The efficacy of non-complete omentectomy in the radical gastrectomy for gastric cancer: a meta-analysis and systematic review
Chenglong Gao, Wenchao Shi, Baoming Zhang, Qiang Tang, Huiyu Chen, Zengtao Bao

TL;DR
This study compares non-complete and complete omentectomy during gastric cancer surgery and finds similar outcomes, but suggests more research is needed.
Contribution
A meta-analysis and systematic review comparing non-complete and complete omentectomy in gastric cancer surgery.
Findings
NCO was associated with lower recurrence rates and fewer complications compared to CO.
NCO showed higher 3- and 5-year survival rates but no significant difference in lymph node harvest or peritoneal recurrence.
No significant advantage was found for NCO over CO in surgical, survival, or recurrence outcomes.
Abstract
Surgery is considered a necessary treatment for gastric cancer (GC), but the extent of resection remains controversial. This study aimed to evaluate the efficacy of non-complete omentectomy (NCO) in GC patients undergoing radical gastrectomy. We searched for studies of non-complete omentectomy versus complete omentectomy (CO) published before February 2024 from PubMed, Web of Science, and Cochrane Library databases. From the extracted clinical data, we compared surgical, survival, and recurrence outcomes between the two groups. Thirteen studies with a total of 4255 patients were included. The meta-analysis showed that compared with the CO group, the NCO group was associated with a lower overall recurrence rate, shorter operative time, and fewer postoperative complications. However, there was no significant difference in the number of harvested lymph nodes and peritoneal recurrence…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
