The emergence of common health conditions across the life course: evidence from the Born in Bradford family cohort
Gillian Santorelli, Dan Lewer, Krishnarajah Nirantharakumar, Siang Ing Lee, Katherine Phillips, Rosemary R.C. McEachan, John Wright, Nusrat Husain, Gillian Santorelli, Syed Masud Ahmed, Gillian Santorelli

TL;DR
A study of nearly 10,000 mothers in Bradford found that South Asian women had higher rates of diabetes and liver disease but lower rates of cancer and mental health disorders compared to White European women.
Contribution
The study provides new evidence on ethnic differences in the incidence of 21 health conditions using longitudinal health records from a large family cohort.
Findings
South Asian women had higher incidence of diabetes, chronic liver disease, and thyroid disorders compared to White European women.
South Asian women had lower incidence of cancer, mental health disorders, and neuromuscular conditions compared to White European women.
Differences in health conditions may be influenced by social, cultural, lifestyle, environmental, and genetic factors.
Abstract
Born in Bradford (BiB) is a family cohort study with linked routine health records. We calculated the rates of common health conditions and explored differences between White European and South Asian participants. 21 health conditions were identified using diagnostic codes and prescription records extracted from electronic health records. Period prevalence of each condition was calculated for the two years before recruitment, and incidence rates per 1000 person years were calculated from recruitment to BiB to the end of 2021, or earlier if censored. Age-adjusted Cox proportional hazard models were used to estimate hazard ratios (HR) between ethnic groups. The sample included 9,784 mothers, 52% of whom were of South Asian heritage and 48% were White European. The highest prevalence and incidence rates were observed for common mental health disorders and eczema. We found evidence that…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
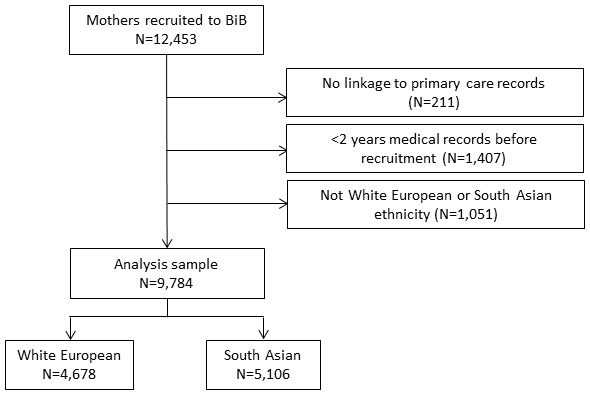 Figure 1
