Mycobacterium heraklionense hand tenosynovitis—a case description of a three-year treatment course and perioperative measurement of azithromycin target tissue concentrations
Mads Kristian Duborg Mikkelsen, Andrea René Jørgensen, Victor Naestholt Dahl, Christian Morberg Wejse, Mats Bue, Maiken Stilling

TL;DR
A case study shows high local azithromycin concentrations in treating Mycobacterium heraklionense tenosynovitis, but bead removal was needed due to drainage.
Contribution
Demonstrates that local azithromycin delivery achieves much higher target tissue concentrations than systemic administration.
Findings
Azithromycin-loaded beads achieved over 100-fold higher local concentrations than systemic treatment.
Beads caused excessive wound drainage requiring surgical removal.
Local antibiotic administration may reduce bacterial burden but needs further study.
Abstract
In a Mycobacterium heraklionense tenosynovitis case, we observed that azithromycin-loaded calcium sulfate beads placed in the surgical wound had minimal systemic absorption and achieved over 100-fold higher target tissue concentrations than a systemic azithromycin-based treatment regimen alone. However, continued excessive wound drainage necessitated surgical removal of the beads. While systemic antibiotics and surgery remain central to nontuberculous mycobacterial treatment, the role of local antibiotic administration in reducing the bacterial burden warrants further investigation.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
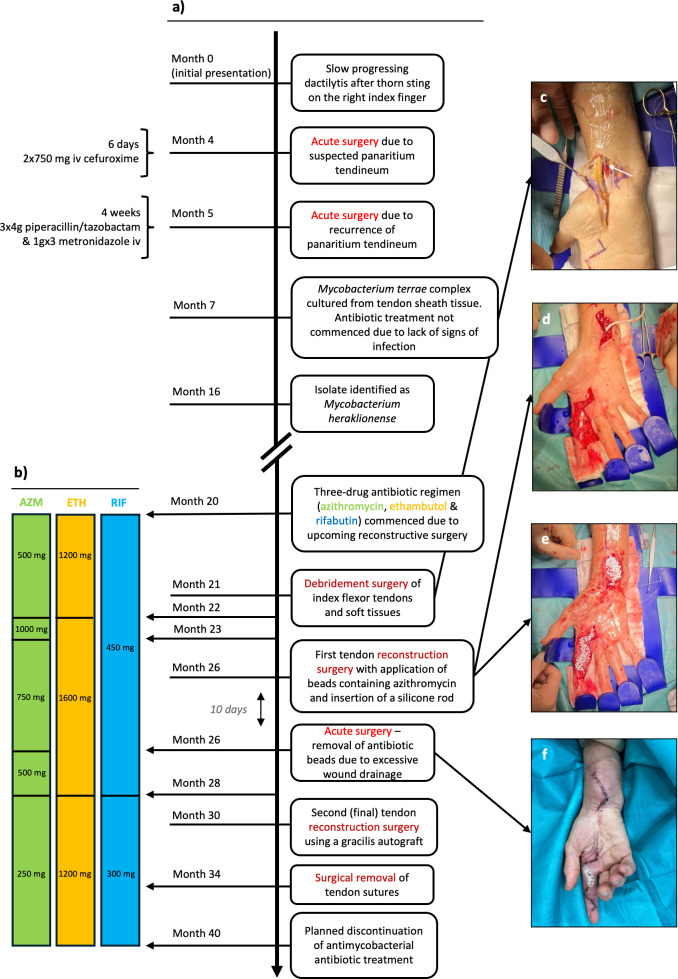 Fig 1
Fig 1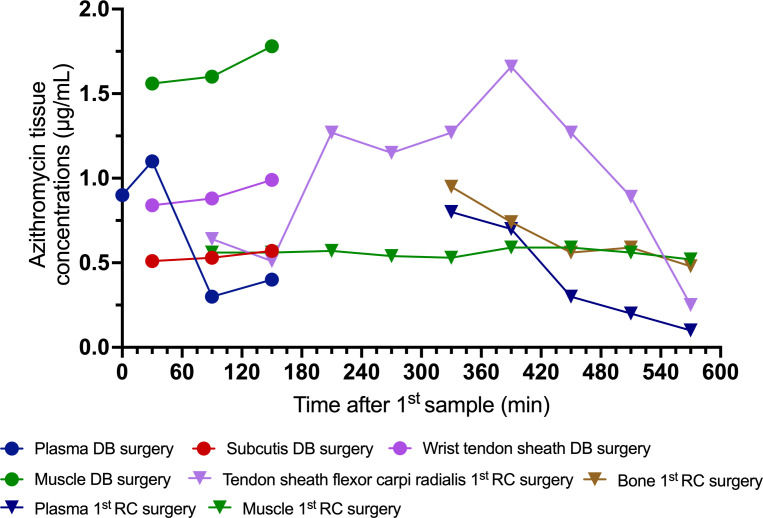 Fig 2
Fig 2| Drug | Minimal inhibitory concentrations, µg/mL | Interpretation |
|---|---|---|
| Amikacin | 16 | R |
| Clarithromycin | 8 | S |
| Ethambutol | 5 | S |
| Levofloxacin | 2 | R |
| Moxifloxacin | 1 | R |
| Linezolid | 16 | R |
| Rifabutin | 0.5 | S |
| Rifampicin | 1 | R |
- —A.P. Møller Fonden | Fonden til Lægevidenskabens Fremme (A.P. Møller Fonden til Lægevidenskabens Fremme)
- —Eva Merete Falck Crones Fond (Eva Merete Falck Crones Foundation)
- —Novo Nordisk Fondenhttp://dx.doi.org/10.13039/501100009708
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMycobacterium research and diagnosis · Infectious Diseases and Tuberculosis · Tuberculosis Research and Epidemiology
INTRODUCTION
Extrapulmonary nontuberculous mycobacterial (NTM) infections are notoriously difficult to treat, and in recent years, NTM hand infections have received increasing attention (1). Mycobacterium heraklionense, a member of the M. terrae complex, was first described by Tortoli et al. in 2013 (2). Since then, multiple hand infection cases have been documented, with a predominance of tenosynovitis (3). Azithromycin is a cornerstone in treating several NTM species; however, little is known about the relationship between azithromycin plasma and tissue concentrations and the therapeutic effect. In the following section, we present the case of an immunocompetent female in her mid-60s undergoing treatment for M. heraklionense hand tenosynovitis, focusing on perioperative azithromycin target tissue concentrations.
