Sick building syndrome, multiple chemical sensitivity, and related factors: A cross-sectional analysis from the Japan Environment and Children’s Study
Yasuaki Saijo, Eiji Yoshioka, Yukihiro Sato, Hiroyuki Shiotsuki, Kentaro Nakanishi, Yasuhito Kato, Ken Nagaya, Satoru Takahashi, Yoshsiya Ito, Atsuko Ikeda, Hiroyoshi Iwata, Takeshi Yamaguchi, Reiko Kishi

TL;DR
This study explores factors linked to sick building syndrome and multiple chemical sensitivity in a large Japanese population, finding associations with allergies, mental health, and lifestyle factors.
Contribution
The study identifies demographic, lifestyle, and comorbidity factors associated with sick building syndrome and multiple chemical sensitivity in Japan using a large population sample.
Findings
Allergic diseases, psychiatric disorders, and psychological distress are strongly associated with sick building syndrome and multiple chemical sensitivity.
Higher IgE levels and autoimmune diseases are linked to increased odds of sick building syndrome and multiple chemical sensitivity in pregnant women.
Autistic traits and physical activity are associated with these conditions among pregnant women but not their partners.
Abstract
Sick building syndrome (SBS) is caused by having unhealthy indoor environments. Multiple chemical sensitivity (MCS) is a chronic condition that is potentially triggered by low-level chemical exposure. Demographic factors, lifestyle factors, and comorbidities have been reported as potential risk factors of both conditions; however, studies on these factors involving large populations in Japan are limited. The aim of this study was to investigate whether demographics, lifestyle, and comorbidities were associated with MCS and SBS in a large Japanese population, and whether autistic traits (Japanese version of the Autism-Spectrum Quotient Short Form, AQ-10-J), psychological distress (Japanese version of the Kessler 6-Item Psychological Distress Scale, K6), and serum total and allergen-specific immunoglobulin E (IgE) levels were related to the outcomes. The participants included 92,387…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
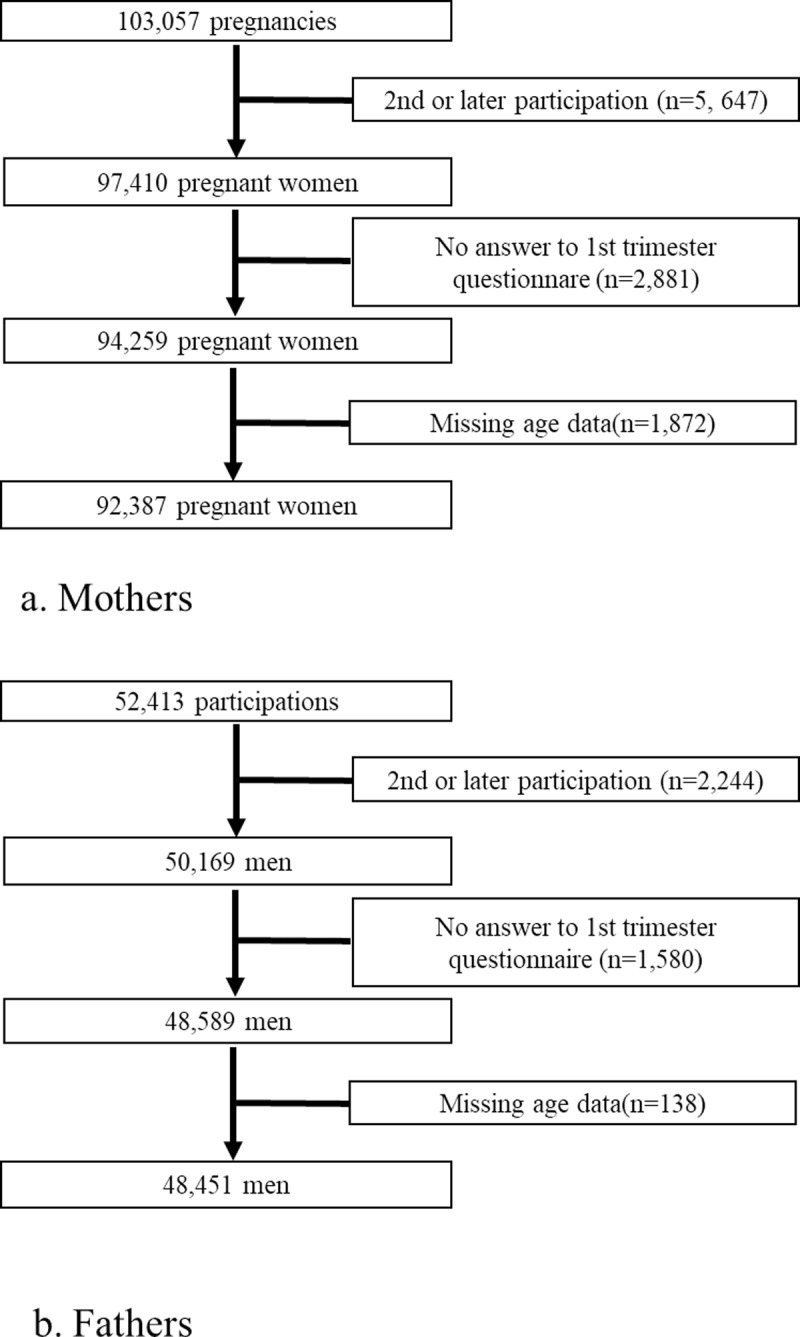 Fig 1
Fig 1- —http://dx.doi.org/10.13039/501100006120Ministry of the Environment, Government of Japan