Figure 1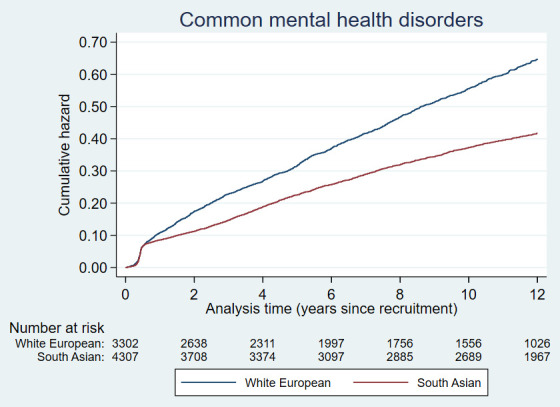 Figure 2a
Figure 2a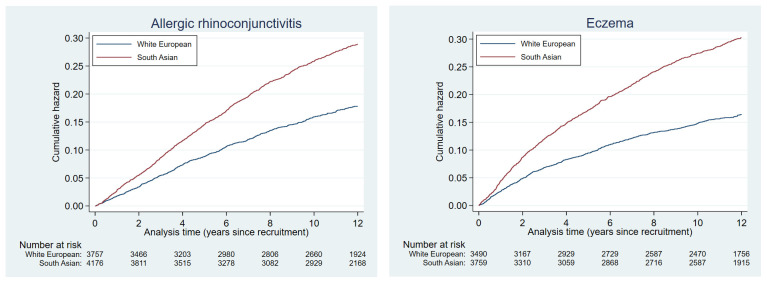 Figure 2b
Figure 2b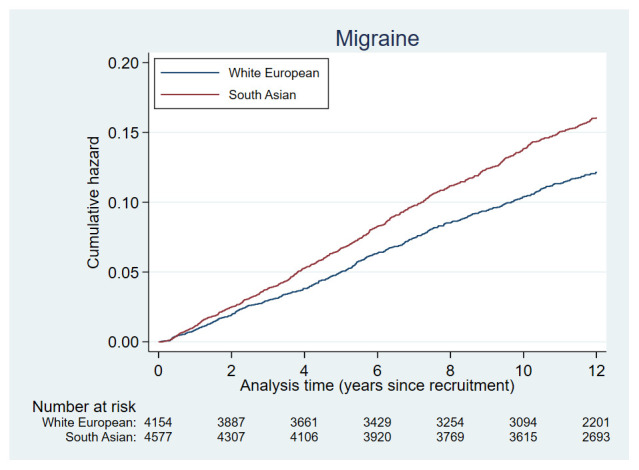 Figure 2c
Figure 2c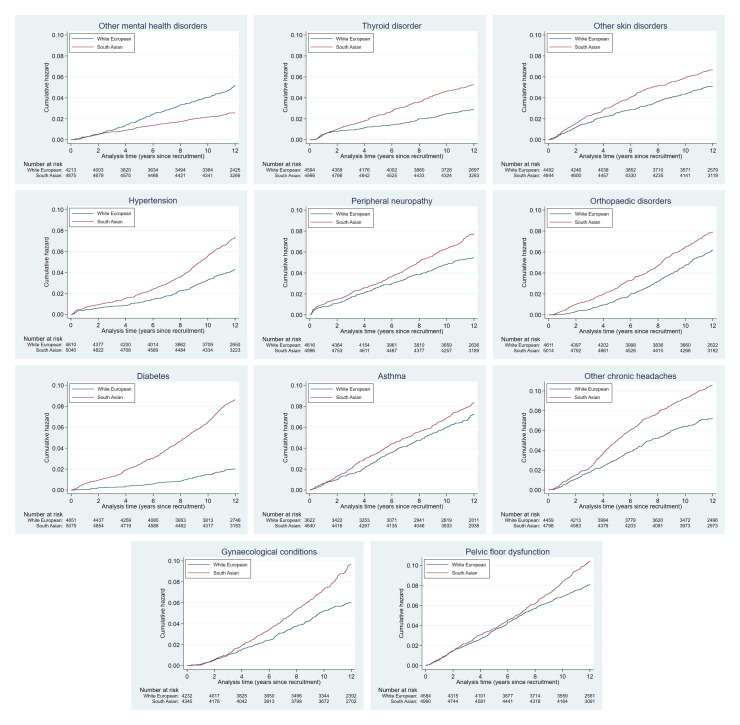 Figure 2d
Figure 2d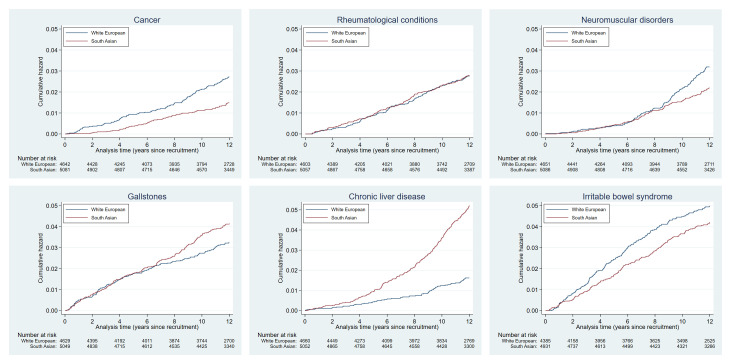 Figure 2e
Figure 2e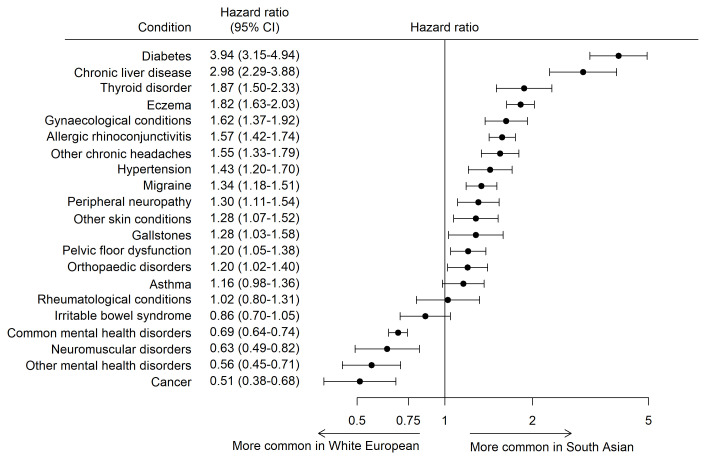 Figure 3
Figure 3| Health condition | Conditions included (where
| Definition |
|---|---|---|
| Cancer | - All cancers | Diagnosis code |
| Hypertension | N/A | Diagnosis code |
| Eczema | N/A | Diagnosis code
|
| Other skin disorders | - Seborrheic dermatitis
| Diagnosis code |
| Allergic rhinoconjunctivitis | - Allergic rhinitis (hay fever)
| Diagnosis code
|
| Irritable bowel syndrome | N/A | Diagnosis code |
| Chronic liver disease | - Chronic hepatitis B & C
| Diagnosis code |
| Gynaecological disorders | - Polycystic ovarian syndrome
| Diagnosis code |
| Pelvic floor dysfunction | - Urinary incontinence
| Diagnosis code |
| Rheumatological
| - Systemic lupus erythematosus
| Diagnosis code |
| Orthopaedic conditions | - Scoliosis
| Diagnosis code |
| Migraine | N/A | Diagnosis code |
| Other chronic headaches | - Tension-type headaches
| Diagnosis code |
| Peripheral neuropathy | N/A | Diagnosis code |
| Asthma | N/A | Diagnosis code
|
| Gallstones | N/A | Diagnosis code |
| Diabetes | - Type 1 diabetes
| Diagnosis code
|
| Thyroid disorders | - Hyperthyroidism
| Diagnosis code |
| Other neuromuscular disorders | - Chronic fatigue syndrome/
| Diagnosis code |
| Common mental health
| - Depression
| Diagnosis code
|
| Other mental illness | - Obsessive compulsive disorder
| Diagnosis code |
| Characteristic | All
| White European
| South Asian
|
|---|---|---|---|
| Year of recruitment, n (%) | |||
| 2007 | 2,286 (23.4) | 1,076 (23.0) | 1,210 (23.7) |
| 2008 | 2,740 (28.0) | 1,276 (27.3) | 1,464 (28.7) |
| 2009 | 2,617 (26.7) | 1,239 (26.5) | 1,378 (27.0) |
| 2010 | 2,141 (21.9) | 1,087 (23.2) | 1,054 (20.6) |
| Age at recruitment, mean (SD) | 27.7 (5.7) | 26.8 (6.1) | 28.5 (5.1) |
| BMI, kg/m 2, mean (SD) | 26.2 (5.7) | 26.6 (6.0) | 25.8 (5.5) |
