The emotional cost of containment: a cross-sectional analysis of treatment effects among informal carers in South Asia during the COVID-19 pandemic
Carol Troy, Anna Tjin, Anna Goodwin, Iracema Leroi, Roger O’Sullivan, Yaohua Chen

TL;DR
This study explores how pandemic containment measures in South Asia affected the emotional well-being of informal caregivers and suggests ways to support them in future crises.
Contribution
The study identifies specific emotional costs of pandemic policies on caregivers in South Asia and proposes culturally embedded support strategies.
Findings
Social confinement and restricted visitation rights caused persistent emotional costs for caregivers.
Emotional costs were highest when caregiving intensity increased or decreased unexpectedly from pre-pandemic levels.
Counseling and emotional support services can help reduce caregiver distress during crises.
Abstract
The COVID-19 pandemic led to government-imposed mobility restrictions, social distancing, and lockdowns, altering the caregiving environment worldwide. In South Asia, it is unknown what aspects of these changes posed significant emotional costs to informal carers, or how such costs can be mitigated in future pandemics. To identify environmental change aspects (dimensions) that posed distinct emotional costs for South Asian carers. To quantify the costs and classify them as persistent, transient, hidden, or insignificant. To propose ways of mitigating carer distress during future pandemics. The data came from the Coping with Loneliness, Isolation, and COVID-19 Caregiver survey. Carers (n=454) in Bangladesh (N=123), India (N=116), and Pakistan (N=215) self-reported their experiences before/during the pandemic. The dimensions were extracted from 11 change indicators. A dimension’s…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
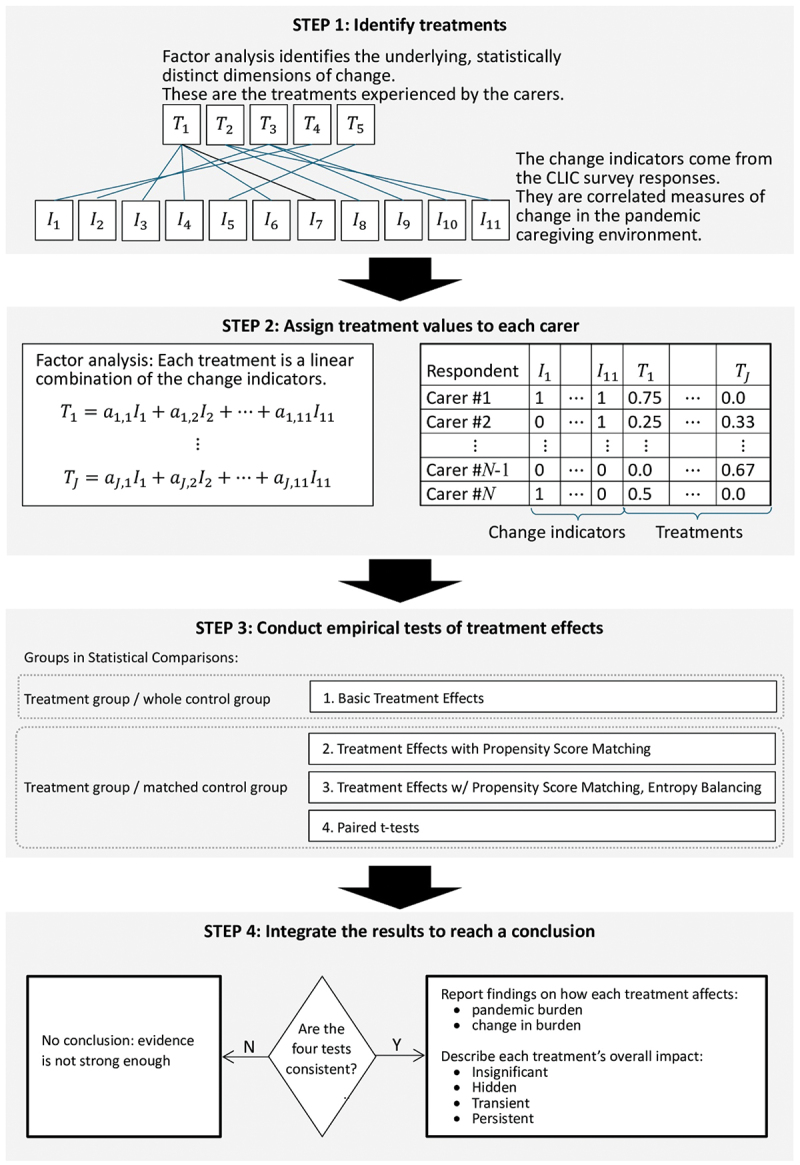 Figure 1
Figure 1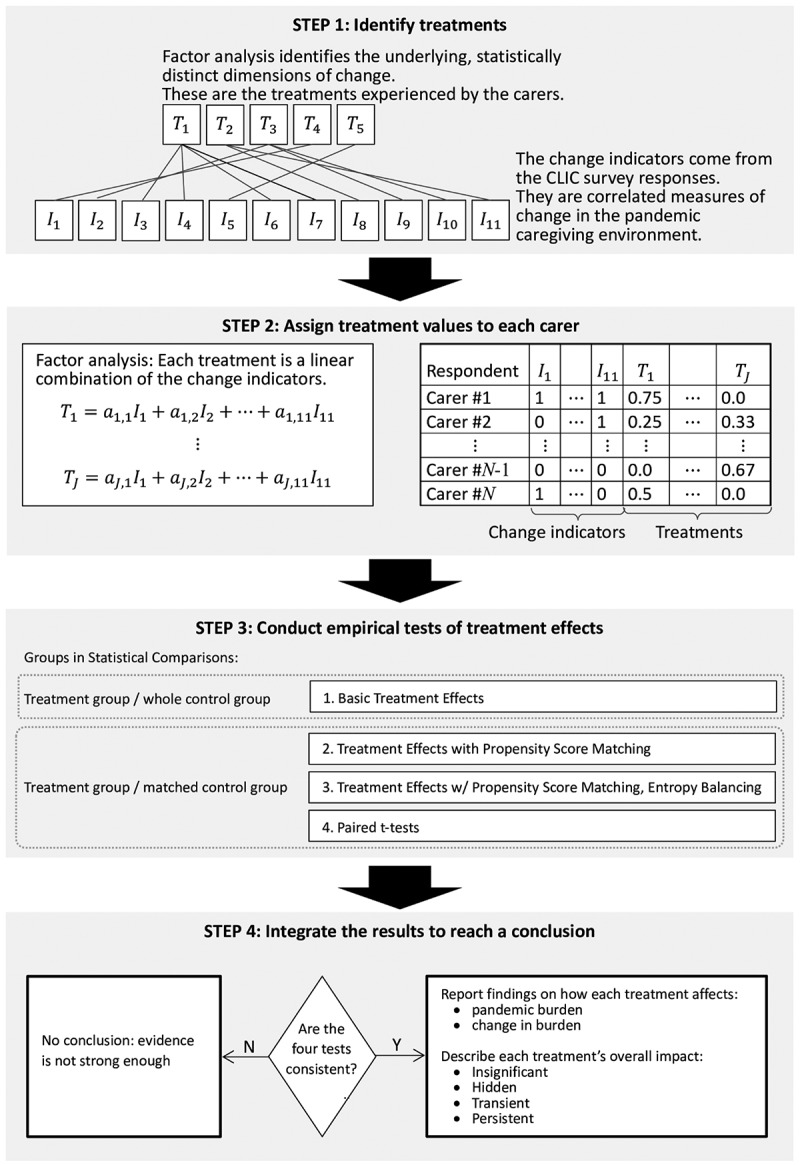 Figure 2
Figure 2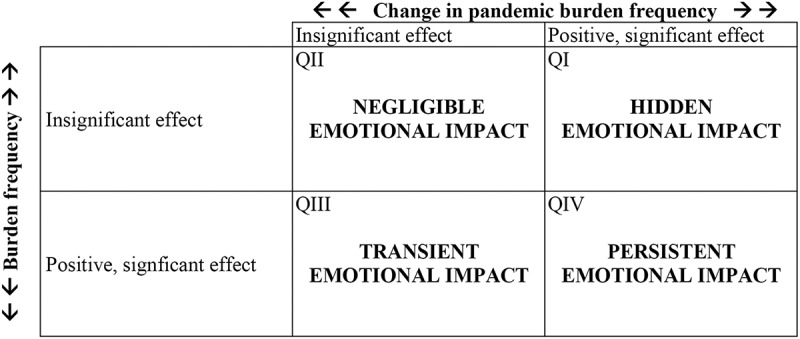 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5 Figure 6
Figure 6 Figure 7
Figure 7 Figure 8
Figure 8 Figure 9
Figure 9 Figure 10
Figure 10 Figure 11
Figure 11 Figure 12
Figure 12 Figure 13
Figure 13 Figure 14
Figure 14 Figure 15
Figure 15 Figure 16
Figure 16 Figure 17
Figure 17 Figure 18
Figure 18 Figure 19
Figure 19 Figure 20
Figure 20 Figure 21
Figure 21 Figure 22
Figure 22 Figure 23
Figure 23 Figure 24
Figure 24 Figure 25
Figure 25 Figure 26
Figure 26 Figure 27
Figure 27 Figure 28
Figure 28 Figure 29
Figure 29 Figure 30
Figure 30 Figure 31
Figure 31 Figure 32
Figure 32 Figure 33
Figure 33 Figure 34
Figure 34 Figure 35
Figure 35 Figure 36