CASE PRESENTATION
A female in her mid-60s without any relevant medical history, aside from small joint hand osteoarthritis, presented to her local clinic with slowly progressing swelling and soreness of the right index finger (Fig. 1a). Suspectedly, this was caused by a thorn prick from a barberry bush. Four months later, her symptoms had worsened, with intense pain, paresthesia, and marked swelling of the finger, though no systemic signs of infection were present. Acute surgery was performed for suspected infectious tenosynovitis, which involved debridement of infected and necrotic tissue alongside median nerve decompression. Perioperative biopsy samples from the tendon sheath, pulley, and subcutaneous tissue were negative on routine bacterial cultures. One month later, symptoms returned, prompting another acute surgery, which revealed deposits of pus between the tendon floor and the bone, along with pulley destruction and massive tendon sheath granulation (5 mm thick). No rice body formation was observed. Extensive debridement of infected and necrotic tissue was performed, and histopathological examination of tissue biopsies from the tendon sheath and pulleys demonstrated necrotizing granulomatous inflammation but no acid-fast bacilli (Ziehl–Neelsen staining). After acute surgery, symptoms of infection quickly resolved. Paresthesia of the index finger persisted, and bowstringing of the flexor tendons with adhesion developed. Seven months after clinical presentation, mycobacterial cultures from the tissue biopsies in the first surgery grew a few colonies of M. terrae complex. Auramine–rhodamine fluorochrome staining was negative. Antimycobacterial treatment was not commenced due to the absence of clinical signs of infection and seemingly spontaneous improvement.
Case timeline with clinical images during the treatment. (a) Timeline of disease progression and surgical interventions. (b) Timeline of antimycobacterial treatment, with administered daily doses. (c) Placement of a microdialysis catheter (white arrow) in the subcutaneous tissue of the distal forearm during debridement surgery. (d) Placement of a silicone rod during the first reconstructive surgery. (e) Application of azithromycin-containing beads in the distal forearm and index finger during the first reconstructive surgery. (f) Inflamed wound with persistent drainage 10 days after implantation of the azithromycin-containing beads. AZM, azithromycin; ETH, ethambutol; RIF, rifabutin.