| Missing, n (%) | 1,791 (18.3) | 807 (17.3) | 984 (19.3) |
| Smoked during pregnancy, n (%) | |||
| No | 7,033 (71.9) | 2,787 (59.6) | 4,246 (83.2) |
| Yes | 1,573 (16.1) | 1,408 (30.1) | 165 (3.2) |
| Missing | 1,178 (12.0) | 483 (10.3) | 695 (13.6) |
| IMD, n (%) | |||
| 1 (most deprived) | 6,364 (65.0) | 2,452 (52.4) | 3,912 (76.6) |
| 2 | 1,775 (18.1) | 1,004 (21.5) | 771 (15.1) |
| 3 | 1,120 (11.4) | 782 (16.7) | 338 (6.6) |
| 4/5 (least deprived) | 466 (4.8) | 416 (8.9) | 50 (1.0) |
| Missing | 59 (0.6) | 24 (0.5) | 35 (0.7) |
| Health condition | Prevalence % | IR/1000
| ||
|---|---|---|---|---|
| White European
| South Asian
| White European
| South Asian
| |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
- —Medical Research Council
- —UK Prevention Research Partnership
- —British Heart Foundation
- —Wellcome
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiversity and Career in Medicine · Global Health Care Issues · Retirement, Disability, and Employment
Introduction
Bradford is a city in West Yorkshire, England. It has a young population; high levels of deprivation, being the 13 ^th^ most deprived local authority out of 317 in England, with almost a fifth of children living in low income families ^ 1 ^; and ethnic diversity, with 57% identifying as White British and 26% of Pakistani heritage ^ 2 ^. Concerns over the high rates of illness in Bradford led to the establishment of the Born in Bradford (BiB) cohort study, which aims to examine how socio-economic, environmental, behavioural, and genetic factors influence development, health, and wellbeing. The study recruited 12,453 women over 13,776 pregnancies between 2007 and 2010, resulting in 13,858 births ^ 3 ^.
The mothers recruited to the BiB cohort are now reaching middle age, thus providing a unique opportunity to understand accumulation of health conditions postpartum in women. The aim of this study was to (1) describe rates of common health conditions in mothers participating in the BiB cohort study; and (2) determine if there were any differences in incidence of health conditions between the two largest ethnic groups in Bradford.
