Atypical Overlap Presentation in Guillain-Barré Syndrome: Lessons From a Case Report
Arpita Sharma, Saurabh Singhal, Vishal Vishnoi, Yashendra Sethi

TL;DR
A case of a rare overlap syndrome involving Guillain-Barré, Miller Fisher, and Bickerstaff brainstem encephalitis is reported, highlighting diagnostic challenges and treatment outcomes.
Contribution
This case report adds to the understanding of atypical GBS presentations by describing a rare overlap syndrome and its management.
Findings
The patient exhibited a rapidly progressing combination of symptoms consistent with GBS-MFS-BBE overlap syndrome.
Treatment with IVIG led to gradual neurological recovery despite initial respiratory failure.
The case underscores the importance of early diagnosis and immunotherapy in managing atypical GBS presentations.
Abstract
Guillain-Barré syndrome (GBS) is an acute, immune-mediated polyradiculoneuropathy characterized by rapidly progressive limb weakness and areflexia. While the classical form is well-recognized, variants such as Miller Fisher syndrome (MFS) and Bickerstaff brainstem encephalitis (BBE) also exist, each with distinct clinical features. Rarely, these syndromes may present in combination, forming GBS-MFS-BBE overlap syndromes. These atypical presentations pose significant diagnostic challenges that may delay the initiation of appropriate treatment. We report the case of a 60-year-old male who initially presented with pain and weakness of the left upper limb, which progressed rapidly over 72 hours to symmetrical quadriplegia, bulbar dysfunction (including dysphagia and dysarthria), complete ophthalmoplegia, and altered sensorium suggestive of encephalopathy. Neurological examination revealed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
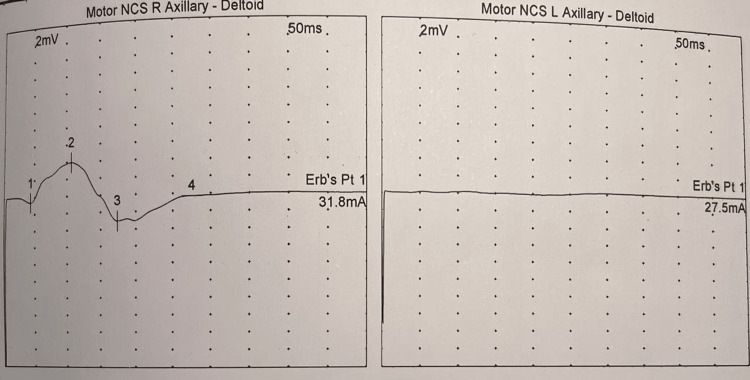 Figure 1
Figure 1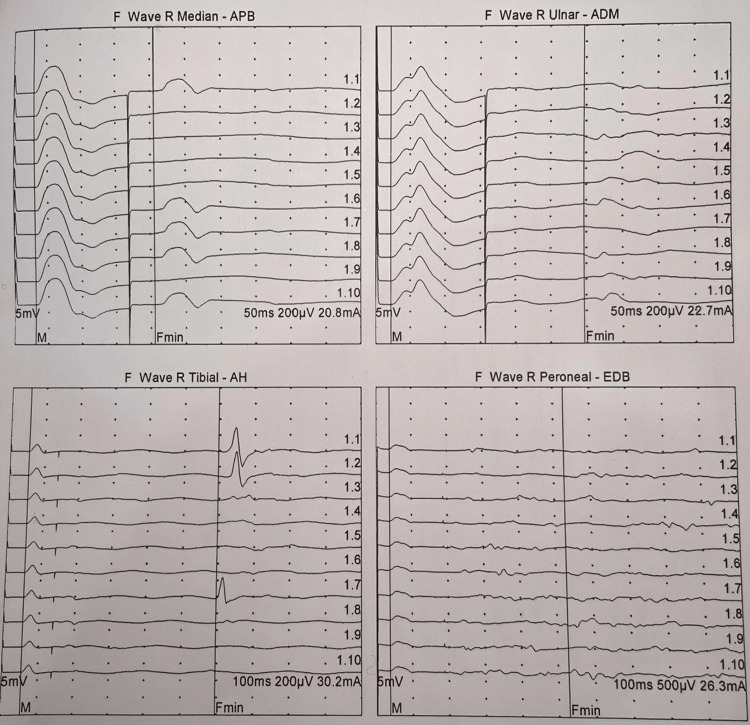 Figure 2
Figure 2| Test | Result | Normal reference range |
| ESR | 34 mm/hr | 0–9 mm/hr |
| Hemoglobin | 12.7 g/dL | 13–18 g/dL |
| Total WBC count | 9,300 /µL | 4,000–10,000 /µL |
| PCV | 38.1% | 41–51% |
| MCV | 87.79 fL | 80–97 fL |
| Platelet count | 138 × 10³/µL | 150–450 × 10³/µL |
| Neutrophils | 75% | 40–70% |
| Lymphocytes | 19% | 20–40% |
| PT | 21 seconds | Control: 14 seconds |
| INR | 1.56 | 1.1 |
| HbA1c | 6.8% | 4.2–6.2% |
| CRP | 4.6 mg/L | Normal: <6.0 mg/L |
| Rheumatoid factor | 11.3 IU/mL | Normal: <20 IU/mL |
| Total bilirubin | 2.1 mg/dL | 0–0.1 mg/dL |
| Direct bilirubin | 0.97 mg/dL | 0–0.3 mg/dL |
| Indirect bilirubin | 1.13 mg/dL | 1.1–1.35 mg/dL |
| ALP | 130 IU/L | 53–128 IU/L |
| Serum ammonia | 112 µmol/L | 12–98 µmol/L |
| Blood urea | 37 mg/dL | 6–44 mg/dL |
| Serum calcium (total) | 9 mg/dL | 8.4–10.4 mg/dL |
| Serum calcium (ionic) | 1.04 mmol/L | 1.1–1.35 mmol/L |
| Serum creatinine | 1 mg% | 0.9–1.2 mg% |
| CPK | 254 IU/L | 24–1950 IU/L |
| GGT | 24 IU/L | 0–45 IU/L |
| LDH | 120 U/L | 80–285 U/L |
| Serum total proteins | 7.1 g/dL | 6–8 g/dL |
| Serum albumin | 3.4 g/dL | 3.5–5.2 g/dL |
| Serum globulin | 3.7 g/dL | 2.3–3.5 g/dL |
| AST | 68 IU/L | 10–50 IU/L |
