Propranolol is efficacious against Aspergillus and Fusarium corneal isolates in vitro and in a murine model of Aspergillus keratitis
Michael E. Zegans, Manali M. Kamath, Jane T. Jones, Ruina Bao, Brandon S. Ross, Cecilia Gutierrez-Perez, Emily M. Adams, Jorge D. Lightfoot, Galini Poimenidou, Chetan Pavuluri, Venkatesh Prajna, Robert A. Cramer, Kevin K. Fuller

TL;DR
Propranolol, a beta-blocker, shows antifungal effects against corneal fungi in lab tests and in a mouse model, suggesting it could be a new treatment for fungal eye infections.
Contribution
The study demonstrates propranolol's efficacy against Aspergillus and Fusarium in vitro and in a murine model of keratitis.
Findings
Propranolol displays antifungal activity against Aspergillus and Fusarium corneal isolates in vitro.
Propranolol blocks disease establishment in a murine model of Aspergillus fumigatus keratitis.
Abstract
Fungal keratitis is a severe corneal infection most commonly caused by filamentous fungi. Even with prompt treatment with current antifungals, it often results in corneal perforation and blindness. In this report, we observe that the beta-adrenergic antagonist, propranolol, displays antifungal activity against Aspergillus and Fusarium corneal isolates in vitro and strikingly blocks disease establishment in a murine model of Aspergillus fumigatus keratitis. These findings suggest that beta-blockers have potential as a novel FK treatment. This study is registered with ClinicalTrials.gov as NCT00997035 (MUTT Trial).
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
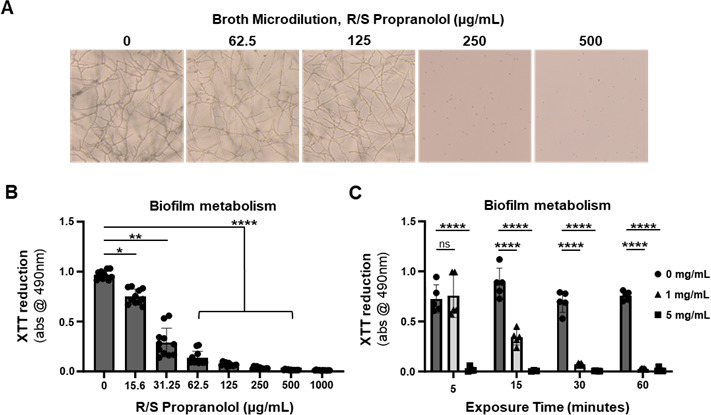 Fig 1
Fig 1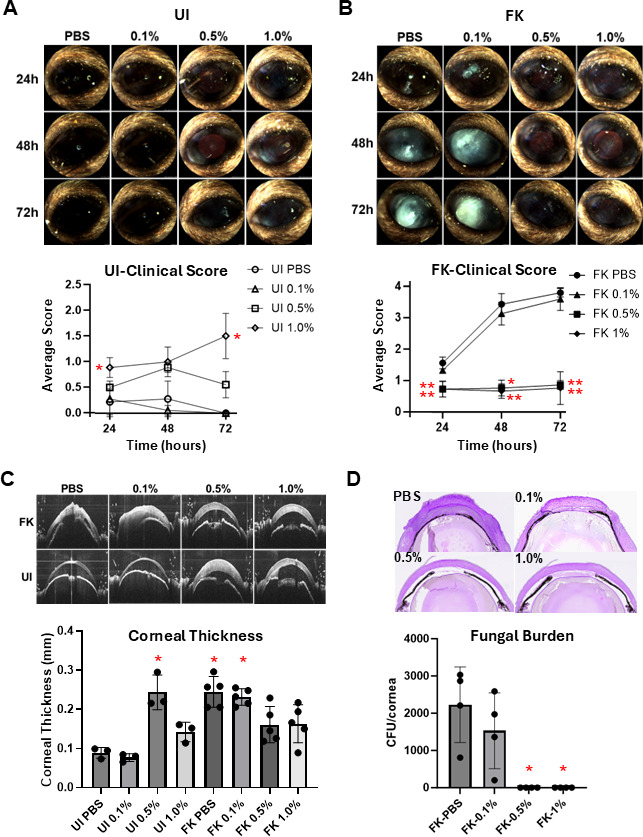 Fig 2
Fig 2| Species | R-propranolol | S-propranolol | R/S-propranolol |
|---|---|---|---|
|
| |||
| Af293 | 250 | 125 | 250 |
| A1163 | 125 | 125 | 125 |
| IFM59356-1 | 125 | 125 | 125 |
| IFM59356-3 | 250 | 250 | 250 |
| Af110-5.3 | 250 | 250 | 125 |
| Af100-10.1 | 250 | 250 | 250 |
| MIC range | 125–250 | 125–250 | 125–250 |
| MUTT 1121U | 52 | 52 | 31 |
| MUTT 1146N | 52 | 52 | 63 |
| MUTT 1584Q | 52 | 63 | 52 |
| MUTT 1587W | 47 | 42 | 42 |
| MUTT 1736Z | 31 | 42 | 42 |
| MUTT 1753Z | 31 | 42 | 31 |
| MUTT 2725Z | 42 | 63 | 52 |
| MUTT 2226R | 47 | 52 | 52 |
| UCSF 06-0110 | 42 | 52 | 52 |
| UCSF 06-0111 | 26 | 52 | 42 |
| UCSF 06-0133 | 26 | 52 | 31 |
| UCSF 06-0330 | 26 | 52 | 42 |
| UCSF 06-0487 | 52 | 63 | 31 |
| DUMC 132.02 | 31 | 73 | 73 |
