From Learning to Policy: Adapting National Cancer Control Plans and Implementation to Africa’s Cancer Control Realities
Nwamaka Lasebikan, Annet Nakaganda, Erinma Elibe, Rebecca Erickson-Hinds, Allison Frank, Paulette Ibeka, Abdulhafiz Zakieh, Mishka K Cira

TL;DR
This paper evaluates discussions from the Africa Cancer ECHO series to identify gaps and opportunities in cancer control planning for African countries.
Contribution
The study introduces a content analysis framework to assess cancer control discussions in Africa, highlighting system-level barriers and context-specific priorities.
Findings
Diagnosis, staging, screening, service delivery, and finance were the most discussed topics in the ECHO sessions.
Task shifting emerged as a key strategy to improve healthcare access and efficiency in African cancer care.
A context-aware NCCP framework is recommended to better align with Africa's cancer control priorities.
Abstract
The Africa Cancer Research and Control ECHO (Africa Cancer ECHO) convenes cancer researchers, advocates, clinicians, policymakers, and implementers to address cancer control challenges with evidence-based approaches, to inform and respond to a country’s national cancer control planning efforts. To conduct a content analysis of the 2020–2021 Africa Cancer ECHO series, mapping discussions to NCCP core elements and identifying gaps, opportunities, and system-level barriers. A SWOT analysis of the 2020–2021 Africa Cancer ECHO series was conducted. 19 sessions were recorded, transcribed, and uploaded to Dedoose®. Each session was coded using two guiding frameworks: 1) reported strengths, weaknesses, opportunities, and threats (SWOT); and 2) domains of the Core Elements of National Cancer Control Plans (NCCP) Checklist. Also, descriptors were coded to classify session presenter…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