Figure 36 Figure 37
Figure 37 Figure 38
Figure 38 Figure 39
Figure 39 Figure 40
Figure 40 Figure 41
Figure 41 Figure 42
Figure 42 Figure 43
Figure 43 Figure 44
Figure 44 Figure 45
Figure 45 Figure 46
Figure 46 Figure 47
Figure 47 Figure 48
Figure 48 Figure 49
Figure 49 Figure 50
Figure 50- —National Science and Technology Council10.13039/100020595
- —Irish Research Council10.13039/501100002081
- —Trinity College10.13039/100022647
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntergenerational Family Dynamics and Caregiving · COVID-19 and Mental Health · Health disparities and outcomes
Background
During the early stages of the COVID-19 pandemic, governments throughout the globe instituted public health containment policies, including mobility restrictions, international travel bans, social distancing, event cancellations, school and work closures, mask mandates, and lockdowns [1–5]. These measures were enforced by institutions and businesses [6,7], particularly at the peak of the pandemic [8,9]. Although the policies achieved some successes in limiting disease transmission [10,11], they changed the caregiving environment in unintended ways. This had consequences for informal carers [12–15], the individuals who deliver unpaid assistance and support to family, friends, and loved ones. The containment measures upended established care routines in numerous households [16,17]. Needed caregiving inputs, such as medical care, daycare services, and informal assistance (e.g. from friends or family) became scarce [8,18], while demanded outputs (e.g. time spent with the recipient) increased [19]. Disruptions to personal lives (e.g. job losses and school closures) spilled over into caregiving, posing additional obstacles, particularly for women [20,21]. Carers adapted to these environmental changes by redoubling their efforts to meet the new demands without compromising quality [22]. For some carers, the adaptations brought psychological impacts beyond the baseline pre-pandemic levels, including more frequent feelings of burden. Thus, the COVID-19 containment strategies adopted by governments posed ‘emotional costs’ for carers. The caregiving literature defines emotional cost as ‘the emotional value a subject pays, in terms of suffering and discomfort, when faced with extreme or traumatic situations’ [23]. Since national health care services throughout the world rely on informal carers [24], recognizing the emotional costs they face is essential to evaluating policies and ensuring the sustainability of informal care systems. This paper will focus on assessing the emotional costs of the COVID-19 pandemic containment measures.