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPediatric health and respiratory diseases · Fibromyalgia and Chronic Fatigue Syndrome Research · Urban Green Space and Health
Introduction
Sick building syndrome (SBS) is characterized by non-specific symptoms (e.g., headache, eye, nose, or throat irritations; dry cough; dry or itchy skin; dizziness) developed in specific buildings, and its cause was classified as ambient (environment)-related factors and individual-related factors [1,2]. In Japan, SBS, which occurs in home environments and is caused mainly by exposure to volatile organic compounds, has become a major environmental medical issue since the 1990s and is also called “sick house syndrome” [3,4]. Thus, SHS is a type of SBS developed at home, a term that has been used especially in Japan. Multiple chemical sensitivity (MCS), also known as idiopathic environmental intolerance, is a medical condition of unknown etiology triggered by low-level chemical exposure. They involve a large spectrum of organ systems, and the symptoms are reported to be induced by environmental chemicals at doses far below those usually harmful to most persons [5–7].
Exploring the risk factors for SBS and MCS is a developing field, and various comorbidities related to MCS, such as anxiety, depression, psychotic disorders, migraines, asthma, allergies, atopic dermatitis, autoimmune diseases, neurological diseases, gynecological diseases, and cardiopulmonary diseases, have been reported as potential risks [5,8,9]. The demographics of patients with MCS, such as being female, middle-aged, and of high socioeconomic status, have also been considered potential risks [5,10]. SBS is also related to being female, atopy, anxiety, aggressiveness, low sense of coherence, neuroticism, and working in a poor psychosocial environment [11–13]. A recent review showed that SBS and MCS share common symptoms and possibly have the same mechanisms, such as neurogenic inflammation and neural sensitization [14]. Furthermore, they sometimes overlap [3], with 60% of MCS cases in Japan developing from SHS [15]. However, to the best of our knowledge, no studies have been conducted to simultaneously investigate the comorbidities of SBS (or SHS) and MCS in the general population.