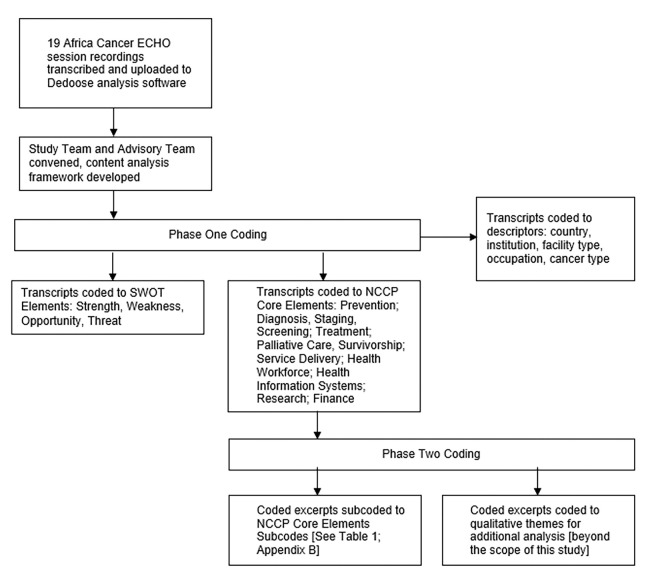 Figure 1
Figure 1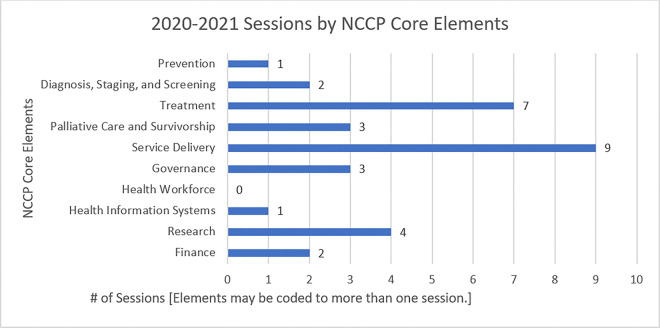 Figure 2
Figure 2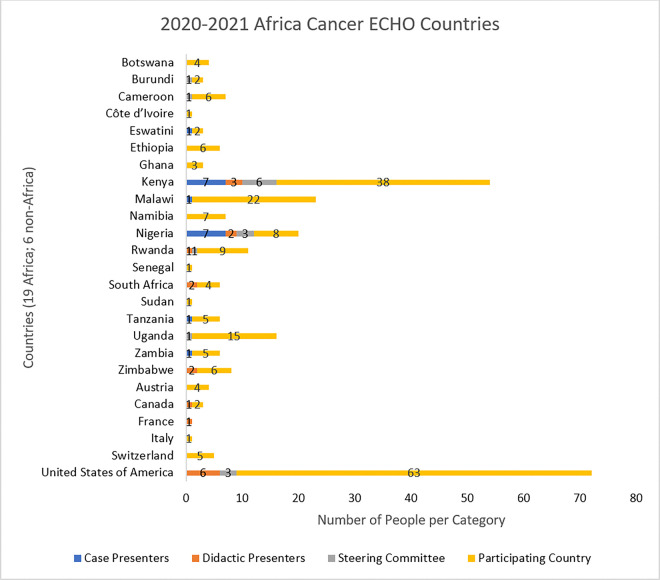 Figure 3
Figure 3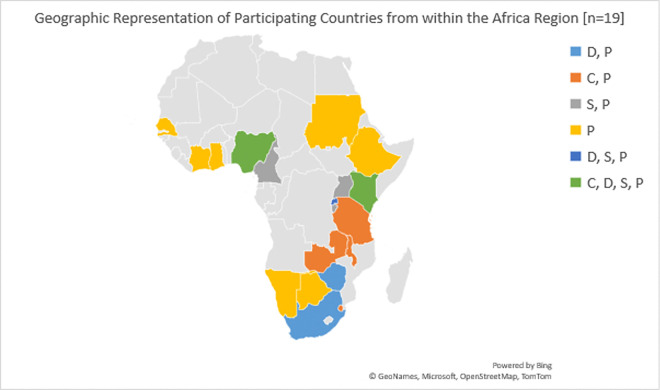 Figure 4
Figure 4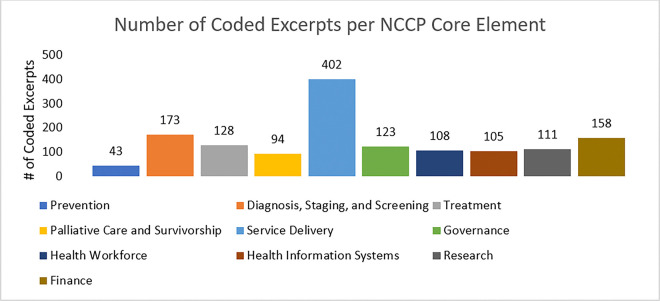 Figure 5
Figure 5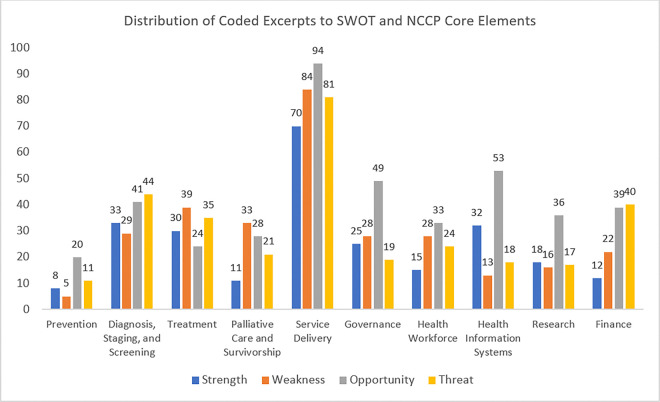 Figure 6
Figure 6- —US National Cancer Institute’s Center for Global Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Cancer Incidence and Screening · Global Public Health Policies and Epidemiology · Economic and Financial Impacts of Cancer
Introduction
The burden of cancer is growing globally, and disproportionately impacts low- and middle-income countries (LMICs). In 2020, it was estimated that the incidence of new cancer cases was 19.3 million globally, and that number is projected to rise to 28.5 million by 2040. Within the same time frame, it is estimated that there will be a 95% increase in new cancer cases in countries categorized as Low on the Human Development Index (HDI) ^1^. One of the tools available to countries to strengthen their health system response to this growing burden in a coordinated way is a National Cancer Control Plan (NCCP) that is evidence-informed and contextually relevant ^2^. An NCCP is a roadmap for countries to lay out, prioritize, and centrally coordinate locally led and implemented initiatives across the cancer continuum. When developed and implemented effectively, national cancer control plans (NCCPs) improve cancer outcomes at the population level. To aid development and evaluation of the plan, a standard reference of NCCP core elements developed by Oar et al was utilized. This is an evidence-based comprehensive checklist that provides a ready-to-use guide to support NCCP development and facilitate internal and external critical appraisal of existing NCCPs for countries.