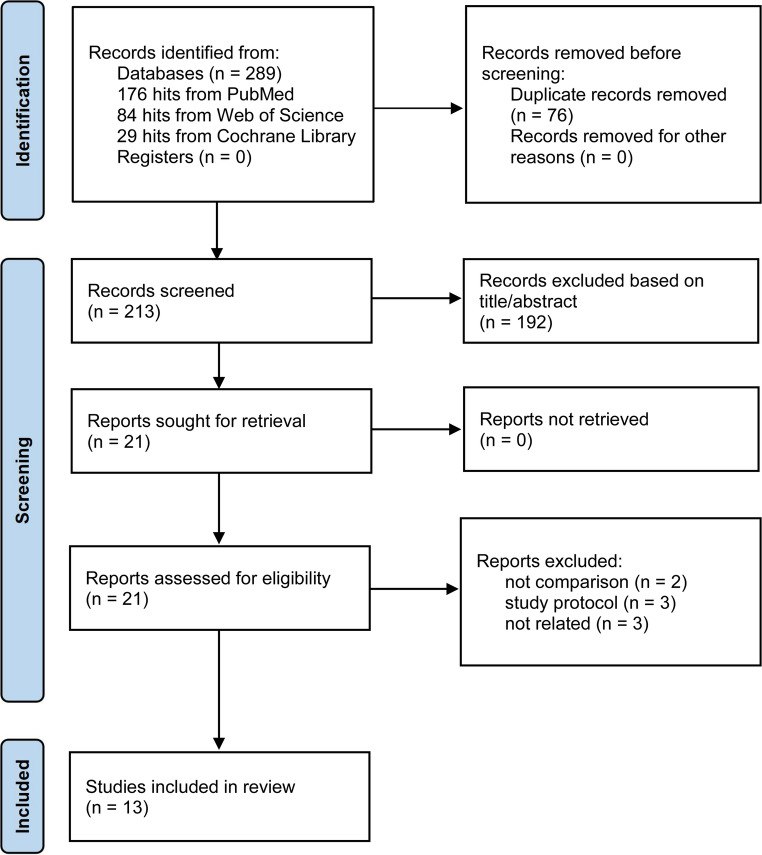 Figure 1
Figure 1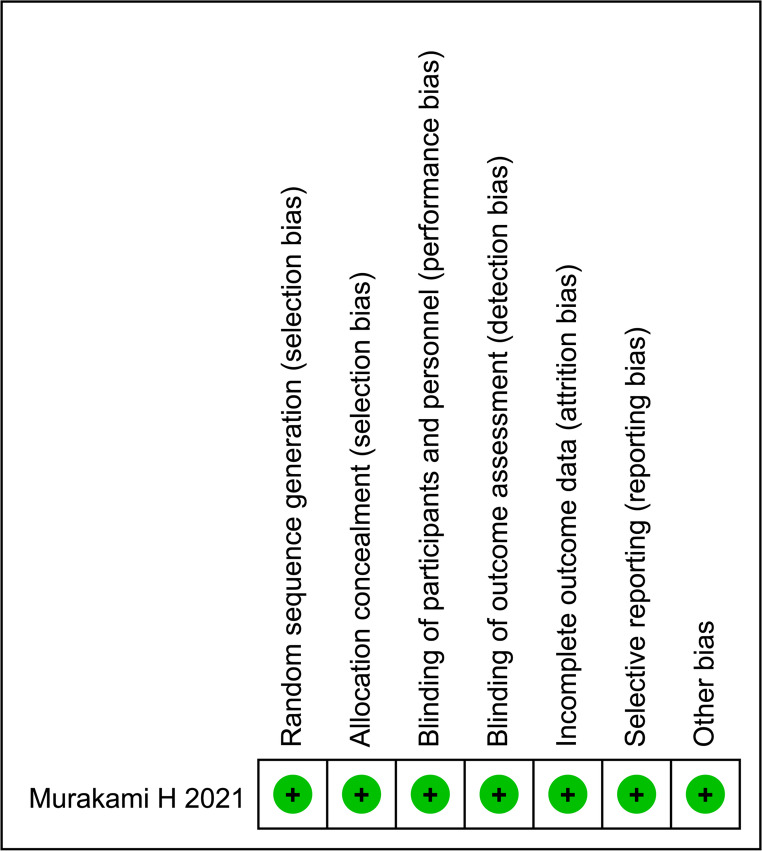 Figure 2
Figure 2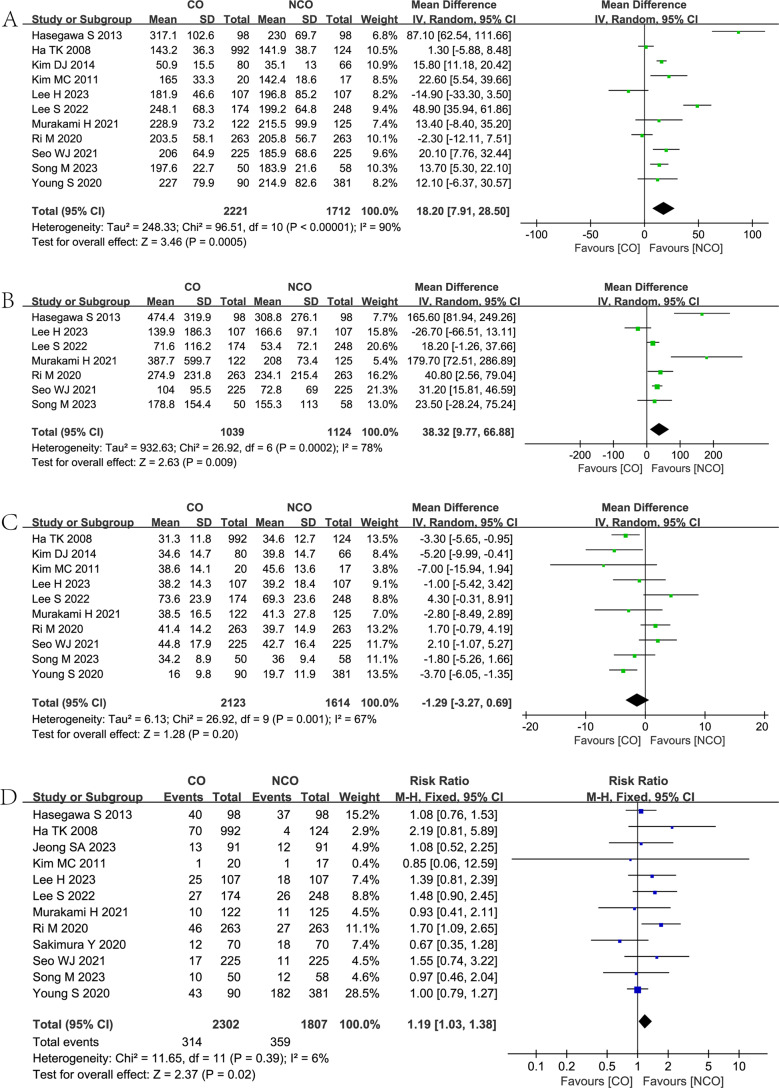 Figure 3
Figure 3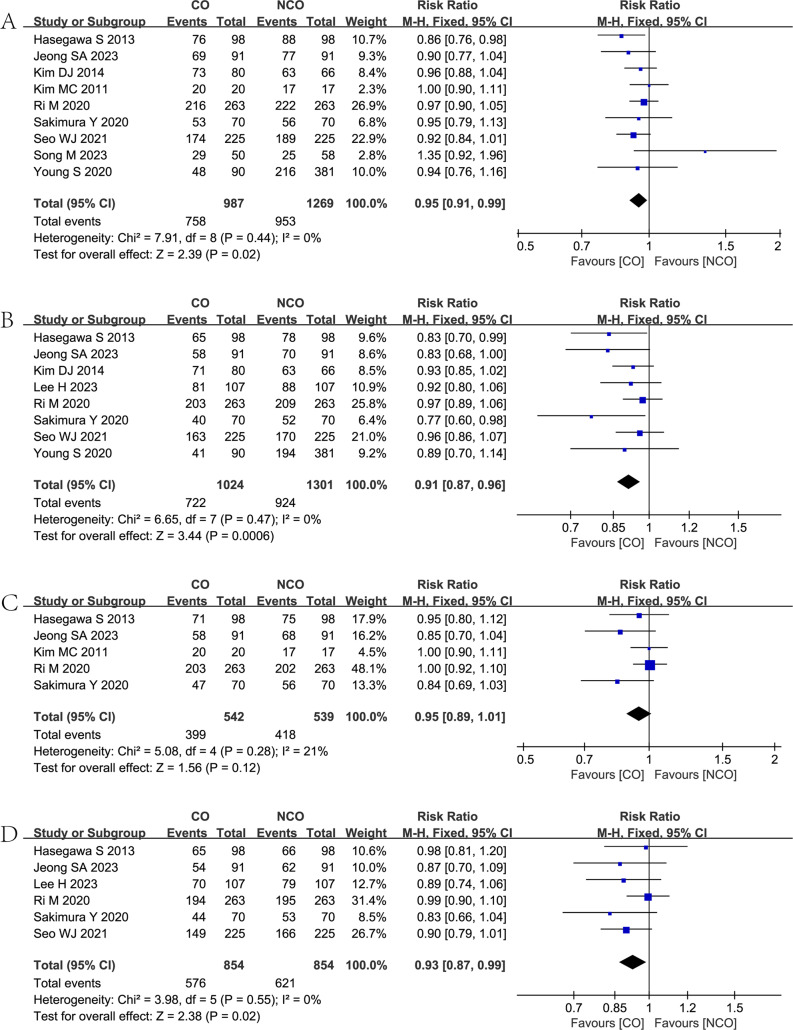 Figure 4
Figure 4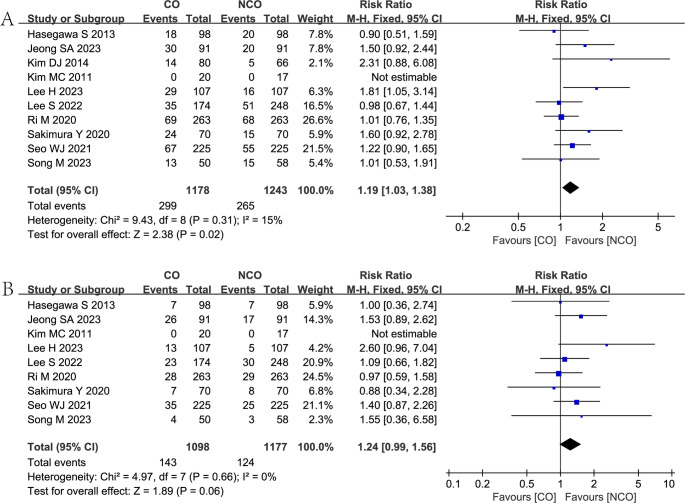 Figure 5
Figure 5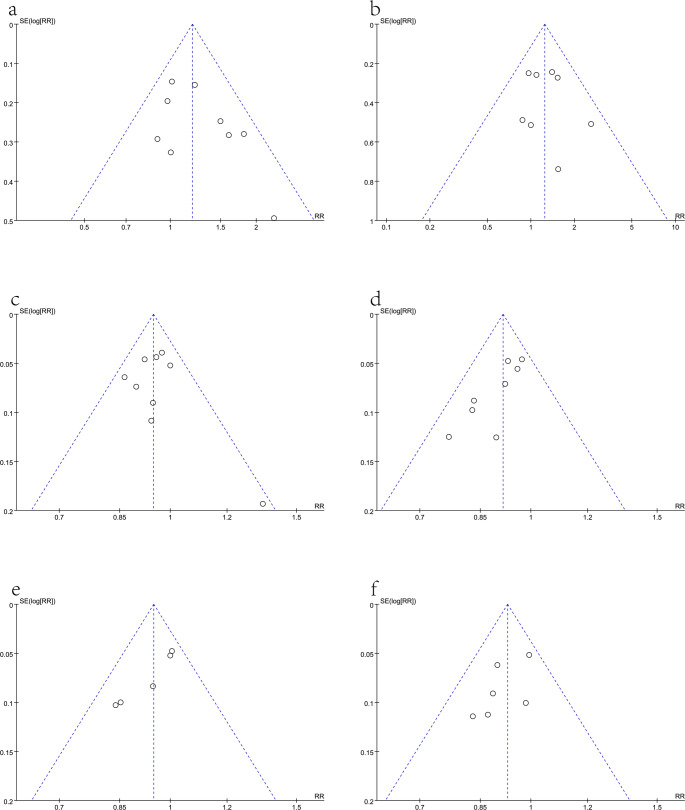 Figure 6
Figure 6- —Doctoral Research Foundation of Lianyungang First People’s Hospital
- —Youth Project of Lianyungang City Health Science and Technology Project
- —open research project of Jiangsu Key Laboratory of New Drug Research and Clinical Pharmacy
- —Lianyungang science and technology project
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Metastasis and carcinoma case studies · Gastrointestinal Tumor Research and Treatment
Background
Gastric cancer (GC) has become a great global human health hazard. According to GLOBOCAN 2020, it is the fifth most common malignant tumor and the fourth leading cause of cancer-related death in the world [1]. Meanwhile, GC has become the second most common cancer and the second leading cause of cancer-related deaths in China [2]. Compared with most developed countries, it has a higher incidence rate, mortality, and 5-year prevalence rate [2]. Radical gastrectomy remains the mainstay of treatment for resectable gastric cancer, although the efficacy of adjuvant radiotherapy, immunotherapy, and targeted therapy has been proven today [3].