Methods
Participants and data sources
We used research data and linked primary care electronic health records (EHR) from mothers participating in the Born in Bradford birth cohort study. Informed consent was provided at recruitment for data collection and linkage to their routine health care records. Information on demographic variables was obtained from the BiB baseline questionnaire. Primary care data was extracted from SystmOne, a clinical computer system which stores electronic health records and is used by all GP practices in Bradford.
Outcomes
We identified several health conditions that could plausibly affect individuals within the same age range as our participants, and searched EHR for relevant diagnostic codes and prescriptions. Following exploratory analysis of the incidence of various health conditions, we report trends for 21 health conditions (19 physical and 2 mental health) with an incidence per 1000 person-years ≥2% in either ethnic group. Many of the 21 health conditions reported included several other conditions; see Table 1 for details and definitions.
Ethnicity
Information on ethnicity was obtained from research questionnaires and routine data sources, all of which were self-reported by the participant and categorised using the same classification as the 2001 UK census ^ 4 ^. White European ethnicity included those who identified as White British, Irish, Gypsy/Irish traveller, and White Other; South Asian ethnicity was assigned to participants of Pakistani, Indian, and Bangladeshi heritage.
Ethics statement
Ethics approval for the Born in Bradford study was granted by the National Health Service Health Research Authority Yorkshire and the Humber (Bradford Leeds) Research Ethics Committee (reference: 07/H1302/112, date of approval 01/04/2008). Informed consent for data collection and linkage to routine healthcare records was provided by participants at recruitment to the BiB cohort study. Further information on our privacy policy can be found here: https://borninbradford.nhs.uk/privacy-policy/.
