 17–28 ^ In patients with a notable reduction in rotation strength, tendon transfers have the ability to restore strength while safely preserving the joint.^ 22 ^ After surgery, increases in forward flexion and external rotation are expected, as well as a reversal of the external rotation delay signal when present before surgery.^ 8 ^
We observe that with the inclusion of more studies on this topic, the surgical technique of LTT has undergone significant improvement. This has been used assistively with the aid of arthroscopy and is considered a promising option for the treatment of this condition.^ 18–20,22–26,28 ^
It is important to highlight that the transfer of the lower trapezius tendon should not be used in certain patients such as: those with arthropathy due to rotator cuff tear; combined loss of elevation and external rotation; irreparable tear of the subscapularis muscle; involvement of the teres minor muscle; and in elderly patients or those considered unable to comply with the strict rehabilitation guidelines.^ 6 ^
We highlight the sample value and observed results as relevant positive aspects of this secondary study. We cannot fail to point out some negative aspects of this systematic review where we highlight the low level of evidence of the compiled studies, with most being retrospective cohort studies. The homogeneity among the studies was not evaluated. Authors who used combinations of different surgical techniques, approaches (open versus arthroscopic), and types of grafts were excluded. Some studies presented biases when considering sample size and minimum follow-up time, which hindered the identification of more relevant considerations.
Thus, we emphasize that this interesting topic requires the pursuit of scientific work with the highest level of scientific evidence that can be achieved through randomized clinical trials and the performance of representative sample calculations.
CONCLUSION
The authors conclude that the results of the pre and postoperative evaluation of patients with irreparable rotator cuff injuries treated by the LTT technique showed:
Improvement of pain after the surgical intervention was performed. The average pain intensity was 7.1 to 2.4, as measured by the VAS. Improvement in function, as measured by the ASES system. The initial average value was 49.5 (a poor result) and subsequently improved to 78.3 (a good result).
The associated p-value indicated a statistically significant difference in pain levels before and after the intervention. The transfer of the lower trapezius is an effective therapeutic option for patients treated with the studied surgical technique, according to the results obtained.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chung SW Kim JY Kim MH Kim SH Oh JH Arthroscopic repair of massive rotator cuff tears: outcome and analysis of factors associated with healing failure or poor postoperative function Am J Sports Med 20134171674168310.1177/036354651348571923631883 · doi ↗ · pubmed ↗
- 2Ek E Cassidy J Arthroscopic-Assisted Transfer of the Lower Trapezius Tendon for Irreparable Massive Posterosuperior Rotator Cuff Tears In: Arthroscopy and Endoscopy of the Shoulder Singapore Springer 2023211218
- 3Kuan FC Shih CA Su WR Garcia AV Kuroiwa T Iida N Definition of irreparable rotator cuff tear: a scoping review of prospective surgical therapeutic trials to evaluate current practice BMC Musculoskelet Disord 202324195295210.1186/s 12891-023-07067-538066535 PMC 10704799 · doi ↗ · pubmed ↗
- 4Wagner E Elhassan B Tendon transfers for rotator cuff pathologies Current Orthopaedic Practice 2019301110.1097/BCO.0000000000000757 · doi ↗
- 5Li X Galvin JW Zalneraitis BH Gasbarro G Parada SA Eichinger JK Muscle Tendon Transfers Around the Shoulder: Diagnosis, Treatment, Surgical Techniques, and Outcomes J Bone Joint Surg Am 2022104983385010.2106/JBJS.21.0039835213452 · doi ↗ · pubmed ↗
- 6Waterman BR van der List JP Fiegen A Editorial Commentary: Lower Trapezius Transfer May Be Indicated for Surgical Management of Massive Irreparable Rotator Cuff Tears in Younger, Non-Arthritic Patients Arthroscopy 202440396096210.1016/j.arthro.2023.08.06738219138 · doi ↗ · pubmed ↗
- 7Clouette J Leroux T Shanmugaraj A Khan M Gohal C Veillette C The lower trapezius transfer: a systematic review of biomechanical data, techniques, and clinical outcomes J Shoulder Elbow Surg 20202971505151210.1016/j.jse.2019.12.01932169465 · doi ↗ · pubmed ↗
- 8de Marinis R Marigi EM Atwan Y Velasquez Garcia A Morrey ME Sanchez-Sotelo J Lower Trapezius Transfer Improves Clinical Outcomes With a Rate of Complications and Reoperations Comparable to Other Surgical Alternatives in Patients with Functionally Irreparable Rotator Cuff Tears: A Systematic Review Arthroscopy 202440395095910.1016/j.arthro.2023.06.02937394146 · doi ↗ · pubmed ↗