The pandemic caregiving environment in low- and high-income regions
At the outset of the pandemic, countries worldwide adopted similar containment policies, but implemented them differently, with important consequences for informal carers. In the EU and US, COVID-19 restrictions were shaped by federated governance structures. However, the EU’s response was faster and more cohesive: all 27 members enacted lockdowns by 19 March, compared to just two US states, and more members adopted the strictest lockdowns [25,26]. Mask mandates, mobility restrictions, and internal border controls were implemented more uniformly across the EU [27–29], under the coordination of institutions like the European Commission and the ECDC. In the US, decentralized health infrastructure, lack of national caregiver strategies and support services [30], political polarization [31], and inconsistent public messaging [32] produced a fragmented response. For informal carers, especially women balancing paid work and caregiving, this patchwork response created anxiety, uncertainty, and exhaustion [30,33].
Stress among informal carers in East Asian countries (e.g. China, South Korea, Japan, and Taiwan) was mitigated by the centralized and technologically supported strategies of their governments. Like the EU, these countries promptly imposed mobility restrictions and border controls. By late March, all EU members except Ireland had barred non-essential non-EU travellers [34]; likewise, in late March and early April, China, Japan, and Taiwan implemented near-total bans, and South Korea established 14-day quarantines [35–38]. East Asian countries adopted digital technologies for contact tracing, surveillance, and supply distribution [39]. Moreover, higher levels of government trust − 95.4% in China, 51.3% in South Korea, 43.4% in Japan, and 51.8% in Taiwan, versus 30.3% in the EU and 31.0% in the US – boosted compliance and reduced the psychological toll associated with rule ambiguity and public dissent [40]. East Asian carers faced isolation and increased workloads, but often within clearer and more predictable policy environments.
Despite differences in execution, the EU, US, and East Asian strategies all relied on costly interventions, e.g. economic relief to businesses and citizens [41–48] and emergency funding for health systems and infrastructure [31,49–55]. These programs offered some protection for carers in high-income countries. By contrast, low- and middle-income countries (LMICs), following WHO guidance [56] and mimicking the strategies of first-affected countries like China and Italy (e.g. lockdowns and mobility restrictions) [57], lacked the resources to offer equivalent support. Their standardized, top-down containment policies could not accommodate socioeconomic realities such as informal labor markets, overcrowding, and weak health infrastructure [57]. For informal carers in these settings, especially in South Asia, the result was emotional hardship: heightened anxiety, burnout, and a sense of helplessness in the face of mounting demands and limited institutional support.
The pandemic caregiving environment in South Asia
Three South Asian countries, Bangladesh, India, and Pakistan, exemplified the contradictions of COVID-19 containment in LMICs. Medical resources were relatively scarce: pre-pandemic, South Asia had fewer than half the per capita number of doctors and hospital beds [58] typical in Western countries (e.g. the UK). During the pandemic, healthcare became even less accessible, and by many measures, the quality declined [59]. Fear of contagion often caused patients to avoid hospital visits [2,5]. Some facilities were reserved for COVID-19 patients, further limiting doctor availability [60–62]. Carer access to medical services was therefore severely disrupted.
Lockdowns and closures had detrimental effects on caregiving support services. In a qualitative study of caregiving to persons with dementia, Vaitheswaran et al. [63] found that pre-pandemic, Indian carers had formal and informal support networks, which dwindled during the pandemic. Daycare services were often suspended [64,65], depriving carers of respite and recipients of medical services (e.g. physical rehabilitation). Mobility restrictions also limited assistance from non-cohabiting family members [18], exacerbating the strain on the carer.
During the initial pandemic period, there was a global shortage of Personal Protective Equipment (PPE) [3]. In South Asia, the needs of hospital staff were prioritized. Volunteers and low-paid carers such as community health workers [5,66] struggled to access PPE, often resorting to hand-made substitutes. Inadequate access to PPE heightened stress and fears of COVID-19 exposure.
The benefits of this study
By examining informal carers in South Asia, this paper will address a research gap, as LMICs like Bangladesh, India, and Pakistan are underrepresented in the literature favoring high-income regions. Furthermore, the study will provide a window on three societies in rapid transition. The caregiving environments in these countries are similar in terms of history, cultural heritage, geography, and socio-economic characteristics [58]. In the traditional South Asian family structure, individuals accept a strict division of labor, subordinating their personal ambitions to the caregiving needs of the family [67]. However, demographic pressures have subjected the informal care system to unprecedented strain, and the ageing trend may be eroding this caregiving orientation.1^1^North and Fiske [131] argue that rapid ageing has caused demographic strains in Eastern societies, making ageism and age-based stereotyping more prevalent than in the West. The pandemic exerted an additional stress test, which has thrown a spotlight on the underlying tensions.