| ALT | 74 IU/L | 10–50 IU/L |
| Serum uric acid | 7.1 mg/dL | 3.4–7 mg/dL |
| Serum potassium | 3.6 mEq/L | 3.5–5.5 mEq/L |
| Vitamin D3 assay | 69.4 nmol/L | 75–250 nmol/L |
| Dengue NS1 antigen | Negative | – |
| Typhidot | Negative | – |
| Card test for malaria | Negative | – |
| ABG | Normal | – |
| Urine routine | Normal | – |
| Hospital day | Clinical features | Diagnostic findings | Interventions |
| Day 1 | Left arm weakness (MRC 3/5) | NCS: left axillary nerve CMAP ↓ (3.2 mV) | Analgesics, monitoring |
| Day 2 | Right arm weakness (MRC 4/5) | - | Neurology consult |
| Day 3 | Quadriparesis, dysphagia, respiratory failure | NCS: demyelination (prolonged latencies, absent F-waves); CSF: albuminocytologic dissociation | IVIG initiated, intubation |
| Day 4 | Ophthalmoplegia | Anti-GQ1b Ab (+) | Continued IVIG |
| Day 5 | Encephalopathy (GCS 8/15) | MRI brain: Normal | EEG (ruled out seizures) |
| Day 15 | Return of eye movements | - | Tracheostomy |
| Day 25 | Ventilator weaned | NCS: partial improvement | Aggressive rehab |
| Day 30 | Discharged (MRC 3/5) | - | Outpatient follow-up |
| Clinical feature | GBS mimics | Distinguishing clues | Confirmatory tests |
| Asymmetric limb weakness | Cervical radiculopathy | No sensory level, progression to areflexia | NCS (demyelination), CSF analysis |
| Brachial plexopathy | Rapid bilateral spread, bulbar involvement | Serial NCS | |
| Ophthalmoplegia + encephalopathy | Brainstem stroke | Absent DWI changes on MRI | MRI, anti-GQ1b Ab |
| Myasthenia gravis | Fatigability, response to edrophonium | Repetitive nerve stimulation | |
| Quadriparesis + respiratory failure | Botulism | Pupillary dilation, descending paralysis | Stool toxin assay |
| Therapeutic option | Mechanism | Considerations for overlap syndromes |
| IVIG (2 g/kg over 5 days) | Neutralizes autoantibodies | Preferred in hemodynamic instability |
| Plasma exchange | Removes pathogenic antibodies | Avoid in autonomic dysfunction |
| Eculizumab (anti-C5) | Complement inhibition | Reserved for anti-GQ1b+ refractory cases |
| Corticosteroids | Immunosuppression | Not recommended |
| Supportive care (ventilation) | Prevents complications | Early tracheostomy if prolonged intubation |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Neuropathies and Disorders · Hereditary Neurological Disorders · Nerve injury and regeneration
Introduction
Guillain-Barré syndrome (GBS) represents the most common cause of acute flaccid paralysis worldwide, with an annual incidence of 0.8-1.9 cases per 100,000 population [1]. The classic form, acute inflammatory demyelinating polyradiculoneuropathy (AIDP), accounts for approximately 90% of cases in Western countries, while axonal variants predominate in Asia. The annual incidence of GBS in India is reported to be around 1-2 per 100,000 people [2]. The syndrome typically manifests one to three weeks following a respiratory or gastrointestinal infection, with Campylobacter jejuni being the most frequently identified trigger [3]. Molecular mimicry between microbial antigens and neural components leads to the production of anti-ganglioside antibodies, which mediate nerve injury through complement activation and macrophage infiltration [4].