Statistical analysis
To ensure we had sufficient medical records to identify prevalent conditions, we excluded participants if they had less than 2 years-worth of medical records before recruitment. The period prevalence for each health condition was defined as those who had a GP-recorded diagnostic code or relevant medication prescribed at any time in the two years before recruitment (“time 0”). Prevalence was calculated separately for each ethnic group and is reported as percentages. Incidence rates per 1000 person years (IR/1000) was calculated from the date of recruitment, with participants censored at the date of the last GP event up to 31 ^st^ December 2021, or at the date they withdrew from the study, moved out of the area, or died. Prevalent cases were not included in the denominator when calculating incidence. For the main condition categories, an age-adjusted Cox proportional hazards model was used to calculate hazard ratios (HR) to estimate the differences in the risk of developing each health condition between White European and South Asian participants, with White European as the reference. HR were not estimated for the individual conditions combined into each main category due to small numbers. Analyses were conducted using Stata/SE version 17 software ( https://www.stata.com/).
Results
The sample comprised 9,784 mothers, of whom 52% were of South Asian ethnicity; see Figure 1 for further details of the sample selection, and Table 2 for participant characteristics.
Sample flow chart.
Prevalence and IR/1000 are presented in Table 3. The conditions with the highest prevalence in White European and South Asian women were common mental health disorders (29.3% vs 15.7% respectively), eczema (25.3% vs 26.4%), and asthma (22.5% vs 9.1%). The highest IR/1000 was for common mental health disorders (55.9 vs 35.4 in White European and South Asian women respectively). High IR/1000 was observed in South Asian women for eczema, allergic rhinoconjunctivitis and migraine. Of the individual health conditions combined into larger categories, the IR/1000 were statistically significantly higher in White European compared to South Asian for fibromyalgia, endometriosis, genital prolapse, and all conditions included in common and other mental health disorders apart from dissociative disorders. South Asian women had higher rates of hypothyroidism, seborrhoeic dermatitis, lichen planus, systemic lupus erythematosus, back pain, osteoarthritis, polycystic ovarian syndrome, uterine fibroids, infertility, urinary incontinence, and all conditions included in other chronic headaches.
Plots of the cumulative hazards of the health condition examined are presented in Figure 2a to Figure 2e and show the different patterns of the conditions over time by ethnic group. Some had very similar trajectories over the whole study period (rheumatological and orthopaedic conditions, cancer, irritable bowel syndrome and asthma); some showed ethnic divergence from the birth of the BiB child (eczema, allergic rhinoconjunctivitis); some conditions diverged in the early years (other skin, thyroid and gynaecological disorders, migraine/other headaches, diabetes); whilst others diverged between 7 – 10 years after recruitment (gallstones, hypertension, peripheral neuropathy, pelvis floor dysfunction and neuromuscular disorders). The increasing divergence in the rate of common mental health disorders in WE compared to SA women was apparent shortly after recruitment, whereas other mental health disorders had a similar trajectory in both ethnic groups until 2 – 3 years after recruitment before increasing more rapidly in WE women.
Health conditions with a cumulative hazard >30%.
Health conditions with a cumulative hazard of 21% to 30%.
Health conditions with a cumulative hazard of 11% to 20%.
Health conditions with a cumulative hazard of 6% to 10%.
Health conditions with a cumulative hazard 2% to 5%.
The HRs for each health condition are shown in Figure 3. Cancer (HR 0.53 [95%CI 0.40, 0.70]), other mental health disorders (HR 0.56 [95%CI 0.44, 0.70]), neuromuscular disorders (HR 0.63 [95%CI 0.49, 0.82]) and common mental health disorders (HR 0.69 [95%CI 0.64, 0.74]) were more common in White European mothers. South Asian mothers were at statistically significantly higher risk of developing 14 out of the 21 health conditions, with diabetes (HR 3.92 [95%CI 3.13, 4.91]) and chronic liver diseases (HR 2.98 [95%CI 2.29, 3.88]) have the largest hazard ratios.
Age-adjusted hazard ratios with 95% CI for common health conditions in South Asian and White European women (White European is the reference).
Discussion
Main findings
This study describes the prevalence and incidence of 21 common health conditions in mothers participating in the Born in Bradford cohort before and after recruitment and explores differences in the risk of conditions in women of White European and South Asian heritage. Mental health and atopic disorders were the most common health conditions in both ethnic groups. The risk of developing 14 of the 21 health condition was statistically significantly higher in South Asian mothers, with diabetes and chronic liver disease having the greatest difference, at four and three times higher compared to White European women. White European mothers were at higher risk of developing common and other mental health disorders, neuromuscular disorders, and cancer.