| UCSF 06–0197 | 42 | 52 | 52 |
| UCSF 06–0342 | 42 | 63 | 52 |
| MUTT 1090Z | 83 | 104 | 83 |
| MUTT-1170W | 27 | 42 | 42 |
| MIC Range | 27–83 | 42–104 | 31–83 |
- —National Eye Institutehttp://dx.doi.org/10.13039/100000053
- —National Institute of Allergy and Infectious Diseaseshttp://dx.doi.org/10.13039/100000060
- —National Heart Lung & Blood Institutehttp://dx.doi.org/10.13039/100000050
- —Cystic Fibrosis Foundationhttp://dx.doi.org/10.13039/100000897
- —National Eye Institutehttp://dx.doi.org/10.13039/100000053
- —National Eye Institutehttp://dx.doi.org/10.13039/100000053
- —National Eye Institutehttp://dx.doi.org/10.13039/100000053
- —Research to Prevent Blindnesshttp://dx.doi.org/10.13039/100001818
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Infections and Treatments · Essential Oils and Antimicrobial Activity · Antifungal resistance and susceptibility
INTRODUCTION
Fungal keratitis (FK) is a severe and often blinding infection commonly caused by filamentous fungi. Despite the introduction of newer antifungals, such as the azoles, the polyene natamycin remains the only Food and Drug Administration-approved drug for FK treatment. Indeed, the Mycotic Ulcer Treatment Trials (MUTT-I and II) found that voriconazole, a drug-of-choice for many systemic mold infections, is inferior to natamycin as a topical monotherapy and provides minimal benefit as an oral supplement to topical therapy alone (1). Both studies revealed a high rate of corneal perforation and/or transplantation even with natamycin treatment. Transplanted corneas in the MUTT-II were culture positive in 67% cases. These findings, in agreement with other studies, indicate that currently available antifungals often fail to achieve a microbiologic cure, and fungal persistence drives poor clinical outcomes. The development of better FK therapies is therefore a clinical imperative. We previously reported that the beta-adrenergic antagonist (a.k.a. beta-blocker) timolol is not intrinsically antifungal but synergizes with natamycin against filamentous fungi at concentrations comparable to those used to treat glaucoma (2). Interestingly, several studies have reported direct antifungal activity of another beta-blocker, propranolol, against Candida albicans and the plant pathogen Magnaporthe oryzae (3, 4). Here, we explore the activity of propranolol against FK-relevant molds and its potential use as an FK therapeutic in vivo.