Typically, the NCCP includes coordination of resources -technical, human, infrastructure, and financial - needed for all areas of cancer control, such as prevention, early detection, diagnosis and treatment, rehabilitation and reintegration, supportive and palliative care, survivorship, service delivery, governance, research, and surveillance ^3^. Multiple challenges in cancer control planning persist in LMICs, including mobilization of resources and collection, collation, and utilization of relevant contextual data; and the development of sustainable and innovative partnerships to implement NCCPs ^4^. Starting in 2012, the National Cancer Institute (NCI) Center for Global Health (CGH), in partnership with UN agencies, cancer centers, and global partners such as the Union for International Cancer Control, convened a series of regional cancer control leadership forums, of which there were two in the Africa region^5^. In 2018, NCI-CGH transitioned the leadership forum program to the Africa Cancer Research and Control ECHO (Africa Cancer ECHO) Program. The ECHO model utilizes an online collaborative learning approach through case-based learning to advance knowledge on a specific topic ^6^. The Africa Cancer ECHO convenes cancer researchers, advocates, clinicians, and policymakers to address topics around cancer control planning. Each session includes a ‘case’ presentation of a cancer control challenge and a ‘didactic’ presentation on evidence-based approaches to address the challenge, to inform and respond to a country’s national cancer control planning efforts.
Since 2019, a volunteer, rotating Steering Committee of multi-disciplinary cancer experts from the Africa region has led the Africa Cancer ECHO. The sessions are organized by volunteer members of the Steering Committee representing research, clinical practice, civil society, and government. Session topics are identified through an annual evaluation survey of the Africa Cancer ECHO distribution list, and past publications have covered the program evaluation of the utility of the ECHO model for advancing cancer control efforts in Africa ^7^. Program evaluation data have shown that participants reported increased self-efficacy and utilization of cancer control concepts and resources, as well as expanded networks and collaborations ^8^.
Each year, the Steering Committee conducts an evaluation survey to measure the extent to which the program achieves its goals, and in 2020, the Steering Committee conducted and published on how the Africa Cancer ECHO responded to the COVID-19 pandemic^9^.
This study aims to evaluate the content and thematic focus of the 2020–2021 Africa Cancer ECHO sessions by mapping discussions to the core elements of National Cancer Control Plans (NCCPs), to identify practical insights, implementation gaps, and system-level barriers in cancer control across African contexts. By linking session content to the NCCP framework, this analysis seeks to inform context-responsive adaptations of cancer control strategies and highlight how regional telementoring models like ECHO can serve as catalysts for policy development, capacity building, and integrated, locally driven cancer care systems.
Methods
Setting, Participants, and Procedures
Each year, members of the Africa ECHO identify specific cancer research and control topics of interest through an annual online survey. Thereafter, every Africa Cancer ECHO session was conducted and recorded using Zoom^®^. Participants in the Africa Cancer ECHO program were clinicians, people living with cancer, advocates, policy makers, researchers, and implementers from 25 countries, 19 in Africa and six countries outside of Africa with work in the region (see Fig. 3). Nineteen publicly accessible one-hour sessions were recorded from September 2020 to August 2021 [Appendix A]. Upon joining each session participants are notified that sessions are recorded and shared publicly after the session. Participants give consent to continue participating in the session. The sessions were moderated by a member of the Africa Cancer ECHO Steering Committee; questions and discussions from all participants were actively encouraged in line with the ECHO collaborative learning model. Further descriptions of the ECHO methodology have been detailed in other publications ^11^.