Ethnic inequality
** Mental health disorders.** The risk of common and other mental health disorders in South Asian women was 31% and 44% lower respectively than in White European women. Previous research on women participating in BiB found that although minority ethnic women self-report similar levels of psychological distress as White British women, they are less likely to access treatment and therefore have a GP-recorded diagnosis ^ 5 ^. It is therefore likely that the incidence of common mental health disorders in South Asian women is underestimated using health service data. An alternative explanation may be that stronger social networks evidence in South Asian women may protect against mental ill-health by provision of financial, social or emotional support ^ 6 ^.
** Diabetes mellitus.** We found that women of South Asian heritage were almost four times more likely to develop diabetes compared to White European women. This is comparable to other recent estimates reported in people aged between 40–69 ^ 7 ^, though the mean age of women by the end of our study was 40 years, suggesting that differential risk starts young and may yet be higher.
** Chronic liver diseases.** The development of chronic liver disease in South Asian-heritage women was three times higher than in White European participants, predominantly due to fatty liver disease. A recent systematic review and meta-analysis found that South Asian men and women have more fat in the liver compared to their White European counterparts despite having similar BMI levels ^ 8 ^. Although our primary care data did not categorically distinguish between the types of fatty liver disease, the high prevalence of non-alcoholic fatty liver disease (NAFLD) in South Asian-heritage people has been well documented and is associated with obesity, dyslipidaemia, diabetes, and hypertension ^ 9 ^, the latter two of which are also reported as being higher in South Asian women in our study.
** Thyroid disorders.** Women of South Asian heritage were at almost twice the risk of developing thyroid disorders compared to White European women, with hypothyroidism being the most common. Hypothyroidism can be caused by low iodine levels, and a study of almost 7,000 BiB mothers found that the urinary iodine-to-creatinine ratio was lower in Pakistani compared to White European participants ^ 10 ^. Another small multi-ethnic study of thyroid function in pregnancy found that women of South Asian heritage had higher levels of serum thyroid stimulating hormone (TSH) compared with ethnic Europeans despite having similar levels of iodine deficiency; a higher prevalence of subclinical hypothyroidism was also observed ^ 11 ^.
** Gynaecological disorders.** We also found that women of South Asian heritage had higher rates of uterine fibroids, infertility and polycystic ovarian syndrome compared to White European women but lower rates of endometriosis. Systematic reviews have reported that black ethnicity was a strong risk factor for uterine fibroids ^ 12 ^ although black women are less likely to be diagnosed with endometriosis ^ 13 ^. There is limited literature on the prevalence of these disorders in South Asian women apart from a small US-based study that found South Asian women had a similar prevalence of uterine fibroids as white women ^ 14 ^.
Reasons for ethnic inequality and clinical implications
The clear differences found in the incidence of most of the health conditions examined between ethnic groups could be explained by social, cultural, genetic or lifestyle factors ^ 15– 17 ^. There is a clear link between socioeconomic deprivation and poor health, and data from England – and in our own cohort – show that ethnic minorities experience higher deprivation compared to the white population ^ 15, 17 ^. Differences in lifestyle behaviours may also partially explain differences: whilst people of South Asian heritage are less likely to adopt some risky behaviours such as smoking and drinking alcohol, they are more likely to be physically inactive, have a poor diet, and have higher rates of obesity ^ 18 ^. Genetic and epi-genetic factors may also underlie the risk of some health conditions, such as diabetes (including worse diabetes-related outcomes in South Asian compared to White European people), cardiovascular health conditions, and insulin resistance ^ 19 ^. There is also evidence that people of minority ethnic groups are more at risk of allergic health condition and autoimmune disorders ^ 20 ^, and that the onset of these health condition occurs earlier in non-White compared to White groups ^ 21 ^.
