Mixed-methods Study of the Effect of Chemotherapy-induced Peripheral Neuropathy SymptomPermanence on Patient’s Willingness to Alter Neurotoxic Chemotherapy Treatment
Yerial Jun, Xueting Tao, Jaeyoung Choi, Kelley M. Kidwell, Daniel L. Hertz

TL;DR
This study shows that patients are more likely to change their chemotherapy treatment if they believe the side effects will be permanent.
Contribution
The study reveals how the permanence of CIPN significantly affects patient treatment preferences using mixed-methods analysis.
Findings
CIPN permanence increased the likelihood of altering treatment by 29 times.
62% of patients continued treatment despite CIPN, but only 8% would do so if it were permanent.
Improved communication about permanent CIPN risks is needed for shared decision making.
Abstract
Chemotherapy-induced peripheral neuropathy (CIPN) is a common dose-limiting side effect from taxane and platinum chemotherapy, with symptoms that can persist for years after treatment and significantly diminish quality of life. This study aimed to evaluate how the potential permanence of CIPN influences patient preferences for continuing vs. altering neurotoxic chemotherapy. A mixed-methods approach was adopted, which included surveys and semi-structured interviews. During treatment, surveys used the EORTC QLQ-CIPN20 questionnaire to assess CIPN severity and patient preferences for continuing, altering, or discontinuing chemotherapy under hypothetical scenarios of temporary vs. permanent CIPN. Post-treatment interviews investigated patients’ perceptions of altering treatment due to temporary or permanent CIPN. Survey data from 66 participants revealed that CIPN permanence considerably…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
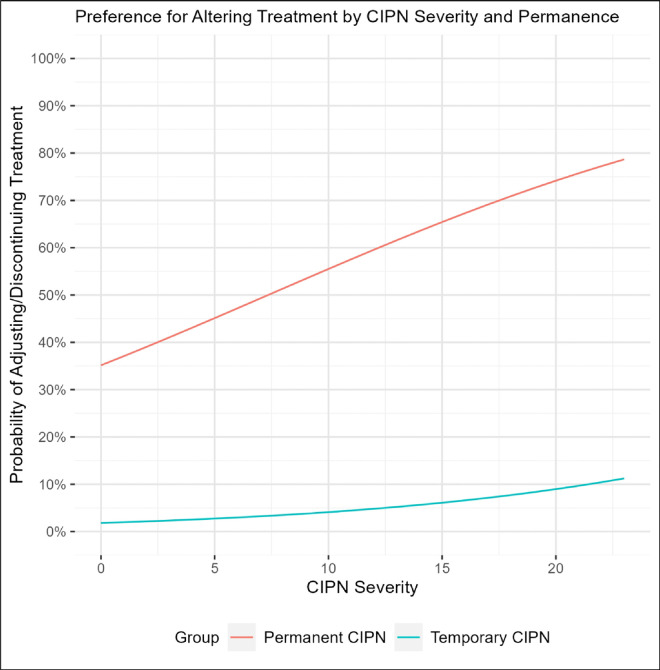 Figure 1
Figure 1- —Michigan Institute for Clinical & Health Research (MICHR)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Treatment and Pharmacology · Chemotherapy-related skin toxicity · Cancer-related cognitive impairment studies
Introduction
National Comprehensive Cancer Network Guidelines recommend treatment with neurotoxic chemotherapy including taxanes and platinums for several tumor types such as breast, colorectal, lung, and ovarian cancer [1, 2]. Although taxane treatment efficacy is well established, treatment is associated with a high rate of chemotherapy-induced peripheral neuropathy (CIPN) [19]. CIPN is characterized by numbness and tingling in the extremities that occurs in more than 50% of taxane-treated patients [16]. CIPN symptoms can improve after treatment but more than half of patients report residual symptoms more than 3 years later[10], including long-term effects on balance and stability [23] and diminished quality of life [3]. The risk of long-term CIPN may outweigh the incremental benefit of continuing taxane treatment, particularly in patients with early-stage breast cancer in whom the risk of long-term recurrence is relatively low.