There is still controversy about the extent of resection in radical cancer surgery. According to the Japanese gastric cancer treatment guidelines 2018 (5 th edition), resection of the greater omentum is recommended during standard gastrectomy for patients with T3 or deeper tumors [4]. For patients with T1/T2 GC, guidelines recommend that the omentum be preserved more than 3 cm from the gastroepiploic artery [4]. Meanwhile, total omentectomy for D1 and D2 gastrectomy is recommended by the Chinese Society of Clinical Oncology (CSCO) [5]. The available studies are mainly retrospective observational studies and the only randomized controlled trial (RCT) that analyzed the effects and outcomes of CO and NCO in radical gastrectomy [6–15]. Due to the significant bias in the abovementioned studies, several meta-analyses have previously been performed to statistically analyze the data in the literature [16–24], illustrating that NCO has similar or even better outcomes than CO in radical gastrectomy.
Based on the results of a recent literature search, we identified three new studies comparing CO and NCO for radical gastrectomy in patients with GC [25–27]. Therefore, our meta-analysis was conducted to update the existing evidence from the most recent study data comparing CO and NCO for outcomes of surgery, survival, and recurrence in radical gastrectomy.
Methods
This meta-analysis was carried out in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [28]. The study was registered on the PROSPERO database (CRD42023449075).
Search strategy
The PubMed, Web of Science, and Cochrane Library databases were systematically searched to investigate the efficacy of NCO versus CO in gastrectomy for GC. The specific search strategy was as follows:
Pubmed: (“gastric cancer” OR “gastric carcinoma” OR “stomach cancer” OR “gastric adenocarcinoma”) AND (“omentum” OR “omentectomy”) AND “gastrectomy”.