Data Collection and Analysis
The 19 recorded sessions were transcribed into Microsoft Word (Version 2302, Microsoft Corporation, Santa Rosa, CA, USA) for analysis. The transcribed sessions were uploaded into Dedoose^®^ (version 9.0.107; Los Angeles, CA, USA), a web-based qualitative data analysis software, which was used for coding the content of each transcript. A study advisory group was convened, including five African cancer experts through an open invitation to the Steering Committee members from 2020–2021 (TF, PI, NL, AN, CMS). A study team was convened consisting of six research fellows and staff from the US NCI/CGH (MKC, EE, TE, RE, AF, AZ).
The study team developed a content analysis framework that involved two phases (explained below). The coding protocol was established, and a practice coding session was conducted to ensure coding uniformity throughout the study. In the practice phase, the study team individually coded the same ECHO session in Dedoose. Each piece of coded text was referred to as a coded excerpt. Coding was compared by study team members to ensure inter-reviewer agreement. Once agreement was achieved, the remaining ECHO sessions were assigned to be coded by the study team (one study team member per ECHO session). The study team consulted via Zoom meetings and email for quality control and to address any questions about the data. Figure 1 shows the coding methodology used for both phases of the content analysis.
Phase One –
In phase one, excerpts were coded to identify reported strengths, weaknesses, opportunities, and threats (SWOT) about discussed topics, in relation to the core elements of National Cancer Control Plans (NCCPs)^3^: prevention; diagnosis, staging, and screening; treatment; palliative care and survivorship; service delivery; governance; health workforce; health information systems; research; and finance. The Core Elements of NCCPs can be used as a standardized tool to look at the comprehensiveness of an NCCP. This list was organized based on recommendations from the Organization for Economic Cooperation and Development (OECD) for policy makers to address cancer at a population level and was published following the 2018 global review of NCCPs as guidance to countries in national cancer control planning ^12^. Additional coding at this phase identified descriptors of the speaker and topic, such as country, institution, facility type, occupation, and cancer type. See Appendix B for the full codebook.
Phase Two –
In this phase, the NCCP core elements codes were further sub-coded into categories as outlined by Oar et al. (e.g., tobacco control and vaccination within Prevention; see Appendix B) (Table 1). During this phase, the coding team also identified qualitative themes that emerged from the coded excerpts. These qualitative themes were recorded as memos within the Dedoose software and saved for future analysis, which is outside the scope of this initial study.
Additionally, each ECHO session topic was coded to the NCCP core elements, as displayed in Fig. 2; session topics could be mapped to more than one core element. Each NCCP core element code was assigned a subcode based on categories within each core element of the NCCP core elements publication^3^.
Results
There were 19 Africa Cancer ECHO sessions [Appendix A], which were held from September 2020 to August 2021. The session case presenters came from six countries and represented six professions. The didactic presenters came from 8 countries and represented six professions. See Fig. 3 for a full list of countries represented by the Steering Committee members and session speakers. See Fig. 4 for the geographic display of case presenters, didactic presenters, and Steering Committee members by country.
The sessions identified through the annual survey of members were: pediatric cancer, prostate cancer, access to medicines, radiation therapy, clinical practice guidelines, palliative care, survivorship, patient-centeredness (patient navigation, vulnerable populations), research (patient engagement, partnerships, dissemination and implementation research), and system strengthening (mHealth and telehealth, costing strategies, integration, measuring impact).
Coding the transcripts resulted in a total of 1,547 coded excerpts. Of these, 1,446 excerpts were coded to align with the NCCP core elements, and 931 excerpts were coded to SWOT codes. The top NCCP core element coded categories were service delivery (402 coded excerpts), diagnosis, staging, screening (173 coded excerpts), and finance (158 coded excerpts).