The COVID-19 pandemic was a natural experiment enabling researchers to observe how the informal care system stood up during a crisis. As informal caregiving is voluntary and non-monetary, the resulting stresses cannot be measured in dollars. This study conceptualizes the negative impacts as ‘treatments’ requiring emotionally costly adjustments. To evaluate these emotional costs, the study will do three things. First, using survey data from 454 predominantly young, well-educated carers in Bangladesh, India, and Pakistan, it will identify the latent dimensions of pandemic environmental disruption. Second, the study will estimate the effects of these changes (treatments) on two subjective carer responses: change in burden frequency and pandemic burden frequency (from henceforth, ‘burden change’, and ‘pandemic burden’). Third, the study will interpret the analysis outputs, yielding a better qualitative understanding of the stresses experienced by the carers. It will illustrate how globally implemented health policies aimed at limiting contagion created an exogenous shock in the South Asian environment that impacted carers’ ability to perform their duties.
Methods
This section describes the questionnaire and sample, summarizes the analysis strategy, and presents the variables. The technical details of the analysis are covered in the Supplementary online Appendix.
CLIC caregiver questionnaire
The data came from Coping with Loneliness, Isolation, and COVID-19 (CLIC), an international study using a cross-sectional online self-administered survey [68]. The CLIC responses came from over 20,000 adults in over 100 countries, collected between June and November 2020. The embedded CLIC Caregiver study focused on carers of individuals with long-term brain health and physical conditions before and during the pandemic. The survey instrument was developed by an international panel of specialists in loneliness/social isolation, dementia, and other brain health conditions in collaboration with the Alzheimer Society of Ireland (ASI) and Family Carers Ireland. It was developed in English and translated into Urdu and Bengali to increase dissemination.
The effects of the pandemic varied from one country to the next. One goal of the CLIC study was to produce region-specific analyses that explored these unequal impacts, controlling for cultural, religious, and linguistic variations [12]. This study highlights the pandemic’s effects on the well-being of South Asian carers.
Sample
The participants were informal carers (unpaid spouses, family members, and friends) born and practicing in India, Pakistan, and Bangladesh. They were identified by their affirmative response to ‘Do you provide care and support to a family member or friend with a long-term or life-limiting health problem or disability (including mental health)?’
Analysis strategy
Figure 1 depicts the analysis strategy. An overview of the four steps is presented below. The Supplementary online Appendix provides further technical details. Figure 1.Overview of analysis procedure.
Step 1 identifies the treatments. Respondents completed an 11-item checklist specifying the ways the pandemic had changed their caregiving environments. These indicators were correlated; therefore, tetrachoric factor analysis was used to distinguish the latent dimensions of environmental change, representing emotional treatments.
Step 2 assigns treatment values to the respondents. Factor analysis expresses the treatments as linear combinations of the change indicators. For each carer, the treatment magnitudes were estimated and appended to the data set.
Step 3 conducts statistical tests to evaluate the impacts of the treatments on the two emotional outcomes, pandemic burden and burden change. In the first three tests, the treatment effects were obtained from the outputs of ordinal logistic regressions. Treatment effects were obtained under three conditions: unmatched control sample, propensity score matching (PSM), and PSM with entropy balancing (EB). The fourth test was a one-sided paired -test.
Step 4 integrates the treatment-related findings. When the four tests yielded consistent results, the Figure 2 matrix was used to interpret the two combined treatment effects. The axes represent the impacts on burden change (horizontal) and pandemic burden (vertical). When both effects were insignificant (second quadrant, upper left corner), the treatment had an insignificant impact on the carer’s well-being. A significant effect on burden change only (third quadrant, lower left) indicated a transient impact: burden initially increased but then subsided, either because the change was not lasting or because the carers adjusted to the modified environment, achieving a new equilibrium. A significant effect on pandemic burden only (first quadrant, upper right) suggested a hidden impact: the carer experienced lasting stress without fully recognizing it. When both treatment effects were positive and significant (fourth quadrant, lower right), there was a persistent impact: the carer recognized the burden increase, which had durable psychological consequences lasting into the pandemic. Figure 2.Interpretations of the four possible combinations of treatment effects.
Variables
Ordinal logistic specifications were used throughout the analysis to estimate the emotional impact of each treatment on the outcome (burden change or pandemic burden). The variables, including primary stressors, secondary stressors/concordances, and background/context variables [69], are described in detail below.
Emotional outcomes
The two dependent variables describe negative emotional outcomes. Pandemic burden was measured by an item from the Zarit Burden Interview (ZBI), ‘How often do you feel burdened in your role during Covid-19?’ [70]; change in burden, by ‘Is it [the burden] the same as usual, more than usual, or less than usual?’
Treatments
The changes to the pandemic caregiving environment are conceptualized as emotionally costly treatments. In the CLIC survey, carers completed a checklist specifying changes to their caregiving environments. The treatments, derived from these data via exploratory factor analysis, are described in the Results section below.
Primary stressors
The primary stressors describe aspects of the carer/recipient relationship [71,72] that affected care demand. The first is a caregiving venue. Co-residence with the recipient posed risks of overexposure and lower quality of life [73]. Although institutional caregiving can shield carers from overexposure [19], during the pandemic it was associated with restricted access and lack of information/control over the recipient’s well-being.
The second primary stressor is recipient age. During the pandemic, carers assumed additional responsibilities over longer periods [16]. Older recipients, especially those with chronic conditions and disabilities, tended to become increasingly dependent (United Nations ESCAP 2020); child recipients, less so.
The third stressor is the recipient’s medical condition. Carers typically face longer hours, greater physical effort, more job-related complications/conflicts, and higher emotional demands with dementia patients than with patients having only physical conditions [74]. Moreover, a dementia recipient’s functional abilities may decline, while behavioral impairments may increase [75].