Additionally, the interplay between developmental disorders, SBS, and MCS has attracted attention, and increased incidences of autism and attention deficit hyperactivity disorder (ADHD) in children of parents with MCS have been reported [16,17]. A four-country study (the United States, Australia, Sweden, and the United Kingdom) revealed that individuals with chemical sensitivity were more likely to report autism/autism spectrum disorders (ASDs); however, statistical analysis was not performed [18]. Moreover, no report exists on whether developmental disorders are more common comorbidities in patients with SBS or MCS based on statistical analyses.
Thus, the aim of this epidemiological study was to investigate whether demographics, lifestyles, and comorbidities were associated with SBS or MCS among a relatively young child-bearing Japanese population, and to investigate whether autistic traits (Japanese version of the Autism-Spectrum Quotient short form, AQ-10-J) [19], psychological distress (the Japanese version of the Kessler 6-Item Psychological Distress Scale, K6) [20], and serum total and allergen-specific immunoglobulin E (IgE) levels were associated with SBS or MCS.
Materials and methods
Participants
This study was conducted using data from the Japan Environment and Children’s Study (JECS), an ongoing nationwide, multicenter, prospective birth cohort study. The study was conducted in 15 Regional Centres located in all geographical areas of Japan (Hokkaido, Miyagi, Fukushima, Chiba, Kanagawa, Koshin, Toyama, Aichi, Kyoto, Osaka, Hyogo, Tottori, Kochi, Fukuoka, and South Kyushu/Okinawa) [21,22]. Women at an early stage of pregnancy (103,057 pregnancies) and their partners (52,413) were recruited between January 2011 and March 2014. The total eligible numbers were confirmed, but the child coverage was estimated at approximately 45% in 2013 when recruitment was largely stabilized [22]. Written informed consent was obtained from all participants prior to data collection. After excluding pregnancies involving the same women, 97,410 unique pregnant women were included. After excluding participants with missing first-trimester questionnaire and age data, the final number of pregnant women was 92,387 (Fig 1a). After excluding second participating partners and those with missing the partner questionnaire and age data, 48,451 men were included (Fig 1b). We used the jecs-ta-20190930 dataset from the JECS, which was the JECS registry, the University Hospital Medical Information Network (UMIN) 000030786 (UMIN Clinical Trials Registry).
Flowchart of the study.
Ethics statement
The JECS protocol was reviewed and approved by the Institutional Review Board on Epidemiological Studies of the Ministry of the Environment and the Ethics Committees of all participating institutions. The JECS was conducted by the Declaration of Helsinki and other national regulations. Written informed consent was obtained from all participants.
History of SBS and MCS
A questionnaire was distributed to the enrolled pregnant women (mothers) during the first trimester (T1 questionnaire for mothers; if participation was delayed, it was distributed during the second or third trimester). Their partners were asked to complete a questionnaire during the mothers’ early pregnancy and one month after delivery. The questionnaire included queries about history of SBS and MCS, and those who answered yes were considered SBS-positive and MCS-positive, respectively.
Independent variables
The T1 questionnaire for mothers and the partner questionnaire included queries about history of allergies (bronchial asthma, allergic rhinitis or pollinosis, allergic conjunctivitis, atopic dermatitis, food allergy, drug eruption and drug allergy, contact dermatitis), depression, dysautonomia, anxiety disorder, schizophrenia, ADHD, learning disability (LD), ASD (questions about autism, Asperger’s syndrome, and pervasive developmental disorder [PDD]), other development disorders, hypertension, dyslipidemia, cardiovascular diseases, migraine, diabetes, thyroid diseases, other endocrine disorders, autoimmune diseases, digestive diseases, cancer, and kidney diseases. The questionnaire also included questions on smoking (‘never,’ ‘previously did, but quit before realizing current pregnancy,’ or ‘previously did, but quit after realizing current pregnancy/ currently smoking’) and drinking habits (‘nondrinker,’ ‘ex-drinker,’ and ‘drinker’).
T2 questionnaire was distributed to mothers during the second or third trimesters. It comprised questions about maternal and paternal educational attainment, categorized as ≤12 years (≤high school) and ≥13 years (>high school). T2 questionnaire also included questions on annual household income, categorized as ≤3.99 and ≥ 4.00 million yen.