Web of Science: ((TS = (gastric cancer)) AND TS = (omentectomy)) AND TS = (gastrectomy).
Cochrane Library: gastric cancer in Title Abstract Keyword AND omentectomy in Title Abstract Keyword AND gastrectomy in Title Abstract Keyword.
There were no date or language restrictions in the search strategy. The latest recent search was conducted on 26 February 2024.
Study selection criteria
The inclusion criteria were as follows: [1] studies on patients undergoing radical gastrectomy for GC and comparing the use of CO and NCO during surgery; [2] the literature was required to provide one or more of the indicators of the patients’ 3-year or 5-year overall survival rate and relapse-free survival rate, postoperative complications, and recurrence of the tumor. The exclusion criteria for this study were as follows: [1] studies in the form of abstracts, animal experiments, case reports, letters, protocols, and reviews; [2] studies with incomplete or inaccurate data.
Data extraction
Two independent reviewers (CG and ZB) selected papers on the basis of title, abstract, and full text. The following data were extracted from the studies that met the criteria: first author, year of publication, study country, study period, study design, population size, characteristics of the study population, surgical approach, surgical procedure, operative time, estimated blood loss, number of harvested lymph nodes, postoperative complications, overall recurrence rate, peritoneal recurrence rate, 3-year and 5-year overall survival (OS) rates, and 3-year and 5-year relapse-free survival (RFS) rates. Conflicts of opinion encountered between authors were resolved by discussion. The results were checked by a third reviewer (WS).