Sixteen months after the initial presentation, the International Reference Laboratory of Mycobacteriology in Copenhagen identified M. heraklionense as the causative species from the earlier cultured isolate using whole-genome sequencing. Two months later, drug susceptibility testing results were available (Table 1). A two-stage tendon reconstructive surgery was planned to address bowstringing of the flexor tendons and tendon adhesion.
CHALLENGE QUESTION
What is the optimal antibiotic treatment duration for hand tenosynovitis caused by an NTM infection when a foreign body has been inserted?
(A) The presence of a foreign body should not influence treatment duration, and a 6-month treatment is sufficient.
(B) Caution is warranted due to the presence of a foreign body. A treatment duration of more than 1 year after insertion is preferable, while 3-6 months may be sufficient if the foreign body is removed.
(C) The treatment regimen should be guided by the clinical course and discontinued only when there is a clinical conviction of cure.
(D) Option C, but additional local therapies (e.g., surgery, negative pressure wound therapy with instillation and dwell time with topical antibiotics (NPWTi-d), antibiotic-loaded beads) should be considered to improve infection control and potentially shorten the treatment duration.
TREATMENT AND OUTCOME
The treatment regimen and duration were discussed at a multinational, multidisciplinary meeting (4). Based on this, a combination regimen of azithromycin, rifabutin, and ethambutol, initiated one month before tendon reconstruction surgery, was recommended to continue for 6 months after the final surgical intervention (Fig. 1b). Antibiotic dosing was guided by therapeutic drug monitoring in plasma, leading to dose adjustments throughout treatment.
After 21 months, surgery revealed massive tendon adhesion and yellow low-viscosity pus-like deposits in the tendon–bone interface. Thorough debridement was performed, including excision of the flexor tendon and median nerve decompression. Intraoperatively, microdialysis catheters were placed (Fig. 1c) in the flexor carpi radialis tendon sheath, the brachioradial muscle, and forearm subcutaneous tissue to enable postoperative sampling (3 hours) of steady-state azithromycin concentrations in target tissues. Biopsies from the tendon, pus-like deposits, and bone were sent for routine bacterial and mycobacterial culturing but showed no bacterial growth.
The first-stage tendon reconstruction was performed 26 months after the initial presentation, with implantation of a silicone rod (Hunter I) (Fig. 1d). Given the risk of biofilm formation due to the presence of a foreign body in a formerly infected wound, 3 cc of antibiotic calcium sulfate beads (STIMULAN Rapid Cure; Biocomposites, UK) prepared with 300 mg of azithromycin was placed around the silicone rod (Fig. 1e). Microdialysis catheters were positioned along the silicone rod in the index finger and above the wrist, as well as in the flexor carpi radialis tendon sheath, the brachioradialis muscle, the forearm subcutaneous tissue, and the radius cancellous bone for postoperative sampling (10 hours) of steady-state azithromycin concentrations. However, continuous wound drainage necessitated surgical removal of the beads 10 days after implantation (Fig. 1f).
The second-stage flexor digitorum profundus tendon reconstruction was performed after 30 months using a gracilis tendon autograft. Eleven months after the final reconstructive surgery, the patient showed no signs of infection.
Methods
Microdialysis was used to sample local unbound (free) steady-state azithromycin concentrations in target tissues (5). Plasma samples were collected at the midpoint of each sampling interval. Microdialysis catheters type 70 with 20 mm and 10 mm membrane lengths, and a 20 kDa molecule cutoff (M Dialysis AB, Stockholm, Sweden) were used. The catheters were perfused with 0.9% NaCl at a 1 µL/min flow rate using a CMA 107 precision pump. At the end of each sampling period, retrodialysis with azithromycin solutions of 10 µg/mL and 1,000 µg/mL was performed to calibrate the system (6). Azithromycin concentrations were quantified using high-performance liquid chromatography.