We began by screening the activity of R-, S-, and R/S-propranolol (Sigma-Aldrich) against six Aspergillus fumigatus strains, a common FK agent, in a standard broth microdilution assay. Briefly, conidia were harvested from glucose minimal media (GMM) plates and inoculated into RPMI-1640 media at a final density of 5.0 × 10^4^/mL in 200 µL (2). Following 48 h incubation at 37°C (atmospheric conditions), both enantiomers and the racemic mixture of propranolol inhibited germination of each strain at 125–250 µg/mL (Table 1 and Fig. 1A). To determine if this antifungal activity extended to the hyphal (tissue invasive) form of the fungus, biofilms of strain Af293 were pre-formed in 96-well plates overnight in GMM broth, washed and overlaid with R/S-propranolol containing RPMI-media, and incubated for 2 h before measuring the metabolic activity of the biomass using the 2,3-bis-(2-methoxy-4-nitro-5-sulphenyl)-(2H)-tetrazolium-5-carboxanilide (XTT) reduction assay. Interestingly, though a complete loss in metabolic activity was noted at concentrations that corresponded to the above-described conidial MICs (125–250 µg/mL), statistically relevant decreases in XTT reduction were noted as low as 16 µg/mL (Fig. 1B). Taken together, these results indicate that propranolol has antifungal activity below its MIC and is active against both Aspergillus conidia and biofilms.
In vitro antifungal activity of R/S propranolol against Aspergillus fumigatus. (A) Conidia of A. fumigatus (Af293) were incubated in RPMI containing R/S propranolol at 35°C for 48 h. (B) Conidia of Af293 were incubated in glucose minimal media (GMM) for 24 h and subsequently washed and overlaid with RPMI media containing R/S propranolol at 35°C for 2 h. The metabolic activity of the biofilm was then analyzed by XTT assay, and groups were compared using ordinary one-way ANOVA, where asterisks reflect statistical significance relative to the untreated group based on Dunnett’s post hoc test for multiple comparisons. (C) Conidia of Af293 were incubated in GMM for 24 h and subsequently washed and overlaid with RPMI media containing R/S propranolol at 35°C for 2 h for the indicated times. The metabolic activity of the biofilm was then analyzed by XTT assay, and groups at each time point were compared using two-way ANOVA. Asterisks reflect statistical significance relative to the untreated group at each time point based on Dunnett’s post-hoc test for multiple comparisons: (ns) not significant; (**) P < 0.0001. For panels B and C: (ns) not significant; () P < 0.05; (***) P < 0.0001.
To assess the antifungal activity of propranolol on the ocular surface, we utilized an established corneal abrasion (Algerbrush) model of FK using immunosuppressed C57BL/6J mice and A. fumigatus strain Af293 (5–8). On the day preceding fungal inoculation, animals began a once-daily treatment with 2 mg/kg R/S-propranolol by intraperitoneal (i.p.) injection, which recapitulates a prior report in which such treatments reduced kidney fungal burden in a murine model of systemic candidiasis (9). Unique to our study, animals further received a single topical treatment of 1 mg/mL (0.1%), 5 mg/mL (0.5%), or 10 mg/mL (1%) propranolol diluted in PBS on day 0, several hours after fungal inoculation, by anesthetizing them with isoflurane and applying a 5 µL drop to the ocular surface for 5 min. On days + 1 and +2, animals received three topical treatments, 3 h apart, at the same concentration. Groups of five corneas (corresponding to five animals) were used for each topical treatment concentration in addition to a sham-treated group that received both systemic and topical PBS on the same schedule. The contralateral eyes were used as sham-inoculated (uninfected, UI) controls and received the same treatment as the infected (FK) eye. Corneal pathology was tracked longitudinally by slit-lamp (Micron IV) for clinical disease scoring and by optical coherence tomography (OCT) to quantify corneal thickness, as previously described (5–8). Eyes were harvested at 72 h to quantify fungal burden, based on colony forming units (CFU), or for histological endpoints. As shown in Fig. 2, FK corneas that were treated with either PBS or 0.1% topical propranolol developed a progressive corneal opacification that was associated with increased tissue thickness (edema) (Fig. 2C), fungal load, and inflammation at 72 h post-inoculation (p.i.). By contrast, eyes treated with 0.5% or 1.0% topical propranolol remained largely indistinguishable from uninfected control eyes, and this corresponded to an absence of viable fungus and minimal inflammation at end point. Congruent with our in vivo data, when Af293 biofilms were incubated with 0.5% propranolol in vitro, a complete loss in fungal metabolism (XTT reduction) was observed in as early as 5 min; by contrast, it took 30 min of exposure to 0.1% propranolol to achieve the same effect (Fig. 1C). These results indicate that topical propranolol can exert antifungal effects on the ocular surface of mice in a dose-dependent manner.