When sessions were coded based on core NCCP elements, Service delivery had the highest numbers followed by treatment and research, representing the interest and priority of these NCCP core elements within the community.
Each NCCP core element included a set of excerpts that did not fit into the sub coded categories and there were 511 (33%) identified codes transcribed during the sessions that did not align to NCCP core elements framework currently in use that guide planning, evaluation and implementation in different countries indicating potential limitations in capturing priority areas within the region. These are listed as uncoded excerpts, and the full set of figures showing subcodes by NCCP core element is in Appendix D.
See Fig. 5 for a full breakdown of coded excerpts by NCCP core element [n = 1,446]
The top SWOT element for NCCP core elements was Opportunity, with 303 coded excerpts for Service delivery. Other opportunities were also noted in Health Information System, Governance and Finance, highlighting potential areas for development. Similarly significant weaknesses were also coded in Service Delivery, Treatment and Diagnosis, Staging and Screening, signifying gaps and challenges with these core elements noted by the community. Diagnosis, Staging, Screening, and Finance core elements had almost similar codes in opportunity and threats, signifying potential areas for development and barriers to implementation and sustainability.
For the distribution of SWOT analysis of coded excerpts of NCCP core elements, see Fig. 6.
Appendix C lists the number of coded excerpts separately by SWOT elements and NCCP core elements.
Further sub-coding of the NCCP Core elements: noted that the top subcode for Prevention core element was vaccination (Human papillomavirus (HPV), Hepatitis B virus (HBV)) with 19 coded excerpts. Cancer awareness and early detection were the highest subcodes in the Diagnosis, Screening and staging core element, while paediatric cancer, treatment guidelines, essential medicines, and multidisciplinary team care were subcoded under treatment.
Palliative workforce training, survivorship care and survivorship care plan, health workforce training, and patient navigation were most commonly coded for Palliative care and healthcare workforce. Under the Finance subcode, costing, financial resources, and financial protection for patients (financial toxicity) were the common codes seen.
And the top subcode for the Governance core element was monitoring and evaluation (21 coded excerpts). The full breakdown of the number of excerpted codes by NCCP core elements and subcodes is shown in Table 1
A few examples of text cross-coded to SWOT and NCCP core elements include:
Strength and Diagnosis, Staging, and Screening: description of the use of technology to reduce time to diagnosis.
Weakness and Service Delivery: Description of how the lack of information and knowledge among patients and caregivers leads to high mortality rates.
Opportunity and Prevention: Description of the idea of integrating scientific research with social services to reduce HIV and cervical cancer risk factors.
Threat and Health Workforce: description of the shortage of specialists in hospitals which has the potential to lead to long wait times and lack of access to care for patients.
Discussion and Conclusion
In this paper, we describe the results of a content analysis of the 19 Africa Cancer ECHO sessions held between September 2020 and August 2021. The Africa Cancer ECHO activities are designed to address key elements across the core tenets of the NCCP continuum - prevention and early detection, clinical management, cancer support services, and palliative care through non-traditional means. The Extension for Community Healthcare Outcomes (ECHO) has been validated as a model suitable for tele-mending and continuous professional development at a global scale. Despite the ongoing COVID 19 pandemic in the study period (2020–2021), participation in the ECHO remained robust.
The faculty for the year-long series was diverse, bringing expertise from across different professions, highlighting the need for multidisciplinary involvement in cancer control. Similarly, more than half of the speakers for didactic presentations were from the African continent, reflecting the importance of centering regional leadership for decisions based on solid and context-specific knowledge to address regional problems. The core elements of a National Cancer Control Plan (NCCP) include prevention and population-level driven policies, surveillance and monitoring to inform cancer control, treatment and care services, cancer management and support for people diagnosed with cancer, and integration of palliative care into the cancer plan. Our study revealed that numerous sessions focused on opportunities to reinforce crucial components of cancer control programs. While research and cancer control are the overall focus of the ECHO, the content most referenced through analysis of the coded excerpts identified diagnosis, staging, and screening, service delivery, and finance as the most discussed topic areas. These three combined NCCP core elements had significantly more focus and could represent elements with the most immediate opportunities and threats towards the continents’ cancer control efforts. The content analysis also identified systemic and structural challenges as well as resource and infrastructure limitations in coverage of key NCCP core elements, including prevention, screening, diagnosis, staging, treatment, palliative care health workforce, finance and health information systems; all of which need to be addressed to build a successful cancer control program. By mapping the session topics from the Africa Cancer ECHO series onto the cancer control continuum, we have illustrated how facets of individual discussions are connected to broader cancer control, providing a unique opportunity to explore potential linkages between various stakeholders and their activities. Additionally, the role of technology for tele mentoring has multi-sector benefits, including potentially unearthing additional linkages to strengthen cancer control efforts on the continent.