While the majority of patients present with symmetrical ascending weakness and hyporeflexia, several clinical variants have been described. Miller Fisher syndrome (MFS), characterized by the triad of ophthalmoplegia, ataxia, and areflexia, accounts for approximately 5% of cases in Western populations. However, it is more prevalent in Southeast Asia countries like India, where it accounts for 19% to 25% of GBS cases [5]. Bickerstaff brainstem encephalitis (BBE) shares clinical features with MFS but additionally includes impaired consciousness [6]. Pharyngeal-cervical-brachial weakness represents another regional variant that may mimic brainstem pathology [7]. Cerebrospinal fluid (CSF) analysis and anti-GQ1b IgG antibody testing are important in diagnosing GBS and its variants, particularly MFS. CSF analysis helps identify albuminocytological dissociation (elevated protein with normal cell count), while anti-GQ1b IgG antibodies are highly sensitive in MFS, aiding in its diagnosis, and can also be present in other GBS variants [5-7]. These atypical presentations frequently lead to diagnostic delays, particularly when they occur in combination as overlap syndromes.
We present a diagnostically challenging case of GBS that initially manifested as isolated upper limb weakness before progressing to a severe overlap syndrome encompassing features of AIDP, MFS, and BBE. This case highlights the importance of considering atypical presentations of GBS, the value of serial electrophysiological studies, and the need for prompt immunotherapy to optimize outcomes.
Case presentation
A previously healthy 60-year-old male presented to our emergency department with a 24-hour history of severe left shoulder pain and progressive weakness of the left upper limb. He reported no recent febrile illnesses, vaccinations, or trauma. On initial examination, the patient was afebrile with normal vital signs. Neurological assessment revealed Medical Research Council (MRC) grade 3/5 strength in the left deltoid and biceps muscles, with preserved strength in all other muscle groups. Deep tendon reflexes were diminished at the left biceps and brachioradialis but otherwise normal. Sensory examination was unremarkable, and cranial nerves were intact.
Initial nerve conduction studies performed on day 1 demonstrated reduced compound muscle action potential (CMAP) amplitude (3.2 mV) in the left axillary nerve with normal sensory nerve action potentials, suggesting a possible axonal brachial plexopathy (Figures 1, 2). However, the clinical picture evolved dramatically over the subsequent 48 hours. By hospital day 2, the patient developed weakness in the right upper limb (MRC grade 4/5), and on day 3, he progressed to quadriparesis with involvement of both lower extremities (MRC grade 2-3/5). Concurrently, he developed dysphagia and dysarthria, necessitating repeat electrophysiological evaluation.