The only strategy recommended in American Society of Clinical Oncology (ASCO) guidelines for prevention of further CIPN progression in patients with intolerable symptoms is to alter treatment with the offending agent by delaying, decreasing, or discontinuing its administration [14] Up to a quarter of patients receive some treatment alteration due to CIPN [11, 21]. However, prior work indicates that most taxane-treated patients are unaware of the potential long-term effects of CIPN [12] precluding informed discussion with their oncology team regarding the risks and benefits of continued treatment [20]. Including patients in the decision-making process is especially important when it involves an adverse effect that can impact their long-term function and quality of life.
In order to develop tools that can assist in structuring conversations between patients and their medical oncologist, it is critical to understand the patient’s perspective on CIPN and their preferences for being involved in the decision-making process. The purpose of this mixed-methods study was to explore patients’ acceptance of treatment alteration when experiencing CIPN and how the potential permanence of CIPN symptoms affected their preferences.
Methods
Study Design and Participants
Data collection was embedded within a prospective observational clinical study conducted for an unrelated purpose. The clinical study enrolled ambulatory patients initiating taxane and/or platinum chemotherapy for breast or colorectal cancer who had access to an iPhone[5]. The study was conducted at the University of Michigan Rogel Cancer Center and approved by the UM IRB-Med (PI: DL Hertz, HUM00171478). All participants completed written informed consent to participate.
Quantitative Data Collection via Surveys During Treatment
Surveys were completed within an iOS application (NeuroDetect Version 2.0). At the start of cycles 2, 3, and 4 of neurotoxic chemotherapy treatment, patients reported their neuropathy severity via the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ) CIPN20 patient-reported outcome questionnaire. Each item was rated on a scale from 1 (not at all) to 4 (severe) and the sum score minus 8 (the minimum possible score) was used in the analysis (scale: 0–24, higher numbers indicating more severe CIPN) [18]. Immediately after completing the CIPN assessment, patients were asked about their preferences to continue, alter or discontinue chemotherapy treatment under two hypothetical scenarios: 1) their CIPN symptoms would be temporary or 2) their CIPN symptoms would be permanent.
Qualitative Data Collection via Interviews After Treatment
Post-treatment interviews were conducted by a study team member (J.C.) to understand patient’s perspectives on altering chemotherapy treatment due to CIPN. A semi-structured interview guide was developed in conjunction with a multidisciplinary research team comprised of experts in clinical-translational CIPN (DH) and outcomes (TS) research (Appendix 1). The interview explored patient’s acceptance of treatment alteration due to CIPN and the effect of CIPN permanence on this decision. Specifically, patients were asked whether they would prefer to continue; delay the next cycle; decrease the dose; or discontinue chemotherapy if they were predicted to experience severe CIPN by the end of treatment. Participants who chose to continue with the chemotherapy without adjustment were then asked the same question under the assumption that their CIPN would be permanent. For both questions, participants’ were asked to explain the reasoning behind their preference.
At the start of each interview, the researcher obtained verbal consent from the individuals to audio record. The audio files were transcribed verbatim except for removal of all identifying information. Interview recruitment was discontinued when thematic saturation was reached.
Statistical Analysis
The primary outcome of the quantitative analysis was whether patients chose to alter treatment (i.e., delay or discontinue) vs. continue treatment as planned. The main independent variable of interest was CIPN permanence vs. not (i.e., temporary). We analyzed the odds of altering treatment via generalized linear mixed effects models with a random intercept using time as a continuous variable. We additionally controlled for CIPN severity at that time (CIPN20 score), days since start of treatment (continuous), patient’s age (continuous), chemotherapy type (taxane, platinum, or both) and metastatic cancer (vs. non-metastatic) in multivariable analyses.
Interview transcripts were reviewed, and a master codebook was created using Microsoft Excel. Each participants’ responses were coded based on the standardized questions asked during the interview. Response codes were analyzed using descriptive statistics and thematically.
Results
Patient Characteristics
A total of 66 patients were enrolled in the study of whom 55 (83%) had breast and 11 (17%) had colorectal cancer (Table 1), and most (82%) had non-metastatic cancer of either type. Neurotoxic chemotherapy regimens were primarily taxane-containing (83%) with or without platinum. The mean age of patients was 50.0 years (Standard Deviation [SD] = 13.3), and the mean duration of chemotherapy treatment was 2.46 months (SD = 1.20).