Results
Following the debridement surgery, the free concentrations of azithromycin measured with microdialysis in muscle, subcutaneous tissue, and the tendon sheath ranged from 0.5 to 1.8 µg/mL (Fig. 2). Plasma azithromycin total concentrations ranged from 0.3 to 1.1 µg/mL (Fig. 2). During the first reconstructive surgery, free azithromycin tissue concentrations in compartments not directly exposed to the azithromycin-loaded beads ranged from 0.3 to 1.7 µg/mL (Fig. 2). In contrast, tissues in direct contact with the beads had free azithromycin concentrations almost 100-fold higher, ranging from 56 to 151 µg/mL. Plasma azithromycin total concentrations remained between 0.1 to 0.8 µg/mL (Fig. 2), resembling those observed following debridement surgery, indicating that systemic azithromycin concentrations were unaffected by the local azithromycin treatment.
Azithromycin concentrations in plasma and target tissues, measured in relation to the debridement (DB) surgery and the first tendon reconstructive (RC) surgery.
Discussion
This case describes a three-year treatment course with documentation of perioperative azithromycin tissue concentrations in a patient with M. heraklionense hand tenosynovitis. Treatment involved surgical insertion of azithromycin-containing beads in addition to conventional systemic antibiotic therapy. A regimen consisting of azithromycin, rifabutin, and ethambutol was initiated one month before tendon reconstruction surgery and continued for 20 consecutive months.
Microdialysis revealed comparable perioperative azithromycin concentrations in plasma and various target tissues (muscle, tendon sheath, bone, and subcutaneous tissue) that were not in direct contact with the azithromycin-containing beads. These concentrations exceeded previously suggested C_max_ plasma targets of ≥0.4 and >0.2 µg/mL used in clinical studies of patients with M. avium complex lung disease (7, 8). Although these targets may not be directly applicable due to variations in species and disease manifestation, they serve as a valuable starting point in the absence of more robust alternatives. Placing azithromycin-containing beads during surgery resulted in high azithromycin concentrations in tissues directly adjacent to the beads, with tissue concentrations ranging from 56 µg/mL to 151 µg/mL. Unfortunately, the beads had to be surgically removed after 10 days due to excessive wound drainage from the index finger, which prevented wound healing and posed a risk of superinfection. Most likely, the thin skin flaps on the finger did not provide sufficient tissue coverage to seal the fluid production caused by the dissolution of the calcium sulfate beads. Despite the challenges associated with assessing the clinical impact of short-term azithromycin exposure, it may have reduced the perioperative mycobacterial load in comparison to systemic treatment alone. Nevertheless, such an assertion remains speculative, and it is not possible to ascertain the clinical efficacy of the local therapy based solely on this case.
For NTM hand infections, a combination of antibiotics is typically administered over many months, with or without surgery (1). Nevertheless, there is a lack of comprehensive clinical evidence to inform treatment protocols and the optimal duration of therapy (9). Recently, Stemkens et al. successfully incorporated topical antibiotic treatment (NPWTi-d) alongside systemic antibiotics in three similar cases of skin and soft tissue mycobacterial infections (10). In our case, we tried to enhance the understanding of specific tissue concentrations in treating NTM tenosynovitis while also implementing a novel mode of antibiotic delivery. Together, these cases offer intriguing, albeit experimental, perspectives on how topical antibiotics could reduce the local mycobacterial burden to supplement systemic treatment in NTM infections. However, applying localized therapeutic strategies necessitates additional refinement to establish their safety and efficacy thoroughly.
The current pharmacokinetic studies of azithromycin in clinical settings involving NTM infections have focused on patients with lung disease caused by the M. avium complex, a rapidly growing mycobacterium (7, 8). In contrast, M. heraklionense is a slow-growing mycobacterium, which complicates the correlation of treatment targets, as the minimal inhibitory concentration (MIC) values for macrolides (i.e., clarithromycin) are typically higher for rapidly growing mycobacteria (11). In this case, the isolate’s MIC for clarithromycin, a class drug used for drug susceptibility testing of NTM, was determined to be 8 µg/mL and considered susceptible (11, 12). However, the use of clarithromycin susceptibility testing as a surrogate for azithromycin has been questioned (12). In vivo concentrations higher than this MIC were only achieved when azithromycin was administered locally. The calcium sulfate beads may have influenced the intracellular uptake in neutrophils and macrophages, which serve as the primary reservoir, noting that pH and calcium levels significantly regulate this uptake (13). It remains uncertain whether this influence has compromised the efficacy of the antibiotic.