Data on maternal height and pre-pregnancy weight were obtained from medical records transcriptions. If missing, the data were obtained from self-reports. Pre-pregnancy body mass index (BMI) was calculated as maternal pre-pregnancy weight (kg) divided by the square of maternal height (m^2^). The participants were categorized based on their pre-pregnancy BMI as follows: underweight (≤18.5 kg/m^2^), normal weight (18.5–24.9 kg/m^2^), overweight or obese (≥25.0 kg/m^2^). Father’s height and weight were either self-reported or reported by the partner.
Maternal age (≤24, 25–29, 30–34, 35–39, or ≥40 years) and parity (0 or ≥1) were transcribed from medical records. Father’s age was self-reported.
Maternal and paternal psychological distress was assessed using the Japanese version of the K6 in the T1 questionnaire [20,23], with a score ≥5 points indicating positive maternal psychological distress [24]. Maternal and paternal autistic traits were assessed using the AQ-10-J in the T2 questionnaire for mothers or the T1 questionnaire for partners, with a score ≥7 indicating high autism traits.
Maternal physical activity level before pregnancy was evaluated using the Japanese version (short and self-administered) of the International Physical Activity Questionnaire (IPAQ) in the T1 questionnaire, and physical activity level in terms of Met·min/day (metabolic equivalent of a task measured as the number of minute per day) was calculated [25–27]. Physical activity as defined in the IPAQ includes all time spent being physically active, including work-related, housework, and leisure-time activities. Physical activity was quartilized for categorical analysis. IPAQ was not administered to the partners in this cohort.
The mothers’ blood samples were obtained in the first trimester when possible, or in the second trimester if not. Serum total allergen-specific IgE titers were determined in a contract clinical laboratory using immunological assays (ImmunoCAP, Thermo Fisher Scientific, Inc., Sweden). Specific titers were detected for the following allergens: Dermatophagoides pteronyssinus (Der p 1), Japanese cedar, egg white, animal dander (from dogs, cats, guinea pigs, rats, and mice), and moth. High serum total IgE levels were defined as ≥170 IU/mL [28,29]. Positivity for allergen-specific IgE sensitization was defined as allergen-specific IgE ≥ 0.35 UA/mL [30–33]. Only total IgE levels were available to the partners in this cohort.
Statistical analysis
The variables with missing data were shown in Table 1, and 29.94% of mothers and 15.66% of partners had one or more missing values. After stratification by sex (mothers and partners), crude analyses between the abovementioned independent variables and SBS, MCS, and SBS and/or MCS were performed using Fisher’s exact test. Age-adjusted logistic regression models were used to obtain the odds ratios (ORs) of the abovementioned independent variables for SBS, MCS, and SBS and/or MCS (combined outcome, CO). Thus, independent variables were included separately in the age-adjusted logistic regression models, and if the variables had missing values, the total analyzed numbers were reduced.
Table 1: Sick building syndrome, multiple chemical sensitivity, and related factors among mothers.
Two-sided P-values <0.05 were considered statistically significant. All analyses were performed using Stata statistical software (version 18.0) for Windows (StataCorp, College Station, TX, USA).
Results
The proportions of mothers with SBS, MCS, and CO were 307 (0.33%), 128(0.14%), and 415(0.45%), respectively, while those of their partners were 85 (0.18%), 30 (0.06%), and 112 (0.23%), respectively (Tables 1 and 2).
Table 2: Sick building syndrome, multiple chemical sensitivity, and related factors among partners.