Secondary stressors/concordances
In the Pearlin et al. [69] framework, secondary stressors capture personal resource availability and role strains that arise when caregiving demands conflict with a carer’s preexisting role(s). This category is extended to include role concordance, a state in which care demands align with the preexisting role, making it easier to meet social expectations.
Caregiving often requires financial sacrifices [76] impacting the whole household. Carers in good financial health can meet their responsibilities without risking family hardship, while those under financial strain, e.g. from pandemic job losses [77], may struggle to fulfill role expectations [78]. This can lead to feelings of shame, inadequacy, and social stigma, as financial insufficiency is a taboo subject in South Asian culture [79] reflecting on an individual’s competence and ability to provide for loved ones.
Caregiving may involve strenuous tasks [80], e.g. positioning or moving the recipient. A carer in robust physical health can more effectively perform such tasks, while one who is in poor health can either neglect them or risk chronic pain and injury [81].
Caregiving can be mentally and emotionally taxing. A carer in sound mental and psychological health is better placed to handle demands without feeling burdened.
Employed carers may face conflicting societal expectations. During the pandemic, when time and energy reserves were reduced, they may have left care demands unmet, causing role strain and guilt. Working carers who find such burdens intolerable may ultimately quit their jobs [82]. By contrast, homemakers may find their responsibilities more compatible with caregiving, making it easier to balance social expectations.
Troy et al. [83] find that highly educated carers face an ‘expectations gap’ when caregiving conflicts with career ambitions [84]. Carers who compare themselves unfavorably to similarly educated peers may experience psychosocial stresses and emotional health issues. Among paid carers, educated females may be seen by employers as less manageable [85]. In interviews with 313 informal carers of dependent older persons, educated respondents were less likely to express positive attitudes towards the elderly [86].
Background/context variables
Caregiver burden is a multidimensional process [72] linked to the sociodemographic, economic, and health-specific characteristics of the carer [76,83]. The background/context variables capture the stable characteristics of carers and the caregiving environment.
Gender affects societal expectations concerning caregiving. Traditional South Asian norms place women, particularly daughters and daughters-in-law, at the helm of caregiving responsibilities [67]. Female carers are more exposed to all aspects of caregiving [87], with potentially greater impacts on their careers, health, and well-being [88,89]. The pandemic reportedly worsened this gender imbalance [87].
Age, marital status, and number of children are all control variables associated with the carer’s life cycle status.
Nationality is linked to pandemic changes in the caregiving environment. Although Bangladesh, India, and Pakistan adopted broadly similar COVID-19 containment policies, their enforcement approaches differed [58]. Nationality also captures country-specific demographic trends. In 2020, Pakistan’s age dependency ratio (ADR), the proportion of elderly dependents to working-aged people stood at roughly 7%, versus 8% in Bangladesh and 10% in India [90], and Pakistan’s ADR was growing much more slowly. Bangladesh and India have higher human capital indices and per capita GDP. Although these statistics hint that Pakistan may have a stronger caregiving orientation, the relationship appears to be complex. For example, Ng and Indran [91], using corpus-based measures, found that out of 20 countries, Bangladesh, Pakistan, and India ranked 1, 6, and 12 in positive perceptions of carers.
Carer residential setting (e.g. city versus village or town) is another background/context variable. In rural areas, medical services were less available to carers [92]. Containment measures were not as vigorously enforced [58].
Summary
Table 1 presents the variable definitions.Table 1.Variable definitions.Variable name/categoryDescriptionCaregiving outcomes Five-level ordinal response to the question ‘During COVID-19 how often do you feel burdened in your caring role?’ Three-level ordinal response to the follow-up question, ‘Is this the same as usual, less than usual, or more than usual?’Environmental change ( )Continuous measure reflecting the inescapability of the care setting (i.e. feeling ‘trapped’) ( )Continuous measure reflecting the carer’s lack of access to needed medical information ( )Continuous measure reflecting the carer’s feeling of losing connection with the recipient and/or others regarding the recipient’s care ( )Binary indicator that the carer has lost access to the recipient, e.g. because of a ‘no visitors’ policy at a care facility ( )Binary indicator that the need to wear protective clothing (e.g. face masks)Primary stressors Categorical variable identifying one of four possible care venues A categorical variable specifying Binary indicator that the care recipient has a physical condition Binary indicator that the care recipient has dementia Binary indicator that the care recipient has a condition other than physical or dementiaSecondary Stressors Three-level ordinal measure of carer financial health Three-level ordinal measure of carer physical health Three-level ordinal measure of carer mental health Three-level ordinal variable describing the carer’s highest educational qualification Categorical variable specifying one of four possible carer employment statusesBackground/context variables A binary indicator that the carer is of male gender An integer variable stating the carer’s age in years A categorical variable associating the carer with one of three marital statuses An integer count variable stating how many children the carer has A categorical variable identifying the carer’s country of orgin as Bangaldesh, India, or Pakistan An ordinal variable identifying the carer’s residential setting as city, town, or village
Results
This section presents the factor analysis interpretations and summarizes the analysis results. The technical details are reported in the Supplementary online Appendix.
Factor (treatment) interpretations
The loadings (Supplementary online Appendix, Table S-2) suggest that the treatments capture specific aspects of a carer’s pandemic experience. This section interprets the treatments by examining the relevant responses to two open-ended follow-up survey questions, ‘Please describe how this [your ability to give care] has changed [as a result of environmental changes or interruptions]’ and ‘Please describe how you feel about your caring role now?’ For each treatment, responses from carers for whom that treatment was positive but the other treatments were all zero are examined.