Topical propranolol reduces fungal growth and disease burden in a murine model of Aspergillus fumigatus fungal keratitis. (A–B) Representative slit-lamp images of uninfected (UI) or A. fumigatus-infected (FK) corneas treated with the indicated concentration of topical R/S-propranolol or vehicle (PBS). All treated animals also received daily intraperitoneal injections of 2 mg/kg propranolol. Mean clinical disease scores are plotted (±SD) (n = 5/treatment group). Groups were compared at each time point by Kruskal-Wallis test, and asterisks reflect statistical significance relative to either the UI-PBS (panel A) or FK-PBS (panel B) groups based on Dunn’s post-hoc test for multiple comparisons. (C) OCT scans of UI and FK corneas (the same as panels A and B), taken at 72 h p.i. Mean corneal thickness measurements based on the OCT images are plotted (±SD). Groups were compared by Kruskal-Wallis test, and asterisks reflect statistical significance relative to the UI-PBS group based on Dunn’s post-hoc test for multiple comparisons. (D) At 72 h p.i., eyes were either resected for PASH staining (1/group) or homogenized for CFU analysis (4/group). Mean CFUs (±SD) are plotted. Groups were compared by the Kruskal-Wallis test, and asterisks reflect statistical significance relative to the FK-PBS group based on Dunn’s post-hoc test for multiple comparisons. For all panels: () P < 0.05; (**) P < 0.01.*
Interestingly, uninfected corneas that received 0.5 and 1% topical propranolol, but not the 0.1% concentration, displayed signs of corneal edema based on OCT, despite appearing largely healthy based on slit-lamp scores (Fig. 2A and C). While topical natamycin has also been reported to cause ocular surface disease including edema (10), it is nevertheless intriguing to speculate that propranolol at the higher concentrations may be altering corneal physiology. Topical 1% propranolol was investigated in the past for use in glaucoma (11). More recently, a trial was conducted with topical 0.2% propranolol for the treatment of retinopathy of prematurity in infants (12). While we did not find reports of propranolol inducing corneal edema, further studies will be required to better understand these findings.
To gain additional insight into the potential scope of propranolol’s clinical utility in FK, we conducted susceptibility testing against 18 Fusarium corneal isolates obtained from India (the MUTT1 and 2 studies) as well as the United States (1, 2). Microconidia were collected from potato dextrose broth cultures, set up in a broth microdilution assay as described above for A. fumigatus, and incubated for 72 h incubation at 30°C. Remarkably, the three propranolol formulations inhibited all tested Fusarium isolates and did so at a lower concentration range (27–104 µg/mL) than was observed for A. fumigatus (Table 1).