Table 3 shows adjusted ORs for SBS, MCS, and CO among mothers. Parity of one or more was associated with significantly higher ORs for all three outcomes. Compared with ‘never’, ‘previously did, but quit before realizing current pregnancy’ was associated with significantly higher ORs for MCS and CO. Allergic diseases (yes/no, and per number increase), depression, dysautonomia, anxiety disorder, schizophrenia (except for MCS because its OR was not calculable), psychiatric diseases, migraine, autoimmune diseases, digestive diseases, cancer, and kidney diseases were associated with significantly higher ORs for all three outcomes. Dyslipidemia was associated with significantly higher ORs for MCS and CO. K6 score (≥5/ < 5, and per point increase) was associated with significantly higher ORs for all three outcomes. Dichotomous AQ showed no significant results, while continuous AQ (per point increase) was associated with significantly higher ORs for all three outcomes. The highest IPAQ category was associated with significantly higher ORs for all three outcomes, while the second highest IPAQ category was associated with significantly higher ORs for MCS and CO. Per IPAQ score increase was associated with significantly higher OR for all three outcomes. Regarding total and specific IgE levels, almost all allergens were associated with significantly higher ORs for all three outcomes, except for MCS outcome analyses of Der p1, Japanese cedar, and moth IgE levels.
Table 3: Age-adjusted odds ratios of sick building syndrome, multiple chemical sensitivity, and related factors among mothers.
Table 4 shows adjusted ORs for SBS, MCS, and CO among partners. Lower educational attainment (≤high school) was associated with significantly higher ORs for SBS. Compared with ‘never’, ‘previously did, but quit after realizing current pregnancy/ currently smoking’ was associated with a significantly lower OR for MCS. Allergic diseases (yes/no, and per number increase), depression, dysautonomia (except for MCS because its OR was not calculable), anxiety disorder, schizophrenia (except for MCS because its OR was not calculable), psychiatric diseases, and migraines were associated with significantly higher ORs for all three outcomes. Digestive diseases and dyslipidemia were associated with significantly higher ORs for SBS and CO. Dichotomous K6 score was associated with significantly higher ORs for all three outcomes, whereas continuous K6 score (per point increase) was associated with significantly higher ORs for SBS and CO. Dichotomous and continuous AQ (per point increase) were associated with significantly higher ORs for MCS. Total IgE levels were associated with significantly higher ORs for SBS and CO.
Table 4: Age-adjusted odds ratio of sick building syndrome, multiple chemical sensitivity, and related factors among partners.
Discussion
This study showed that allergic diseases, psychiatric diseases, migraine, and psychological distress were related to physician-diagnosed SBS, MCS, and CO in men and women, with similar significant relationships among them. Among pregnant women, autoimmune diseases, cancer, kidney diseases, physical activity evaluated using the IPAQ, autistic traits assessed using the AQ-10-J, and total and specific IgE levels were associated with physician-diagnosed SBS, MCS, and CO. To our knowledge, this is the first study to reveal associations of various comorbidities and IgE levels with SBS and MCS in a large Japanese population, although the participants were restricted to pregnant women and their partners.
Patients with MCS may have more comorbidities of allergic diseases [34,35], as one of the proposed mechanisms of MCS development is allergic responses and alterations in the immune system [5]. A relationship between allergies and SBS has been reported [1], and the environmental factors associated with SBS development include mold, fungi, and mites, which can act as allergens [4,36]. In the allergen-specific IgE analysis among mothers, Der p1 IgE had the highest OR for MCS and egg whites had the highest OR for SBS. Because mite allergen is a sick building-related factor, having the highest OR was plausible. A Japanese web survey study revealed that food allergy was significantly related to chemical intolerance, with a higher OR than other allergic diseases [37]. However, the mechanism was unknown, and the mechanism behind egg white IgE having the highest OR for MCS was not plausible in our study. Further studies are required to explore the relationship between MCS and food allergy.
Previous studies have reported associations of comorbidities with SBS [12,38,39] and MCS [5,8,9,40]. In the present study, psychiatric diseases and psychological distress evaluated using the K6 were significantly related to all three outcomes. Although the etiology is unknown, several studies have speculated that MCS and psychiatric diseases have common risk factors [5] and that MCS is possibly caused by mental illness [41,42] and precedes the onset of mental illness [43,44]. Another possible cause of MCS is neurogenic inflammation, which causes mental illness [5,7,8]. Regarding SBS, air pollution has been reported to be associated with poor mental health [7], and one of the risk factors of SBS is psychosocial stress [13], which can cause mental illness.