Initial motor NCS demonstrating axillary nerve involvement(A) Right axillary nerve study recording from the deltoid shows reduced CMAP amplitude (2 mV) with normal latency (50 ms) and elevated stimulation current at Erb's point (31.8 mA). (B) Left axillary nerve reveals similar findings (CMAP 2 mV, latency 50 ms, Erb's point stimulation 27.5 mA). These findings initially suggested bilateral axonal plexopathy before progression to generalized demyelination.CAMP, compound muscle action potential; NCS, nerve conduction studies
Serial F-wave studies demonstrating demyelinating features(A-D) F-wave studies performed on day 3 show absent/minimal F-waves (Fmin) in right median nerve (recording abductor pollicis brevis, stimulation 20.8 mA), right ulnar nerve (recording abductor digiti minimi, stimulation 22.7 ma), right tibial nerve (recording abductor hallucis, stimulation 30.2 mA), and right peroneal nerve (recording extensor digitorum brevis, stimulation 26.3 mA).The widespread absence of F-waves with normal CMAP amplitudes confirms acute inflammatory demyelination.CAMP, compound muscle action potential
The follow-up nerve conduction studies on day 3 revealed characteristic features of acute inflammatory demyelinating polyneuropathy, including prolonged distal latencies (median nerve: 6.8 ms), conduction block (40% reduction in CMAP amplitude), and absent F-waves. CSF analysis showed albuminocytologic dissociation with elevated protein (120 mg/dL) and normal white cell count (2 cells/μL). The patient's condition continued to deteriorate, culminating in flaccid quadriplegia (MRC grade 0/5) and respiratory failure requiring mechanical ventilation by the evening of day 3.
On day 4, the patient developed complete external ophthalmoplegia with preserved vertical eye movements. Anti-GQ1b antibodies returned positive, supporting a diagnosis of MFS. By day 5, he exhibited progressive encephalopathy with a Glasgow Coma Scale score of 8/15, consistent with BBE. The composite clinical picture fulfilled the diagnostic criteria for an overlap syndrome combining AIDP, MFS, and BBE. All investigations done are summarized in Table 1.
Treatment with intravenous immunoglobulin ([IVIG] 0.4 g/kg/day for 5 days) was initiated on day 3. The patient underwent tracheostomy on day 20 due to prolonged ventilator dependence. Gradual neurological improvement began on day 15, with return of spontaneous eye movements followed by recovery of consciousness. He was successfully weaned from mechanical ventilation by day 25 and transferred to the general ward on day 27. At discharge on day 30, the patient had recovered to MRC grade 3/5 strength in all limbs with intact cognition. The patient’s clinical course, summarized in Table 2, illustrates the rapid progression from focal weakness to quadriplegia and brainstem involvement.
Discussion
This case illustrates several clinically important aspects of GBS and its variant forms. The initial presentation with isolated unilateral upper limb weakness represents an exceptionally rare manifestation of GBS, occurring in less than 5% of cases [8]. Such atypical presentations frequently lead to misdiagnosis, particularly when early electrophysiological studies suggest focal pathology. Our patient's serial nerve conduction studies demonstrate the dynamic nature of GBS, with initial findings mimicking axonal plexopathy that subsequently evolved to show definitive demyelinating features. This underlines the importance of repeating electrophysiological studies when clinical suspicion for GBS remains high despite inconclusive initial results [9]. As highlighted in Table 3, the differential diagnosis for atypical GBS includes compressive neuropathies, brainstem ischemia, and neuromuscular junction disorders.
The development of ophthalmoplegia and encephalopathy in our patient highlights the spectrum of anti-GQ1b antibody-associated disorders. These antibodies, which target gangliosides concentrated in the oculomotor nerves and brainstem, are present in more than 90% of MFS cases and approximately two-thirds of BBE cases [10]. The clinical distinction between these syndromes has become increasingly blurred, with many experts considering them part of a continuous spectrum rather than distinct entities [11]. Our case supports this conceptual framework, demonstrating a clear overlap between what have traditionally been classified as separate disorders.
