Clinical Images in Emergency Medicine: Man With Foot Pain and Indifference
Alex Y. Koo, Susan R. O’Mara

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2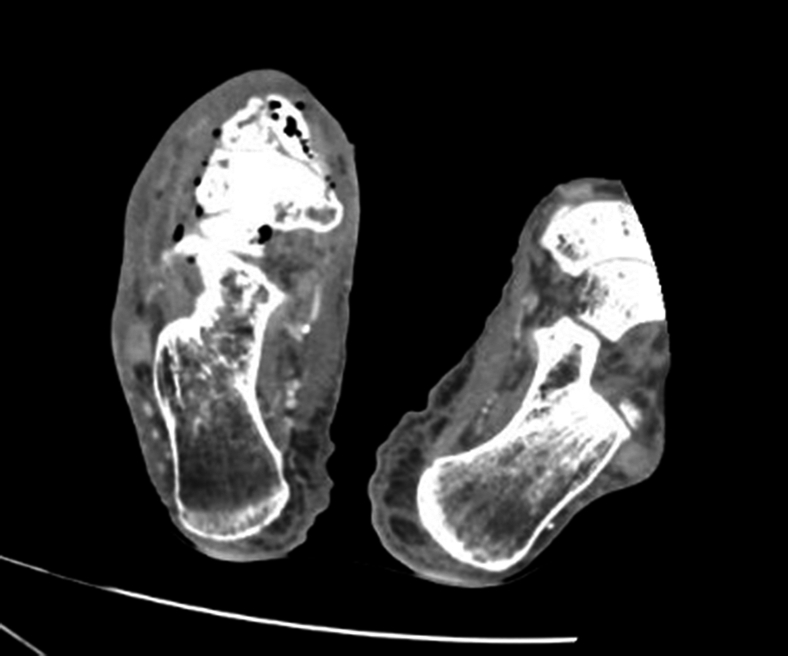 Figure 3
Figure 3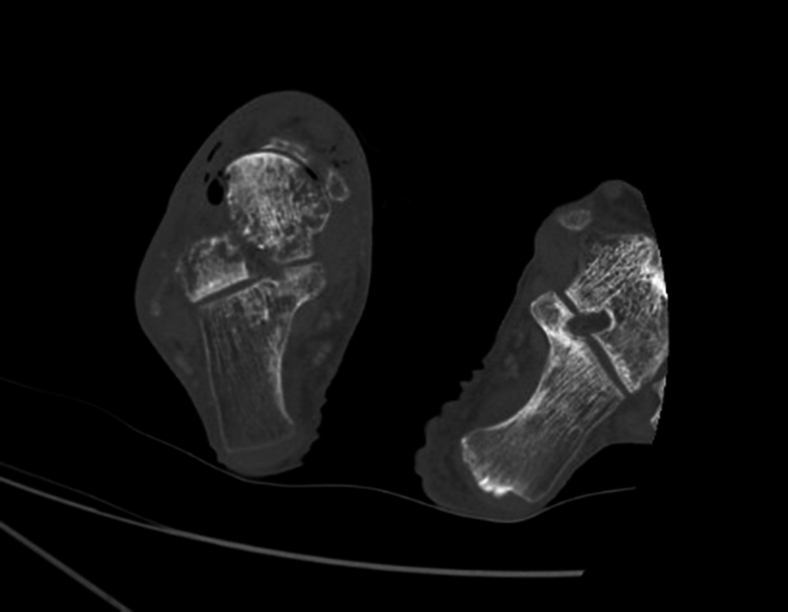 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStreptococcal Infections and Treatments · Hematological disorders and diagnostics · Otolaryngology and Infectious Diseases
Patient Presentation
An 83-year-old male with a history of hypertension and tobacco use presented with right foot pain of unclear duration, reporting its presence for “maybe a couple weeks – or two months.” He was alert and oriented with normal vital signs. Examination of the foot revealed areas of indurated tissue necrosis and hemorrhagic bullae that were minimally painful to touch (Figs 1 and 2). The patient seemingly was indifferent to the concerning appearance of his extremity asking, “Can I just get something for the pain and get out of here?”Figure 1. Right foot with wet and dry gangrene.Figure 2. Right foot with hemorrhagic bullae (red arrow).
Diagnosis: Necrotizing Soft Tissue Infection With Osteomyelitis of the Foot
Computed tomography revealed soft tissue gas of the hind- and midfoot and multifocal osteomyelitis involving the talar head and midfoot (Figs 3 and 4). He underwent right ankle disarticulation with deep tissue drainage culture that grew Morganella morganii.Figure 3. Axial computed tomography right lower extremity with air and stranding in deep tissues.Figure 4. Axial computed tomography right lower extremity with cortical destruction of talar and midfoot bones.
Early necrotizing soft tissue infections present with erythema, pain, and swelling, making it difficult to distinguish from cellulitis. As infection progresses, the blood supply of overlying skin is stripped, and erythema progresses to hemorrhagic bullae with extreme local tenderness.1 Hemorrhagic bullae have been cited to be >90% specific for a necrotizing soft tissue infection.2 Later stages will have appreciable crepitus and systemic signs of sepsis.
“La belle indifference,” defined as a paradoxical absence of distress despite a serious medical illness, has been described in a subset of patients with necrotizing infections.3 Although not well studied, it is theorized that anesthesia of the skin due to necrosis may attribute to this phenomenon.4
Funding and Support
By JACEP Open policy, all authors are required to disclose any and all commercial, financial, and other relationships in any way related to the subject of this article as per ICMJE conflict of interest guidelines (see www.icmje.org). The authors have stated that no such relationships exist.
Conflicts of Interest
All authors have affirmed they have no conflicts of interest to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kiat H.J.En Natalie Y.H.Fatimah L.Necrotizing fasciitis: how reliable are the cutaneous signs?J Emerg Trauma Shock 104201720521010.4103/JETS.JETS_42_1729097860 PMC 5663140 · doi ↗ · pubmed ↗
- 2Fernando S.M.Tran A.Cheng W.Rochwerg B.Necrotizing soft tissue infection: diagnostic accuracy of physical examination, imaging, and LRINEC score: a systematic review and meta-analysis Ann Surg 26912019586510.1097/SLA.000000000000277429672405 · doi ↗ · pubmed ↗
- 3Stone J.Smyth R.Carson A.Warlow C.Sharpe M.La belle indifférence in conversion symptoms and hysteria: systematic review Br J Psychiatry 188200620420910.1192/bjp.188.3.20416507959 · doi ↗ · pubmed ↗
- 4Raam R.Moran G.J.Jhun P.Herbert M.Worms and flesh-eating bacteria? The worst day of your life Ann Emerg Med 682201624524810.1016/j.annemergmed.2016.06.03027451305 · doi ↗ · pubmed ↗