Migraine is an MCS-related comorbidity [45,46], with common possible mechanisms including central sensitization, oxidative stress, and systemic inflammation [7]. SBS has also been reported to be related to migraines [47]. A reason for these significant relationships may be the overlap between the causes of SBS and migraine triggers such as ambient air pollution and volatile molecules (odorants) [48,49].
Developmental disorders showed no significant results in our study because their prevalence was low, and neither SBS- nor MCS-positive participants had developmental disorders. However, AQ point increase was associated with significantly higher ORs for all three outcomes among mothers, and AQ ‘positive’ and point increase were associated with significantly higher ORs for MCS among partners. Individuals with chemical sensitivity have been reported to be more likely to report autism/ASD [18]. Although our study did not show significant results regarding developmental disorder analyses, significant AQ results may indicate that MCS patients may have an autism spectrum tendency.
Digestive diseases were significantly associated with the outcomes, except MCS, among partners (p = 0.050). In a general Swedish and Finnish adult population study, chemical and building-related intolerance groups had significantly greater digestive symptoms [9]. Gastrointestinal symptoms are common in both MCS and SBS [14]. A review described a hypothesis that MCS development may be attributed to the sensitization of transient receptor potential (TRP) receptors (TRPV1 and TRPA1), and sensitization of TRV1 may be involved in the development of functional dyspepsia and irritable bowel syndromes, both of which are frequently comorbid with MCS [7]. Autoimmune diseases, cancer, and kidney diseases were significantly related to all three outcomes among mothers, and dyslipidemia was significantly related to MCS and CO among mothers and were significantly related to SBS and CO among partners. A previous review suggested that SBS, including MCS, is an autoimmune (autoinflammatory) syndrome induced by adjuvants. However, the mechanisms underlying these associations remain unclear, necessitating further studies.
The prevalence among mothers was higher than that among partners, as previously reported [9,11,39,50]. Regarding smoking status, ‘previously did, but quit before realizing current pregnancy’ was associated with significantly higher ORs for MCS and MCS and/or SBS among mothers, while ‘quitting previously did, but quit after realizing current pregnancy/ currently smoking’ was associated with significantly lower ORs for SBS among partners. Tobacco smoke triggers MCS symptoms, but the smoking status of patients with MCS has been inconsistent across studies [46,51]. Our results may reflect smoke-avoiding behaviors after MCS development among mothers with MCS, and the low OR of quitting during early pregnancy/still smoking among partners may make them less prone to developing environmental exposure-induced symptoms. Patients with MCS have lower levels of alcohol use and higher levels of alcohol intolerance [7]. The higher ORs for ex-drinkers among partners may reflect this tendency. Parity of one or more had a significant protective relationship with the three outcomes. This may be due to healthier mothers having more than one child. MCS has been associated with having a sedentary lifestyle [51], whereas other studies on MCS and SBS have revealed no relationship with exercise [9,39]. In our study, higher physical activity levels were associated with all three outcomes. Further studies are required to clarify whether lifestyle factors are associated with MCS and SBS.