No quantification of coadministered rifabutin or ethambutol concentrations was obtained in this case, making it difficult to evaluate synergistic or antagonistic treatment effects. However, in the treatment of M. avium complex, which may be an imperfect comparison, rifamycins and ethambutol are primarily used as companion drugs to prevent the development of macrolide resistance (14).
Conclusion
This case highlights the challenges of diagnosing and treating NTM hand tenosynovitis. Systemically administered azithromycin may achieve adequate target site concentrations with comparable steady concentrations in target hand tissue and plasma. Still, this is highly reliant on the intricacies of the target discussion. A 100-fold higher azithromycin target tissue concentration can be achieved with local treatment. Nonetheless, using antibiotic calcium sulfate beads as a carrier should be used with caution in anatomical sites with thin skin flaps, such as the fingers, since excessive wound drainage may complicate wound healing and pose a risk of superinfection. While systemic antibiotics and surgery remain central to NTM treatment, the role of local antibiotic administration in reducing bacterial burden warrants further investigation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tabaja H, Saleem HY, Bakri K, Tande AJ. 2024. Two decades of insights into nontuberculous mycobacterial hand infections. Open Forum Infect Dis 11:ofae 152. doi:10.1093/ofid/ofae 15238651140 PMC 11034953 · doi ↗ · pubmed ↗
- 2Tortoli E, Gitti Z, Klenk H-P, Lauria S, Mannino R, Mantegani P, Mariottini A, Neonakis I. 2013. Survey of 150 strains belonging to the Mycobacterium terrae complex and description of Mycobacterium engbaekii sp. nov., Mycobacterium heraklionense sp. nov. and Mycobacterium longobardum sp. nov. Int J Syst Evol Microbiol 63:401–411. doi:10.1099/ijs.0.038737-022447702 · doi ↗ · pubmed ↗
- 3Dutronc H, Sawaya E, Poursac N, Desclaux A, Ménard A, Peuchant O. 2023. Mycobacteriumheraklionense as an emerging cause of tenosynovitis. J Microbiol Immunol Infect 56:197–199. doi:10.1016/j.jmii.2022.08.01936137925 · doi ↗ · pubmed ↗
- 4Dahl VN, Burke A, Fløe A, Bruchfeld J, Schön T, Wejse CM, Andersen AB, Svensson E, van Ingen J, Davies Forsman L. 2024. Advantages and limitations of virtual multi-disciplinary team meetings on difficult-to-treat mycobacteria. Int J Tuberc Lung Dis 28:212–213. doi:10.5588/ijtld.23.055138563342 · doi ↗ · pubmed ↗
- 5Joukhadar C, Müller M. 2005. Microdialysis: current applications in clinical pharmacokinetic studies and its potential role in the future. Clin Pharmacokinet 44:895–913. doi:10.2165/00003088-200544090-0000216122279 · doi ↗ · pubmed ↗
- 6Kho CM, Enche Ab Rahim SK, Ahmad ZA, Abdullah NS. 2017. A review on microdialysis calibration methods: the theory and current related efforts. Mol Neurobiol 54:3506–3527. doi:10.1007/s 12035-016-9929-827189617 · doi ↗ · pubmed ↗
- 7van Ingen J, Egelund EF, Levin A, Totten SE, Boeree MJ, Mouton JW, Aarnoutse RE, Heifets LB, Peloquin CA, Daley CL. 2012. The pharmacokinetics and pharmacodynamics of pulmonary Mycobacterium avium complex disease treatment. Am J Respir Crit Care Med 186:559–565. doi:10.1164/rccm.201204-0682 OC 22744719 · doi ↗ · pubmed ↗
- 8Jeong B-H, Jeon K, Park HY, Moon SM, Kim S-Y, Lee S-Y, Shin SJ, Daley CL, Koh W-J. 2016. Peak plasma concentration of azithromycin and treatment responses in Mycobacterium avium complex lung disease. Antimicrob Agents Chemother 60:6076–6083. doi:10.1128/AAC.00770-1627480854 PMC 5038230 · doi ↗ · pubmed ↗