Health inequalities are also evident with regards to health access and ethnic minority patients report poorer experience of healthcare services compared to White British groups ^ 18 ^. The uptake of population health screening is also lower in ethnic minorities and those living in deprived areas ^ 22 ^: screening rates for breast, cervical and bowel cancer are lower in South Asian. This is likely to extend to South Asian communities’ participation in other programmes that are effective in improvements in health condition like diabetes ^ 18 ^. A number of strategies to improve health literacy, together with cultural sensitivity and appropriateness in the healthcare setting have been recommended in an attempt to overcomes these barriers ^ 18, 22, 23 ^.
Strengths and limitations
Using electronic health records, we have assessed the prevalence, incidence, and ethnic differences in risk for a wide range of health conditions in a bi-ethnic sample of 9,784 women enrolled in a longitudinal cohort study. The large proportion of South Asian women in our sample (52%) allowed us to identify health inequalities in some conditions that have not previously been widely explored or reported. However, to enable us to identify prevalent conditions, we excluded women with less than 2 years-worth of medical records before recruitment. This cut-off was based on recorded GP events rather than being registered with GP and may have biased our estimates. Whilst it would have been interesting to examine incidence by area deprivation, the numbers were too small. Finally, the purpose of this study was to explore the level of health condition in the BiB cohort, so we acknowledge that the findings are Bradford-specific; however, they are likely to represent parous women in similar urban populations with high levels of deprivation and diversity.
Conclusion
In conclusion, our results highlight how non-communicable health conditions emerge across the life course from early adulthood, and how these differ between women of White European and South Asian heritage. The impacts of these health conditions on health services may be greatest in later adulthood, but the opportunity for prevention is greatest in early life. Tackling upstream modifiable risk factors at an individual level (diet, physical activity, smoking) and at a systems level (environment, housing, education, urban design) remains a crucial but neglected priority for improving long term health outcomes and reducing health service pressures ^ 24 ^.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Public Health England: Fingertips.Fingertips.phe.org.uk. Reference Source
- 2City of Bradford Metropolitan District Council: 2021 Census: Ethnic group, religion and language spoken. 2022. Reference Source
- 3Wright J Small N Raynor P : Cohort profile: The born in bradford multi-ethnic family cohort study. Int J Epidemiol. 2013;42(4):978–91. 10.1093/ije/dys 112 23064411 · doi ↗ · pubmed ↗
- 4Office for National Statistics: Ethnic group statistics: a guide for the collection and classification of ethnicity data.London: The Stationary Office, 2003; 2003. Reference Source
- 5Prady SL Pickett KE Petherick ES : Evaluation of ethnic disparities in detection of depression and anxiety in primary care during the maternal period: Combined analysis of routine and cohort data. Br J Psychiatry. 2016;208(5):453–61. 10.1192/bjp.bp.114.158832 26795424 PMC 4853643 · doi ↗ · pubmed ↗
- 6Uphoff EP Pickett KE Wright J : Social gradients in health for Pakistani and White British women and infants in two UK birth cohorts. Ethn Health. 2016;21(5):452–67. 10.1080/13557858.2015.1091442 26428034 · doi ↗ · pubmed ↗
- 7Farmaki AE Garfield V Eastwood SV : Type 2 diabetes risks and determinants in second-generation migrants and mixed ethnicity people of South Asian and African Caribbean descent in the UK. Diabetologia. 2022;65(1):113–127. 10.1007/s 00125-021-05580-7 34668055 PMC 8660755 · doi ↗ · pubmed ↗
- 8Iliodromiti S Mc Laren J Ghouri N : Liver, visceral and subcutaneous fat in men and women of South Asian and white European descent: a systematic review and meta-analysis of new and published data. Diabetologia. 2023;66(1):44–56. 10.1007/s 00125-022-05803-5 36224274 PMC 9729139 · doi ↗ · pubmed ↗