With regards to the specific NCCP core elements discussed, a key enabler and catalyst for change that was most often mentioned or discussed during the sessions is task shifting, a strategy that involves redistributing tasks among healthcare providers to maximize efficiency and improve access to care. While task shifting can help address the challenge of access to cancer care in Africa, it should be implemented within a comprehensive healthcare system that also focuses on strengthening infrastructure, increasing funding, and improving cancer surveillance and data collection^13,14^. In Rwanda task shifting has been employed to enhance breast cancer care through the integration of community health workers (CHWs) and nurses in the healthcare delivery system. The initiative involved training CHWs and nurses to perform basic breast cancer screenings, education, and referrals. This approach aimed to address the shortage of oncologists and specialized healthcare providers in the country^15^
As the continent continues to struggle with the heavy burden associated with late-stage presentation and access to diagnosis and care, more discussion points focused on prevention and early detection to identify barriers and facilitators to early detection and prompt treatment.. Unsurprisingly, vaccination against HBV and HPV was represented within the coded excerpts and correlated well with the heavy burden of malignancies associated with these infections on the continent ^16^. To address the burden of malignancies associated with HBV and HPV infections, vaccination programs against these diseases are crucial elements in cancer control efforts. In addition to vaccination, cancer control efforts should include early detection and treatment of infections that may lead to cancer, which will in turn reduce incidence, mortality, and morbidity of hepatic and cervical cancer on the continent. These important and relevant topics should be included in future Africa Cancer ECHO sessions. Due to less emphasis being placed on topics concerning prevention in 2020–2021, the Africa Cancer ECHO leadership, starting in 2022, has taken measures to ensure more equal coverage of each NCCP core element by assigning each of the ten NCCP core elements to a specific month in the series for the year.
System level challenges focusing on treatment guidelines, access to essential medicines, multidisciplinary team care, palliative workforce training, survivorship care and survivorship care plan; health workforce training and patient navigation as well as costing, financial resources and financial protection for patients (financial toxicity) are opportunities for development of innovative locally relevant, transformative and sustainable strategies that can improve the often flawed and disjointed health systems found in many African nations. ^17,18,19^
There are some examples of ongoing regional partnerships to address system-level weaknesses such as the development of context and resource appropriate guidelines ^20,21^for standardizing care, surgical oncology training led by cross-regional collaborations ^22,23^, coalition-building to address lack of access to medicines and infrastructure for safe delivery of chemotherapy ^24^, and development of sustainable train-the-trainer programs ^25,26^. Other potential strategies to address these weaknesses include investments in subspecialty education and training for healthcare professionals, as well as quality improvement programs. It is important to note that access to palliative care was recognized as a human right by the World Health Organization ^27,28^ and therefore warrants integration into national health policies and action plans. The Africa Cancer ECHO should continue to incorporate knowledge sharing about advances to address system-level weaknesses, especially those that are relevant and feasible to adapt to the diverse settings represented by session participants.
There may be a need to tailor the current NCCP core element framework to be responsive to the African context, considering that about two-thirds of the coded excerpts from phase one could not be captured with the current framework.