Treatment 1
Trapped
This treatment encodes the carer’s perception that the pandemic caregiving environment was socially confining. There were 43 respondents for whom was the only positive treatment. Some described the long hours they spent with the recipient and the curtailing of social outlets: I gave him a lot of time. I was always with him. Give him too much time. Unable to meet families and go out whenever need arises, need to be extra precautionary towards the situation.
Others expressed concern about the impact of isolation on the care recipient:
He is living in a flat nearby where we are allowed as we are also health care workers But, other visitors have restricted entry and this is limiting his social interaction greatly. The stage in dementia has advanced during Covid-19. Going to a daycare before this situation had somehow stabilized the condition.
Treatment 2
NoInfo
This treatment concerns the reduced availability of information (medical or non-medical) regarding the recipient. Information flows were sometimes impeded by poor communication with hospitals and other medical service providers (e.g. because those providers were overwhelmed by demand and/or discouraged non-essential visits), with the recipient or with others involved in the caregiving arrangements. Because of data limitations, no open-ended responses are available to aid in interpretation. Of the 48 carers for whom was positive, most also experienced other treatments. Only four carers had as the only positive treatment, none of whom responded to the open-ended questions
Treatment 3
NoConnect
This treatment captures the carer’s reduced intimacy and connection with the recipient. There were 27 respondents for whom was positive and the other treatments were all zero. Their open-ended responses confirmed that the COVID-19 containment measures limited visits and physical proximity to the recipient: Due to covid 19, I was not able to check his daily routine activities. Unable to visit her. But thankfully my sister is able to take care I take utmost precautions to maintain respiratory hygiene and social distancing while communicating with the concerned person now
Treatment 4
NoVisit
This treatment concerns lack of visitation rights. There were nine respondents for whom was the only positive treatment. While three of them did their caregiving at a facility, six (a plurality) did so at the recipient’s residence. The open-ended responses suggest that while some carers regarded the curtailment of in-person visits as mandatory (i.e. in response to lockdown regulations), there may have been other reasons for the reduced contact (e.g. to protect a vulnerable family member from exposure).
Number of visits becomes lesser and timing becomes short per session
Becauz of lockdown cause covid19
Due to covid visits have lessen
Treatment 5
PClothing
This treatment concerns one environmental change, the need to wear protective clothing. There were eight individuals for whom was the only positive treatment. Half of them did their caregiving in a facility. The open-ended responses confirm that mask-wearing had an outsized impact on residents. … need to wear mask all the time, residents will un co-operative towards care some times, challenges in their personal care, maintain social distance also some times cause agitation behavior Social distancing, using masks – This leading to un co-operative behaviors from the residents.
Summary of findings
Table 2 summarizes the empirical tests. Two of the five treatments, and , consistently increased both burden change and pandemic burden. Across all four tests, increased pandemic burden, but did not influence burden change. Overall, the and effects were either inconsistent or insignificant.Table 2.Summary of the test results. Basic (1)PSM (2)PSM + EB (3)Paired -test (4)Overall (5)Panel A: Change in burden frequency +++++ +InsignificantInsignificantInsignificantInconsistent +++++ InsignificantInsignificantInsignificantInsignificantInsignificant InsignificantInsignificantInsignificantInsignificantInsignificant****Panel B: Pandemic burden frequency +++++ InsignificantInsignificantInsignificantInsignificantInsignificant +++++ +++++ ++InsignificantInsignificantInconsistent(1) In Columns 1–4, each test was either positive and significant (+) or insignificant.(2) In Column 5, the overall treatment effect was positive and significant if all four tests were positive and significant, insignificant if all four tests were insignificant, or inconsistent if the tests had more than one outcomes.
Discussion
This section interprets the empirical results, defines the concept of an Embedded Carer Support Strategy (ECSS), recommends specific caregiving interventions, suggests directions for future research, and summarizes the strengths and limitations of this study.
Interpretations
The analysis identified three changes in the pandemic caregiving environment that significantly influenced the burden. The first, , had a persistently negative impact on carer well-being, in keeping with prior research. During the pandemic, cohabiting carers were often confined with their recipients for extended periods, increasing stress. A Hong Kong study of 25 stroke survivor carers found that confinement increased dependency, exhaustion, verbal abuse, and lack of respite [93]. Similarly, a survey of 5,568 Pakistani carers linked the psychological toll of confinement to various demographic factors [94]. These and other findings [95,96] suggest that the containment measures severely disrupted the carers’ social lives.
The treatment also had persistent negative impacts on carer well-being. Burden was higher when pandemic conditions suppressed carer–recipient interactions. This finding agrees with previous research showing that pandemic conditions could reduce contact and closeness with the recipient [97], causing emotional difficulties for the carer [98]. Numerous studies report a negative association between carer well-being and care intensity [99,100]. A pre-pandemic study of dementia caregivers in eight European countries [101] found that the burden decreased significantly after the recipient had been institutionalized. However, the results imply a more complex interplay, in which the burden rose when the pre-pandemic intensity (the equilibrium level) was ‘forced’ to change (increase or decrease) in undesirable ways. Further research is needed.
The treatment affected pandemic burden but not changes in burden. It mainly concerned recipients in facilities or separate households. To prevent contagion, care facilities worldwide took extraordinary measures to protect residents [102]. Carers were often denied visitation rights [103], contravening South Asian cultural expectations that family carers remain involved [104–106]. For dementia patients, Information and Communication Technology (ICT) was an inadequate substitute, reducing emotional closeness with carers [103].2^2^Chu, Yee, and Stamatopoulos [132] identified four barriers to ICT effectiveness: lack of technology, remote scheduling issues, poor implementation, and unsuitability for residents.