Risk of bias assessment
For randomized clinical trials (RCTs), we used the Cochrane Risk of Bias tool [29], and for included observational studies, we used the Newcastle Ottawa Scale (NOS) [30]. NOS categorizes each observational study into stars ranging from 0 to 9 based on patient selection, comparability, and outcomes. A score ≥ 7 on the NOS scale indicated high-quality studies. Funnel plot analysis was used to detect publication bias when more than 10 studies were included.
Statistical analysis
Our meta-analysis was performed using Review Manager (RevMan) Version 5.4.1 software (Cochrane, London, UK). For dichotomous outcomes, the Mantel‒Haenszel (MH) method was used to calculate risk ratios (RR) and corresponding 95% confidence intervals (CI). In the case of continuous outcomes, mean differences (MD) and corresponding 95% CI were calculated according to the inverse variance method. When the mean or standard deviation (SD) of an endpoint was lacking in the data, calculations were made based on the reported median, range, or interquartile range (IQR), if provided [31, 32].
The heterogeneity of the studies was assessed by means of the I^2^ statistic. The random-effects model was performed when I^2^ > 50% indicated significant heterogeneity. Otherwise, the heterogeneity was considered acceptable and the fixed-effects model was used. Statistical significance was set at P < 0.05. In addition, subgroup analyses were performed according to different study designs.
Results
Search results and study characteristics
From the final literature search, a total of 289 studies (176 in PubMed, 84 in Web of Science, and 29 in the Cochrane Library) were retrieved according to the search strategy. While the search covered 289 studies, 13 studies were included in our meta-analysis after eliminating duplicates and screening the titles, abstracts, and full text of the literature according to strict inclusion and exclusion criteria. The details of the screening are shown in Fig. 1. The total number of patients included in the thirteen studies was 4255 (2382 in the CO group and 1873 in the NCO group). The included studies were published between 2008 and 2023, with a study period ranging from 2000 to 2021, and came from four countries, China, Korea, Japan, and the US. The general information of the included studies, as well as the population characteristics, are summarized in Tables 1 and 2. According to the Cochrane Risk of Bias tool, one RCT study included had a mild risk of bias, as shown in Fig. 2. The remaining 12 studies were retrospective and, according to the Newcastle-Ottawa Scale, all achieved a score of more than 7, thus indicating that they can be regarded as high-quality studies.Fig. 1PRISMA flowchart of the literature search and selection procedureTable 1Study general informationAuthors/YearStudy designStudyPeriodCountryGroupSample sizeGender(Male/Fmale)Age (Years),Mean or MedianBMI(kg/m2),Mean or MedianQuality scoreSong M al. 2023Retrospective2019–2021ChinaCO5029/21NANA9NCO5829/29NANAJeong SA al. 2023Retrospective PSM2005–2017KoreaCO91198/112 NA58.92 ± 18.123.40 ± 3.019NCO9138/55 NA55.94 ± 15.1523.85 ± 3.15Lee H al. 2023Retrospective PSM2009–2016KoreaCO10770/3765.0(30.0–85.0)22.7 (16.4–32.0)9NCO10770/3762.0(30.0–92.0)23.5 (15.3–31.4)Lee S al. 2022Retrospective PSM2014–2018KoreaCO174122/5259.9 ± 12.723.1 ± 3.79NCO248177/7161.6 ± 13.323.8 ± 3.1Seo WJ al. 2021Retrospective PSM2003–2015KoreaCO225131/9459 (49–70)23.5 (21.1–25.6)9NCO225137/8856 (49–67)22.9 (21.0–24.9)Murakami H al. 2021Prospective RCT2011–2018JapanCO12289/3371 (30–90)22.4 (14.8–31.8)-NCO12589/3674 (45–89)22.2 (14.5–32.1)Sakimura Y al. 2020Retrospective PSM2008–2017JapanCO7046/2465.0 (37–90)22.2 (15.8–30.3)8NCO7048/2266.5 (42–94)22.4 (16.4–32.6)Ri M al. 2020Retrospective PSM2006–2012JapanCO263176/8766.7 ± 11.022.4 ± 3.69NCO263181/8265.7 ± 12.922.5 ± 3.4Young S al. 2020Retrospective2008–2016USACO9062/2869.5 (62–77)27.4 ± 6.18NCO381217/16468 (58–76)26.2 ± 5.3Kim DJ al. 2014Retrospective PSM2004–2011KoreaCO8056/2460.9 ± 11.2NA7NCO6650/1662.2 ± 11.0NAHasegawa S al. 2013Retrospective PSM2000–2009JapanCO9872/2669.0 (40–91)NA8NCO9872/2668.7 (45–91)NAKim MC al. 2011Retrospective2005–2009KoreaCO2017/358.2 ± 9.523.3 ± 2.38NCO1711/658.6 ± 10.123.6 ± 2.7Ha TK al. 2008Retrospective2004–2006KoreaCO992681/31157.0 ± 11.3NA7NCO12487/3756.3 ± 11.3NA*BMI *Body Mass Index, *CO *complete omentectomy, *NCO *non-complete omentectomy, *PSM *propensity score matching, *RCT *randomized controlled trial, *NA not available, Quality Score, According to Newcastle–Ottawa ScaleTable 2General population characteristicsAuthors/YearGroupSurgical approachSurgical procedurePathological T stagePathological N stageTNM stageLymphadenectomyOpenMISOthersTGT0T1T2T3T4N0N1N2N3IIIIIIIVD1D1+D2D2+Song M al. 2023CO05050000022281832NANANANA00500NCO05858000025232038NANANANA00580Jeong SA al. 2023CONANANANA000091NANANANANANANANANANANANANCONANANANA000091NANANANANANANANANANANANALee et al. 2023CO0107107000061465651NANANANA011060NCO0107107000061465651NANANANA014930Lee et al. 2022CO017410173002278744219397410431210NANANANANCO0248157910045119846535628621771500NANANANASeo et al. 2021CO69156167580001001257542426609513000252000NCO60165169560001111147347426309912600222030Murakami et al. 2021CO12207349020214239442925242648417191102NCO125081440312131425425172938404072131073Sakimura et al. 2020CO412945251512322022141420NANANANA961NCO25454426061627212914918NANANANA1456Ri et al. 2020CO2630156107047216148115281011295111461024NCO26301511120482151451182996131781461036Young et al. 2020CONANA3125NANANA414753NANANANANANANANANCONANA14099NANANA184176205NANANANANANANANAKim et al. 2014CO0806119002852040141313173924002780NCO06624120037290348168232617005610Hasegawa et al. 2013CO980524600303434392518161640420012842NCO8414613700343034412317172136410013832Kim et al. 2011CO2002000200001910NANANANA137NCO1701700161001520NANANANA152Ha et al. 2008CONANA91775early gastric cancerNANANANA97715NANANANANCONANA9925early gastric cancerNANANANA1240NANANANACO *complete omentectomy, *NCO *non-complete omentectomy, *MIS *minimally invasive surgery, *TG *Total gastrectomy, *NA *not availableFig. 2Risk of bias summary for the included RCT studies
Meta-analysis of outcomes
Surgery-related outcomes
Eleven studies [6–9, 11–15, 25, 27] reported the operative time in both groups, and the meta-analysis showed that the NCO group was associated with shorter operative time (MD = 18.20, 95% CI = 7.91–28.50, P = 0.0005) than the CO group. (Fig. 3A).Fig. 3. Forest plots showing the assessment of surgical-related outcomes: (A) operative time; (B) estimated blood loss; (C) the number of harvested lymph nodes; (D) postoperative complications. CO, complete omentectomy; NCO, non-complete omentectomy
Seven studies [6–8, 11, 13, 25, 27] reported the estimated blood loss in both groups, and the meta-analysis showed that the NCO group was associated with lower estimated blood loss (MD = 38.32, 95% CI = 9.77–66.88, P = 0.009) than the CO group. (Fig. 3B).
Ten studies [6–9, 11, 12, 14, 15, 25, 27] reported the number of harvested lymph nodes in both groups, and the meta-analysis showed a non-statistically significant difference between the CO and NCO groups (MD = −1.29, 95% CI = −3.27–0.69, P = 0.20). (Fig. 3C).
Twelve studies [6–11, 13–15, 25–27] reported postoperative complications in both groups, and the meta-analysis showed that the NCO group was associated with fewer postoperative complications (RR = 1.19, 95% CI = 1.03–1.38, P = 0.02) than the CO group. (Fig. 3D).
Survival outcomes
Nine studies [7, 9–14, 26, 27] reported the 3-year OS in both groups, and the meta-analysis showed that the NCO group was associated with a higher 3-year OS rate (RR = 0.95, 95% CI = 0.91–0.99, P = 0.02) than the CO group. (Fig. 4A).Fig. 4. Forest plots showing the assessment of survival outcomes: (A) 3-year overall survival rate; (B) 5-year overall survival rate; (C) 3-year relapse-free survival rate; (D) 5-year relapse-free survival. CO, complete omentectomy; NCO, non-complete omentectomy
Eight studies [7, 9–13, 25, 26] reported the 5-year OS in both groups, and the meta-analysis showed that the NCO group was associated with a higher 5-year OS rate (RR = 0.91, 95% CI = 0.87–0.96, P = 0.0006) than the CO group. (Fig. 4B).