Our study has several limitations. First, because the participants were restricted to pregnant women and their partners, they appeared healthier and younger than the general population. Second, this was a cross-sectional study; therefore, causal relationships could not be established. As previously mentioned, as psychosocial stress is a common risk factor of both SBS and mental illness [13], common risk factors may have the role for confounders. Furthermore, reverse causations should be considered that suffering diseases like MCS and SHS would cause mental illnesses. Third, MCS and SBS were physician-diagnosed and self-reported. Moreover, there are no specific medical tests to diagnose MCS and SBS; therefore, misclassification may have occurred. Furthermore, SHS and MCS are assumed to be the same among the general Japanese population [52], and they sometimes overlap [3]. A review revealed that the considerable similarities between SBS and MCS suggest the two conditions largely share the same mechanisms [14]. Therefore, “MCS and/or SHS” was defined as a significant outcome in our study. Fourth, because this study was not able to prove the etiology of SBS and MCS, and this was research to explore the various relational factors for SBS and MCS, statistical corrections for multiple comparisons were not done, and only age-adjusted OR were shown after sex-stratification. To confirm the current results, the associations must be tested in further studies. Finally, because this study data were based on a birth cohort study focusing on pregnant women, there were more women than men, and some data, such as antigen-specific IgE levels and IPAQ scores, were not available for the partners.
Conclusions
Allergic diseases, psychiatric diseases, migraine, and psychological distress were associated with SBS, MCS, and CO among both women and men, and autoimmune diseases, cancer, and kidney diseases were associated with SBS, MCS, and CO among women. Allergy and total and antigen-specific IgE levels were also correlated. Furthermore, AQ was related to the three outcomes among mothers, and MCS among partners. These results indicate possible relationships among autism traits, MCS, and SHS. Clinicians should consider common comorbid disorders when managing patients with SBS and MCS. Mothers had a higher prevalence, and higher physical activity level was related to mothers’ SBS, MCS, and CO, and parity of one or more had a protective relationship. Therefore, it is necessary to identify between protective and deteriorating lifestyles and demographic factors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ghaffarianhoseini A, Al Waer H, Omrany H, Ghaffarianhoseini A, Alalouch C, Clements-Croome D, et al. Sick building syndrome: are we doing enough?. Archit Sci Rev. 2018;61(3):99–121. doi: 10.1080/00038628.2018.1461060 · doi ↗
- 2Kishi R, Araki A. Importance of Indoor Environmental Quality on Human Health toward Achievement of the SD Gs. In: Kishi R, Norbäck D, Araki A, editors. Indoor Environmental Quality and Health Risk toward Healthier Environment for All. Singapore: Springer Singapore; 2020. p. 3–18.
- 3Ishibashi M, Tonori H, Miki T, Miyajima E, Kudo Y, Tsunoda M, et al. Classification of patients complaining of sick house syndrome and/or multiple chemical sensitivity. Tohoku J Exp Med. 2007;211(3):223–33. doi: 10.1620/tjem.211.223 17347547 · doi ↗ · pubmed ↗
- 4Saijo Y. Sick Building/House Syndrome. In: Kishi R, Norbäck D, Araki A, editors. Indoor Environmental Quality and Health Risk toward Healthier Environment for All. Singapore: Springer Singapore; 2020. p. 21–38.
- 5Zucco GM, Doty RL. Multiple Chemical Sensitivity. Brain Sci. 2021;12(1):46. doi: 10.3390/brainsci 12010046 35053790 PMC 8773480 · doi ↗ · pubmed ↗
- 6Binkley KE. Multiple Chemical Sensitivity/Idiopathic Environmental Intolerance: A Practical Approach to Diagnosis and Management. J Allergy Clin Immunol Pract. 2023;11(12):3645–9. doi: 10.1016/j.jaip.2023.08.039 37660733 · doi ↗ · pubmed ↗
- 7Molot J, Sears M, Anisman H. Multiple chemical sensitivity: It’s time to catch up to the science. Neurosci Biobehav Rev. 2023;151:105227. doi: 10.1016/j.neubiorev.2023.105227 37172924 · doi ↗ · pubmed ↗
- 8Rossi S, Pitidis A. Multiple Chemical Sensitivity: Review of the State of the Art in Epidemiology, Diagnosis, and Future Perspectives. J Occup Environ Med. 2018;60(2):138–46. doi: 10.1097/JOM.0000000000001215 29111991 PMC 5794238 · doi ↗ · pubmed ↗