Carers of recipients in separate households may have perceived a ‘loss of rights’ when visits were discouraged due to mobility restrictions, contagion risks, or community objections [18]. Fear of community spread was significant; in some cases, healthcare workers faced hostility, even violence, from residents [2,18]. In this climate, non-cohabiting carers may have hesitated to visit recipients in other neighborhoods.
The treatment was found to have a hidden impact: although it caused higher burden during the pandemic, carers were not conscious of its transitional effect. They may have coped by cognitively disengaging – mentally withdrawing or avoiding thoughts about the loss of visitation [107], a strategy common when stressors feel beyond an individual’s control [108].
Previous research suggests that the treatment, reflecting a lack of information about the recipient, should have increased the burden. During the peak contagion, overwhelmed South Asian hospitals prioritized COVID-19 cases, disrupting medical communications with non-COVID patients. Healthcare quality declined, with Raman et al. [59] finding that residents in India’s COVID-19 ‘red zones’ rated medical services as less affordable (OR = 1.917), accessible (OR = 2.458), adequate (OR = 3.015), appropriate (OR = 2.225), and/or continuous (OR = 6.756). Mobility restrictions further limited flows of medical and non-medical information, especially to non-cohabiting carers. However, although the data suggest a link between burden and information, the number of observations treated by alone was too small to support a conclusion. Further study is warranted.
The treatment had an insignificant impact. Open-ended responses suggest that the negative effects mainly impacted carers of residents at facilities, where mask mandates caused behavioral issues. Studies find that PPE could be hot and uncomfortable and weaken carer-recipient closeness [13]. However, South Asian carers may have prioritized other pandemic-related challenges over the PPE requirements.
Embedded carer support strategies
The COVID-19 pandemic underscored the need of governments to prepare for future public health crises. Part of the preparation is supporting informal carers when their mobility is restricted and/or they cannot access essential services in the usual way. The next section presents specific measures that could work under such conditions. It prioritizes
- Mitigation of the stressors identified in the analysis (social isolation resulting from overexposure to the recipient and disrupted access to the recipient).
- Compatibility with existing public health structures.
- Efficient use of resources.
- Respect for South Asian cultural norms.
The guiding principle, that caregiving policies should align with cultural and socioeconomic constraints, is summarized in the notion of an Embedded Carer Support Strategy (ECSS): An Embedded Carer Support Strategy is a public health intervention designed to reduce the emotional burden of caregivers by integrating sustainable support mechanisms within existing healthcare, social, and community structures.
Recommended caregiving interventions
The carers’ primary needs are counseling and emotional support. This section describes a counseling program that would operate under a national healthcare system.
Recommendation #1: Counseling will be made accessible via ICT, ensuring that (1) the program functions during lockdowns, and (2) it accommodates carers who are homebound (e.g. because of caregiving duties or conservative family expectations [109]). India’s Tele-MANAS hotline demonstrates that ICT is an effective way to deliver mental health services. Tele-MANAS, established in 2022, now handles 3,500 calls per day, on average [110].
The ICT platform will accommodate heterogeneous client devices. Increasing numbers of South Asians are internet-connected via smartphones and/or laptops [111–113]. These individuals will be able to book video consultations through digital platforms such as India’s government-administered portal, Ayushman Bharat Digital Mission (ABDM) [114] or Pakistan’s Sehat Kahani, a private tele-health platform that partners with the government [109,115].
Currently, 85% of Indians have access to mobile phones [111], but not necessarily smartphones. The figures for Bangladesh and Pakistan are similar [112,113]. This suggests that an SMS link to counseling services is needed. The link would be activated through a missed call: the user would dial a dedicated number, immediately hang up, and wait for a callback.3^3^In India, many apps are activated in this manner [133]. For example, India’s Aarogya Setu, a mobile phone-based COVID-19 tracker, included a health self-rating app that could used missed call activation [134]. The counseling center would generate SMS acknowledgement and schedule notification messages. At the appointed time, the counselor would call the client, and the session would begin.
Multimedia (video+audio) group therapy sessions could be hosted with the help of a VoIP-Based platform (e.g. Microsoft Teams) with a dedicated phone number [116].
Recommendation #2: Two types of counselors will be employed. The first are mentors, experienced carers who offer advice on problems concerning caregiving. The second are spiritual advisors, religiously affiliated individuals (e.g. imams, pandits, or pastors), or other specialists who give guidance/support concerning the illness/loss of a loved one.
South Asian culture requires that counselors be of the same gender as their clients [117]. Most one-on-one counseling will therefore be done by women. Male counselors may play larger roles in group sessions.
As in Tele-MANAS [118], counselors will be able to refer clients to specialists (e.g. psychiatrists). All counselors will be trained/certified in caregiving issues, including social isolation, forced separation from the recipient, and family disputes.
Recommendation #3: A minority of South Asians have neither cell phones nor internet access. During a lockdown, these individuals would lack access to counseling services. The government can promote the availability of low-cost, basic phone models for these carers.
Recommendation #4: The effects of South Asia’s digital divide are concentrated among women [119] and the poor [120], who are less likely to have mobile phones and/or internet access. South Asian governments traditionally aid poor and underserved groups through community health workers (CHWs) [121–126]. These are community residents, predominantly women, who perform outreach to individual households. During the pandemic, CHWs were the front-line providers of healthcare and psychosocial support [127]. The counseling program will employ them to tutor clients in basic digital skills. This program could be modeled on Internet Saathi [128], an industry-sponsored program that recruited female volunteers to teach digital literacy skills among women in rural Indian communities.