Five studies [10, 11, 13, 14, 26] reported the 3-year RFS in both groups, and the meta-analysis showed that the difference between the two groups was not statistically significant. (RR = 0.95, 95% CI = 0.89–1.01, P = 0.12). (Fig. 4C).
Six studies [7, 10, 11, 13, 25, 26] reported the 5-year RFS in both groups, and the meta-analysis showed that the NCO group was associated with a higher 5-year RFS rate (RR = 0.93, 95% CI = 0.87–0.99, P = 0.02) than the CO group. (Fig. 4D).
Recurrence
Ten studies [6, 7, 10–14, 25–27] reported the overall recurrence rate in both groups, and the meta-analysis showed that the NCO group was associated with a lower overall recurrence rate (RR = 1.19, 95% CI = 1.03–1.38, P = 0.02) than the CO group. (Fig. 5A).Fig. 5. Forest plots showing the assessment of recurrence: (A) overall recurrence rate; (B) peritoneal recurrence rate. CO, complete omentectomy; NCO, non-complete omentectomy
Nine studies [6, 7, 10, 11, 13, 14, 25–27] reported the peritoneal recurrence rate in both groups, and the meta-analysis showed no statistically significant difference in peritoneal recurrence rate (RR = 1.24, 95% CI = 0.99–1.56, P = 0.06) for the two groups. (Fig. 5B).
Subgroup analyses
Subgroup analyses were performed according to study design, and meta-analysis of PSM and RCT studies [6–8, 10–13, 25, 26] confirmed that the NCO group was associated with shorter operative times, fewer postoperative complications, lower rates of overall recurrence, higher 3-year and 5-year OS rates, and higher 5-year RFS rate. (Additional materials, Figures S1–10). Additionally, a subgroup analysis was conducted based on the quality of the research. A meta-analysis of retrospective studies with NOS scores of 9 and RCT studies confirmed that the NCO group was associated with lower estimated blood loss, fewer postoperative complications, lower rates of peritoneal recurrence, higher 5-year OS rates, and higher 5-year RFS rate. (Additional materials, Figures S11–20).
Publication bias
Our meta-analysis used funnel plots to assess publication bias (Fig. 6). Despite the symmetrical appearance of the funnel plot, the risk of publication bias was considered to be moderate due to the small number of RCTs included in the paper.Fig. 6. Funnel plots of publication bias: (a) Overall recurrence rate; (b) peritoneal recurrence rate; (c) 3-year OS rate; (d) 5-year OS rate; (e) 3-year RFS rate; (f) 5-year RFS rate Additional file 1.pdf. Title of data: Additional materials. Subgroup analysis by study type, including Figures S1–8
Discussion
Surgery or endoscopic resection of GC is a necessary cornerstone of treatment [33]. However, after standard surgery, cancer still has a recurrence rate of 39–61% [34, 35]. The peritoneal recurrence rate accounts for 35% of the total recurrence rate [35]. Simultaneously, the peritoneum is one of the most common metastatic sites for GC, occurring in 15–30% of patients at diagnosis [36]. And it is estimated that this metastasis may occur in 55–60% of patients [37].
Among metastases to the peritoneum, metastasis to the greater omentum is a common site of GC metastasis, and this condition often signals a poor prognosis for the patient [38]. In anatomical terms, the greater omentum, adjacent to the stomach and colon, is a two-layered peritoneum that descends from the greater curvature of the stomach, covers the small intestine, and then folds up to fuse with the peritoneum on the anterior surface of the transverse colon, making the greater omentum susceptible to metastasis of cancerous cells implanted by gravity [39, 40]. Under microscopic observation, the greater omentum is composed of two different tissue types: a porous translucent membranous area and a vessel-rich area of adipose tissue, which stimulates the lymphatic tissue to accumulate around the blood vessels in an area known as the"milky spot “ [41]. The milky spot is composed of macrophages (70%), B cells (10%), T cells (10%), and mast cells [42]. Because it consists primarily of the above immune cells, it can function as a distinct secondary lymphoid tissue in peritoneal immunity [43]. With the exception of milk spots, the greater omentum is composed of mesothelial cells and vascular connective tissue. Mesothelial cells are sentinel cells that can sense and respond to signals within the microenvironment, and they play an important role in regulating inflammatory, immune, and tissue repair responses, and may even prevent the peritoneal spread of tumors [44]. The greater omentum has a certain anti-tumor effect due to the presence of milky spots and mesothelial cells. However, this structure is also susceptible to metastasis, and the milk spots and adipocytes can, under certain circumstances, be converted into a source of energy for tumor cells, as well as provide a suitable microenvironment for tumor cells [45]. Therefore, it is still controversial whether the omental tissue is completely resected in radical gastrectomy.