In summary, propranolol has antifungal activity against the FK-relevant molds, A. fumigatus and Fusarium spp. Although the mechanism of action of the drug against these fungi remains an open area of investigation, the fact that the R- and S- enantiomers display comparable efficacy, as well as the apparent lack of beta-adrenergic receptor orthologs in the fungi, suggests that propranolol’s activity against fungi is distinct from its cardiovascular effects in humans (13). Prior work in both Candida and Magnaporthe observed propranolol-mediated inhibition of PLD1 and MoPah1 enzymes, respectively, both of which convert phosphatidic acid to diacylglycerol and are therefore involved in lipid metabolism and membrane homeostasis (3, 4). Similarly, propranolol (racemic and the R and S enantiomers) has been observed to block this pathway in humans via inhibition of phosphatidate phosphohydrolase (14). We are pursuing this and other possible mechanisms in Aspergillus and Fusarium, and such efforts may reveal novel proteins/pathways important for FK pathogenesis. Mechanism aside, the feasibility of developing propranolol as an FK therapeutic is supported by the fact that it has been safely used on the human ocular surface at concentrations similar to those tested here (11, 12). Finally, the evaluation of propranolol in a Fusarium FK model, its synergism with natamycin and other antifungals, and the effects of the drug on corneal biology/immunology will be important next steps in evaluating the therapeutic potential of propranolol for FK.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prajna NV, Krishnan T, Rajaraman R, Patel S, Srinivasan M, Das M, Ray KJ, O’Brien KS, Oldenburg CE, Mc Leod SD, Zegans ME, Porco TC, Acharya NR, Lietman TM, Rose-Nussbaumer J, Mycotic Ulcer Treatment Trial II Group. 2016. Effect of oral voriconazole on fungal keratitis in the Mycotic Ulcer Treatment Trial II (MUTT II): a randomized clinical trial. JAMA Ophthalmol 134:1365–1372. doi:10.1001/jamaophthalmol.2016.409627787540 PMC 6044431 · doi ↗ · pubmed ↗
- 2Rees CA, Bao R, Zegans ME, Cramer RA. 2019. Natamycin and voriconazole exhibit synergistic interactions with nonantifungal ophthalmic agents against Fusarium species ocular isolates. Antimicrob Agents Chemother 63:e 02505-18. doi:10.1128/AAC.02505-1831010869 PMC 6591621 · doi ↗ · pubmed ↗
- 3Zhao J, Chen Y, Ding Z, Zhou Y, Bi R, Qin Z, Yang L, Sun P, Sun Q, Chen G, Sun D, Jiang X, Zheng L, Chen X-L, Wan H, Wang G, Li Q, Teng H, Li G. 2024. Identification of propranolol and derivatives that are chemical inhibitors of phosphatidate phosphatase as potential broad-spectrum fungicides. Plant Commun 5:100679. doi:10.1016/j.xplc.2023.10067937653727 PMC 10811373 · doi ↗ · pubmed ↗
- 4Baker CA, Desrosiers K, Dolan JW. 2002. Propranolol inhibits hyphal development in Candida albicans. Antimicrob Agents Chemother 46:3617–3620. doi:10.1128/AAC.46.11.3617-3620.200212384374 PMC 128717 · doi ↗ · pubmed ↗
- 5Kamath MM, Lightfoot JD, Adams EM, Kiser RM, Wells BL, Fuller KK. 2023. The Aspergillus fumigatus UPR is variably activated across nutrient and host environments and is critical for the establishment of corneal infection. P Lo S Pathog 19:e 1011435. doi:10.1371/journal.ppat.101143537906600 PMC 10637725 · doi ↗ · pubmed ↗
- 6Dos Reis TF, de Castro PA, Bastos RW, Pinzan CF, Souza PFN, Ackloo S, Hossain MA, Drewry DH, Alkhazraji S, Ibrahim AS, Jo H, Lightfoot JD, Adams EM, Fuller KK, de Grado WF, Goldman GH. 2023. A host defense peptide mimetic, brilacidin, potentiates caspofungin antifungal activity against human pathogenic fungi. Nat Commun 14:2052. doi:10.1038/s 41467-023-37573-y 37045836 PMC 10090755 · doi ↗ · pubmed ↗
- 7Lightfoot JD, Adams EM, Kamath MM, Wells BL, Fuller KK. 2024. Aspergillus fumigatus hypoxia adaptation is critical for the establishment of fungal keratitis. Invest Ophthalmol Vis Sci 65:31. doi:10.1167/iovs.65.4.31PMC 1104483438635243 · doi ↗ · pubmed ↗
- 8Kamath MM, Adams EM, Lightfoot JD, Wells BL, Fuller KK. 2024. The mammalian Ire 1 inhibitor, 4µ8C, exhibits broad anti-Aspergillus activity in vitro and in a treatment model of fungal keratitis. Front Cell Infect Microbiol 14:1477463. doi:10.3389/fcimb.2024.147746339600871 PMC 11588707 · doi ↗ · pubmed ↗