Recommendation #5: A public health messaging program can be established to raise consciousness concerning the needs of carers. The program will deliver carer-friendly content to viewers. It will feature advice from expert speakers and testimonials (anonymous and non-anonymous) describing real-life challenges faced by carers and their families. The program will present thought-provoking cases involving issues such as sharing caregiving responsibilities within the home, social isolation among carers, ‘no-visit’ situations, and family conflicts. It will be broadcast on TV or radio at regularly scheduled times.
Future research
This paper suggests that during the pandemic, specific changes in the caregiving environment negatively affected carer emotional well-being. Three treatments stood out for their significant impacts: , reflecting social isolation and overexposure to the care recipient, and , reflecting lack of access/lack of intimacy with the care recipient, and , reflecting loss of visitation rights. Further research is needed to examine these environmental impacts in greater detail. In particular, qualitative analyses could reveal the pathways through which they affect carers in different cultural settings.
Strengths and limitations
A key strength of this study is its methodology. Factor analysis identified five dimensions of pandemic-induced caregiving change, while treatment effects analysis measured their impacts on carer emotional health, revealing the most burdensome changes. Another strength is the focus on South Asian carers, an underrepresented group with distinct socioeconomic caregiving challenges.
The study also has limitations. The retrospective, self-reported survey data may have introduced recall bias and subjective interpretations of burden. The results must be interpreted with caution because of the small sample size in some analyses. The sample is predominantly affluent and well-educated, potentially limiting the generalizability of the findings to the broader South Asian carer population. Although the respondents were predominantly unpaid family carers, some of them may have been paid. Sample weighting was not employed to compensate for the high representation of Pakistani carers (47%) within the sample. Confirmation bias may have influenced the selection of qualitative responses during the interpretation of the identified factors.
Conclusion
Early in the pandemic, South Asian governments adopted lockdowns, mobility restrictions, and school/work closures, which were standard, globalized responses to COVID-19 contagion [57]. Informal carers underwent emotionally costly adjustments, driven by changes in the local caregiving environment. This study identified five change dimensions (treatments) and estimated the emotional costs of each. Social isolation and separation from the recipient, which caused caregiving intensity to deviate from its pre-pandemic level, were found to increase emotional costs. These findings add to the limited evidence on caregiving in LMICs.
Caregiver burden reflects increasing demands on the carer that lead to emotional strain and self-diminishing values [69]. Our study raises the hope that in future crises, public health interventions will mitigate this private emotional suffering among South Asian carers. Using currently available resources, counseling services could be offered either in person during normal times or remotely (e.g. by phone) during a crisis.
In households throughout the globe, carers provide unpaid assistance and support to vulnerable dependents. They meet the needs of their recipients and assume burdens that might otherwise be handled at public expense. The informal care system will be sustainable only if individual carers remain willing to engage in this work. Carer distress is a public health concern, contributing to burnout and the breakdown of home care arrangements [129]. Informal care is both a public good and an extension of national health systems [24,99]. No society, even the wealthiest, can afford to replace its unpaid carers with hired health workers [130].
Supplementary Material
Table S2_Factor_loadings.docx
Table S3_Partition_of_the_sample.docx
Table S1_Self_reported impacts on the caregiving environment 2.docx
Table S4_Sample_statistics_CLEAN.docx
Table S5_Empirical_tests.docx
Figure S1_Smoothed Treatment 2 Effect Curves.docx
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Parkinson A, Matenge S, Desborough J, et al. The impact of COVID-19 on chronic disease management in primary care: lessons for Australia from the international experience. Med J Aust. 2022;216:445–16. doi: 10.5694/mja 2.5149735403236 PMC 9114997 · doi ↗ · pubmed ↗
- 2Venkata-Subramani M, Roman J. The coronavirus response in India - world’s largest lockdown. Am J Med Sci. 2020;360:742–748. doi: 10.1016/j.amjms.2020.08.00232892981 PMC 7405894 · doi ↗ · pubmed ↗
- 3Akhtar H, Afridi M, Akhtar S, et al. Pakistan’s response to COVID-19: overcoming national and international hypes to fight the pandemic. JMIR Public Health Surveill. 2021;7:e 28517. doi: 10.2196/2851733877048 PMC 8136406 · doi ↗ · pubmed ↗
- 4Hashim A. ‘Smart lockdown’ in Pakistan to target 500 coronavirus hotspots. Al Jazeera [Internet]. 2020 [cited 2025 Feb 13]; Available from: https://www.aljazeera.com/news/2020/6/23/smart-lockdown-in-pakistan-to-target-500-coronavirus-hotspots
- 5Ahmed T, Musarrat P, Kabir ZN. Lessons learned from pandemic response to COVID-19 in Bangladesh: NGO-based emergency response framework for low- and middle-income countries. BMC Health Serv Res. 2023;23:656. doi: 10.1186/s 12913-023-09643-w 37340495 PMC 10283326 · doi ↗ · pubmed ↗
- 6VHA Home Health Care. Face masks and dementia care [internet]. Toronto: VHA Home Health Care; 2020 [cited 2025 Feb 5]. Available from: https://www.vha.ca/blog/face-masks-and-dementia-care
- 7Pearl B, Hunter L, Lo K, et al. The enforcement of COVID-19 stay-at-home orders [internet]. Washington, D.C: American Progress; 2020 [cited 2025 Feb 6]. Available from: https://www.americanprogress.org/article/enforcement-covid-19-stay-home-orders/
- 8Zhou X, Song Y, Jiang H, et al. Comparison of public responses to containment measures during the initial outbreak and resurgence of COVID-19 in China: infodemiology study. J Med Internet Res. 2021;23:e 26518. doi: 10.2196/2651833750739 PMC 8023317 · doi ↗ · pubmed ↗