Therapeutic decision-making in overlap syndromes presents unique challenges. While both IVIG and plasma exchange have demonstrated efficacy in classic GBS, data specific to overlap variants remain limited [12]. Therapeutic approaches for overlap syndromes, summarized in Table 4, prioritize IVIG but may incorporate emerging therapies in refractory cases. The presence of brainstem involvement in our patient raised theoretical concerns about autonomic instability during plasma exchange, leading to the selection of IVIG as first-line therapy. Emerging treatments such as eculizumab, a monoclonal antibody targeting complement protein C5, have shown promise in refractory cases and may be particularly relevant in anti-GQ1b-positive patients given the complement-mediated pathogenesis; however, these newer drugs will still take time to become the standard of care [13].
Prognostically, overlap syndromes typically follow a more protracted course than classic GBS. While most patients eventually achieve good functional recovery, the median time to independent ambulation may extend to six months compared with three months in typical cases [14]. Our patient's relatively rapid weaning from mechanical ventilation (25 days) compares favorably with published data on ventilated GBS patients, who average 35 days of respiratory support [15]. This may reflect the benefits of early immunotherapy initiation in our case.
Conclusions
This case report describes an unusual presentation of GBS featuring an overlap between acute inflammatory demyelinating polyneuropathy, MFS, and BBE. The patient's initial manifestation as isolated unilateral upper limb weakness, followed by rapid progression to quadriplegia, respiratory failure, and brainstem dysfunction, underscores the diagnostic challenges posed by atypical GBS variants. Serial electrophysiological studies proved essential in establishing the correct diagnosis, while prompt immunotherapy likely contributed to the favorable outcome. Clinicians should maintain a high index of suspicion for GBS even in cases with unusual initial presentations, particularly when neurological deficits progress rapidly or involve multiple anatomical regions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Guillain-Barré syndrome: pathogenesis, diagnosis, treatment and prognosis Nat Rev Neurol van den Berg B Walgaard C Drenthen J Fokke C Jacobs BC van Doorn PA 4694821020142502334010.1038/nrneurol.2014.121 · doi ↗ · pubmed ↗
- 2Guillain-Barré syndrome Lancet Willison HJ Jacobs BC van Doorn PA 71772738820162694843510.1016/S 0140-6736(16)00339-1 · doi ↗ · pubmed ↗
- 3Quantifying the association between Campylobacter infection and Guillain-Barré syndrome: a systematic review J Health Popul Nutr Poropatich KO Walker CL Black RE 5455522820102126119910.3329/jhpn.v 28i 6.6602 PMC 2995022 · doi ↗ · pubmed ↗
- 4Guillain-Barré syndrome: expanding the concept of molecular mimicry Trends Immunol Laman JD Huizinga R Boons GJ Jacobs BC 2963084320223525627610.1016/j.it.2022.02.003PMC 9016725 · doi ↗ · pubmed ↗
- 5Miller Fisher syndrome: an updated narrative review Front Neurol Noioso CM Bevilacqua L Acerra GM 12507741420233769376110.3389/fneur.2023.1250774 PMC 10484709 · doi ↗ · pubmed ↗
- 6Bickerstaff brainstem encephalitis with isolated acute bilateral ophthalmoplegia: an unusual presentation Ann Indian Acad Neurol Bagaria AK Vyas A Mathur V Ranawat CS Singh M 6246262420213472897610.4103/aian.AIAN_823_20PMC 8513979 · doi ↗ · pubmed ↗
- 7Pharyngeal-cervical-brachial variant of Guillain-Barre syndrome J Neurol Neurosurg Psychiatry Wakerley BR Yuki N 3393448520142380423710.1136/jnnp-2013-305397 · doi ↗ · pubmed ↗
- 8Diagnosis of Guillain-Barré syndrome and validation of Brighton criteria Brain Fokke C van den Berg B Drenthen J Walgaard C van Doorn PA Jacobs BC 334313720142416327510.1093/brain/awt 285 · doi ↗ · pubmed ↗