Quantitative Effect of CIPN Permanence on Chemotherapy Alteration Preference
In the primary analysis, patients were dramatically more likely to choose to alter chemotherapy treatment under the hypothetical scenario that their CIPN symptoms would be permanent compared to when symptoms would be temporary (Odds Ratio [OR] = 29.14 [95% confidence interval: 15.31–55.46], p < 0.001) after adjusting for relevant covariates (Table 2, Fig. 1). In multivariable analyses, CIPN severity, treatment duration, age, type of chemotherapy, and metastases were not associated with the odds of choosing to alter treatment (all p > 0.05).
Qualitative Analysis of Patient’s Perception on Treatment Alteration
Interviews were conducted September 2021 to September 2022. A total of 29 participants were interviewed (Female = 28, Male = 1). The interviews lasted 6 to 14 minutes with a mean duration of 10 minutes.
When asked about their willingness to alter treatment due to CIPN, 62% (n = 18) of participants wanted to continue with their current regimen (Table 3). The most common themes that emerged regarding why patients wanted to continue treatment was Prioritizing Cancer Efficacy (n = 6) and Lack of Concern Regarding CIPN (n = 6). No patients indicated they would discontinue treatment due to CIPN but 21% (n = 6) were interested in altering (i.e., decreasing or delaying) dosing and 14% (n = 4) stated they would want to discuss what to do with their provider (see example quotes in Table 3).
Twenty-four participants were then probed with a hypothetical statement that their CIPN would be permanent. Only 8% (n = 2) still wanted to continue treatment as-is, and these participants were highly motivated by Prioritizing Cancer Treatment Efficacy (Table 4). Higher percentages of patients wanted to alter treatment (50%, n = 12), discontinue treatment (13%, n = 3), and discuss with their provider (29%, n = 7). Several patients commented that the input from their provider was necessary to make this decision (see example quotes in Table 4).
Discussion
CIPN is a common dose-limiting side effect that can persist after treatment and irreversibly affect patient’s function and quality of life [3, 10, 23]. Many patients are unaware of the potential long-term impacts of CIPN when considering whether to continue, alter, or discontinue treatment [12, 20]. The primary objective of this mixed-methods study was to evaluate how the permanence of CIPN symptoms influence patients’ preferences for altering chemotherapy during their treatment. We found that the permanence of CIPN symptoms made patients significantly more likely to want to alter chemotherapy and that patients wanted to make this decision collaboratively with their medical oncologist.
This survey of patients currently undergoing neurotoxic chemotherapy found that permanence of CIPN symptoms had an extremely strong influence on their willingness to alter or discontinue chemotherapy (OR ~ 30). Similarly, post-treatment interviews support the effect of CIPN permeance on patient’s preference to alter or discontinue neurotoxic chemotherapy. These findings are consistent with prior research from our group on this topic. A previous survey of patients who had completed neurotoxic chemotherapy treatment found a dramatic decrease in the percentage of patients who would have wanted to continue chemotherapy if their CIPN would be permanent (58–34%) [12]. Additionally, a previous qualitative analysis found that informing patients about the potential for permanent CIPN affects increased their interest in adjusting or discontinuing treatment to preserve quality of life [20].
These interviews also highlighted the importance of shared-decision making when considering whether to alter treatment due to CIPN. Many patients emphasized the need for collaborative discussions with their oncologist to understand the risks of long-term side effects and the potential impact of alteration on treatment efficacy[22]. This supports previous findings that patients are interested in discussing the potential persistence of CIPN symptoms and options for altering treatment with their oncology team [20]. Shared-decision making could be an effective strategy to provide patients with the necessary understanding of the benefits and risks of continuing or altering treatment, so they can make an informed decision that will maximize their likelihood of achieving their personal treatment goals [7]. Currently, there is insufficient data to estimate a patient’s likelihood of experiencing persistent CIPN. The ~ 50% likelihood of CIPN symptoms remaining 3 + years post-treatment has been estimated primarily from large cross-sectional studies of patients many years after treatment or relatively small cohorts of patients followed longitudinally from the end of treatment[10, 15, 17]. Robust data are needed from large prospective cohorts with longitudinal CIPN assessment at the end of and for years post-treatment to understand the actual risk of persistent CIPN [10]. These risk estimates could be further personalized by identifying demographic, treatment, or genetic factors that affect the risk of CIPN persistence [10]. This data could be integrated into decision aids that provide patients with simple information about the risks of persistent CIPN and the potential benefits (reduced persistent CIPN [6]) and risks (reduced efficacy [13]) of treatment alteration [11]. Decision aids have assisted cancer patients and their clinicians with making high-quality shared-decisions in other areas with risk-benefit tradeoffs such as decisions around surgical mastectomy [4, 8, 9].