There were several limitations to this study. Two limitations that are beyond the control of the study team are of internet connectivity, which can sometimes be a limitation to participants, as well as competing priorities of the participants. Additional limitations specific to this study include the following: First, each transcript was coded by one reviewer, and individual interpretation and coding practices may have varied by reviewer. Second, much of the transcribed content did not fit into the SWOT framework or NCCP core elements (i.e., uncoded excerpts), which may have resulted in relevant information being omitted from our analyses. Third, while further qualitative analysis will provide insights into the types of strengths, weaknesses, opportunities, and threats in the cancer control systems in Africa, the content used for these analyses is based on the individual perspectives of the Africa Cancer ECHO participants and may not reflect broader issues and challenges. Last, the content we analyzed was based on the topics selected for the 2020–2021 Africa Cancer ECHO series and may not have represented the cancer control topics of most relevance to the whole region. While the Africa Cancer ECHO aims to reach participants from around the continent, in our current mapping, the participants came from 19 countries in the Africa region, while the case/didactic speakers came from nine countries. The Africa Cancer ECHO Steering Committee would need to consider ways to expand the diversity of representation of voices to describe country-level context from other participating countries. With a significant proportion of African countries not participating in the 2020–2021 Africa Cancer ECHO series, more should be done to understand the limitations to participation (including language barriers, access to internet, knowledge about the program, etc.). Another limitation could be time constraint due to competing work-related interests,s considering the limited skilled workforce and the heavy work burden these professionals have to contend with. Given the unique nature of this community of practice for regular dialogue in real time on issues related to cancer research and cancer control in Africa, this community should provide resources and connections needed in other countries in the region.
In conclusion, the content analysis of the 2020–2021 Africa Cancer ECHO series served as a useful evaluative tool by providing greater insight into the diversity of topical issues that the Africa Cancer ECHO session participants prioritized for discussion. Further analysis is warranted to explore what is discussed around the most frequently addressed NCCP core elements. At the same time, this analysis identified key NCCP core elements that were given less emphasis, and the limited number of countries represented through speaking roles in sessions. This information can be used to guide future session development to ensure broader inclusion of topics and geographic representation in the Africa Cancer ECHO in years to come.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H, Ferlay J, Siegel RL, : Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 71:209–249, 202133538338 10.3322/caac.21660 · doi ↗ · pubmed ↗
- 2Torode JS, Tittenbrun Z, Romero Y, : Ten Years of the International Cancer Control Partnership: Promoting National Cancer Control Plans to Shape the Health System Response for Cancer Control. JCO Glob Oncol 9:e 2200232, 202336630665 10.1200/GO.22.00232 PMC 10166518 · doi ↗ · pubmed ↗
- 3Oar A, Moraes FY, Romero Y, : Core elements of national cancer control plans: a tool to support plan development and review. Lancet Oncol 20:e 645–e 652, 201931674323 10.1016/S 1470-2045(19)30404-8 · doi ↗ · pubmed ↗
- 4Duncan K, Cira MK, Barango P, : Challenges and opportunities in the creation and implementation of cancer-control plans in Africa. Ecancermedicalscience 13:938, 201931552111 10.3332/ecancer.2019.938PMC 6722107 · doi ↗ · pubmed ↗
- 5Duncan K, Cira M, Ng’ang’a A: Use of telementoring to advance cancer control: The 2018 Africa Cancer Research and Control ECHO® Programme Cancer Control:69–74, 2019
- 6Arora S, Thornton K, Murata G, : Outcomes of treatment for hepatitis C virus infection by primary care providers. N Engl J Med 364:2199–207, 201121631316 10.1056/NEJ Moa 1009370 PMC 3820419 · doi ↗ · pubmed ↗
- 7Nakaganda A, Cira MK, Abdella K, : Expanding best practices for implementing evidence-based cancer control strategies in Africa: The 2019–2020 Africa Cancer Research and Control ECHO Program. J Cancer Policy 28:100286, 202135559915 10.1016/j.jcpo.2021.100286 · doi ↗ · pubmed ↗
- 8Lasebikan N, Nakaganda A, Fadelu T, : Demonstration of Impact Through the Evaluation of the 2020–2021 Africa Cancer Research and Control ECHO. JCO Global Oncology 8:37–37, 2022