This study used a patient-centered mixed-methods approach to understand patient preferences around treatment alteration in the context of permanent CIPN. Using actual patients currently receiving treatment enhances the relevance and applicability of these findings whereas the semi-structured interviews allowed for in-depth exploration of patients’ perspectives. There are also limitations of this study that should be considered. The modest sample size, and predominance of women with early-stage breast cancer, limits the reliability of these findings and precludes subgroup analyses to further explore differences between patients or their cancer types or treatment regimens. Additionally, self-reported data can be subject to bias, as patients may provide socially desirable responses.
In conclusion, the permanence of CIPN significantly influences patients’ preferences for altering chemotherapy treatment. There is a critical need for better data to support communication between patients and their oncology teams regarding the potential long-term effects of CIPN, perhaps assisted with decision aids. Prospective trials could then be conducted investigating the effectiveness of these tools to support shared decision-making that improves patient’s likelihood of achieving their goals of chemotherapy treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Referenced from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Breast Cancer V.1.2019. © National Comprehensive Cancer Network, Inc 2019. All rights reserved. Accessed [June 27, 2019]. To view the most recent and complete version of the guideline, go online to www.nccn.org. NATIONAL COMPREHENSIVE CANCER NETWORK®, NCCN®, NCCN GUIDELINES®, and all other NCCN Content are trademarks owned by the National Comprehensive Cancer Network, Inc
- 2Referenced from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Colon Cancer V.2.2019. © National Comprehensive Cancer Network, Inc 2019. All rights reserved. Accessed [June 27, 2019]. To view the most recent and complete version of the guideline, go online to www.nccn.org. NATIONAL COMPREHENSIVE CANCER NETWORK®, NCCN®, NCCN GUIDELINES®, and all other NCCN Content are trademarks owned by the National Comprehensive Cancer Network, Inc
- 3Beijers A, Mols F, Dercksen W, Driessen C, Vreugdenhil G (2014) Chemotherapy-induced peripheral neuropathy and impact on quality of life 6 months after treatment with chemotherapy J Community Support Oncol 12: 401–40625856013 10.12788/jcso.0086 · doi ↗ · pubmed ↗
- 4Berlin NL, Tandon VJ, Hawley ST, Hamill JB, Mac Eachern MP, Lee CN, Wilkins EG (2019) Feasibility and Efficacy of Decision Aids to Improve Decision Making for Postmastectomy Breast Reconstruction: A Systematic Review and Meta-analysis Medical decision making: an international journal of the Society for Medical Decision Making 39: 5–2030799692 10.1177/0272989 X 18803879 · doi ↗ · pubmed ↗
- 5Chen C-S, Dorsch MP, Alsomairy S, Griggs JJ, Jagsi R, Sabel M, Stino A, Callaghan B, Hertz DL (2025) Remote Monitoring of Chemotherapy-Induced Peripheral Neuropathy by the Neuro Detect i OS App: Observational Cohort Study of Patients With Cancer Journal of medical Internet research 27: e 6561539908091 10.2196/65615 PMC 11840369 · doi ↗ · pubmed ↗
- 6Eckhoff L, Knoop A, Jensen MB, Ewertz M (2015) Persistence of docetaxel-induced neuropathy and impact on quality of life among breast cancer survivors Eur J Cancer 51: 292–30025541155 10.1016/j.ejca.2014.11.024 · doi ↗ · pubmed ↗
- 7Epstein RM, Street RL Jr. (2011) The values and value of patient-centered care Ann Fam Med 9: 100–103. doi: 110.1370/afm.1239.21403134 PMC 3056855 · doi ↗ · pubmed ↗
- 8Hawley ST, Griggs JJ, Hamilton AS, Graff JJ, Janz NK, Morrow M, Jagsi R, Salem B, Katz SJ (2009) Decision involvement and receipt of mastectomy among racially and ethnically diverse breast cancer patients J Natl Cancer Inst 101: 1337–134719720966 10.1093/jnci/djp 271PMC 2758308 · doi ↗ · pubmed ↗