The meta-analysis in this paper was conducted to update the data related to the impact of NCO on patient outcomes compared to CO in radical gastrectomy. A total of thirteen studies including twelve retrospective studies and one RCT were included in this paper. Eight of the 12 retrospective studies progressed to PSM. Studies have shown that NCO is significantly associated with shorter operative time, less intraoperative bleeding, fewer postoperative complications, higher rates of 3-year and 5-year overall survival and 5-year recurrence-free survival, and a lower rate of postoperative recurrence. Subsequently, subgroup analysis was conducted based on the research design, and the results were identified as consistent with the previous findings. However, the results of the study indicated a notable statistical heterogeneity in relation to operative time, estimated blood loss, and the number of harvested lymph nodes. Three potential explanations for this heterogeneity can be postulated. Firstly, the duration of the study is 21 years, and the surgical approaches employed in each study may vary, resulting in discrepancies in the selection of anastomosis techniques and surgical equipment by the researchers. Secondly, the studies included GC patients with varying clinical and pathological stages. Thirdly, the inclusion of predominantly retrospective studies may result in heterogeneity due to measurement errors.
The result of this paper indicates that the NCO cohort demonstrated higher OS and 5-year RFS rates, which may potentially be attributed to the following factors: CO increases the difficulty of the operation due to the need to handle more omentum, particularly in laparoscopic surgery. The resection involves more blood vessels and tissue structures, which, under the same conditions, prolongs the surgical time and increases the possibility of intraoperative bleeding. Previous research indicates that increased intraoperative blood loss may negatively impact the prognosis of GC patients [46]. However, the absence of the omentum could reduce the body’s ability to limit infection and prevent disease [44], potentially leading to more complications and a poorer prognosis. In terms of recurrence rate, it is noteworthy that the NCO group is significantly correlated with a lower overall recurrence rate. However, no significant difference was observed in the results of peritoneal recurrence between the two groups. Firstly, the surgical procedure in the CO group is associated with greater blood loss and a longer surgical duration, which might increase the risk of damaging the integrity of lymphatic and blood vessels in the surgical area. Furthermore, it is important to consider the role of the omentum in regulating inflammatory, immune, and tissue repair responses when removing it during gastric cancer surgery. The combined effect of two distinct types of injury factors may potentially exacerbate the possibility of recurrence in GC patients during the recovery period.
For patients with advanced gastric cancer, the optimal treatment plan should include not only surgical intervention but also a multimodal treatment to improve prognosis [47]. Although the treatment guidelines for adjuvant chemotherapy and neoadjuvant chemotherapy vary in different countries, adjuvant chemotherapy is recommended in Asian countries, while neoadjuvant chemotherapy and adjuvant chemotherapy are recommended in Europe and America [48, 49]. With the confirmation of the safety and efficacy of neoadjuvant chemotherapy, the application of adjuvant therapy may be of greater importance than the selection of omentectomy. Among the studies included in the paper, seven studies [6, 7, 10, 11, 13, 26, 27] mentioned the use of chemotherapy, but did not provide specific prognostic data. Consequently, it is imperative to obtain more comprehensive data regarding the entirety of the cancer treatment process in order to reliably reach conclusions.
Although thirteen relevant studies were included in our paper, the impact of preoperative pathologic staging and tumor location of GC on surgical, survival, and recurrence outcomes was not considered. Perioperative chemotherapy has been the standard of care for resectable localized GC, while adjuvant chemotherapy is recommended for patients with stage II or III disease who have improved survival [3]. The impact of these treatments on patients was not explored by us. Furthermore, the majority of studies originate from Asian countries, which introduces certain limitations. Therefore, we cannot completely exclude whether the above factors might have influenced the differences between the CO and NCO groups.
Conclusions
In conclusion, our meta-analysis indicates that compared to NCO, CO has no benefit on surgery-related, survival, or recurrence outcomes. Although there are limitations to the studies discussed in this paper, based on the available evidence, NCO may be a more feasible procedure in radical gastrectomy. As most of the studies included in our meta-analysis were retrospective, more high-quality and well-designed RCTs are needed to further substantiate our results.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1(2021) Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer 24(1):1–2110.1007/s 10120-020-01042-y PMC 779080432060757 · doi ↗ · pubmed ↗
- 2Sakimura Y, Inaki N, Tsuji T, Kadoya S, Bando H (2020) Long-term outcomes of omentum-preserving versus resecting gastrectomy for locally advanced gastric cancer with propensity score analysis. Sci Rep 10(1):1630510.1038/s 41598-020-73367-8PMC 752979833004919 · doi ↗ · pubmed ↗
- 3Kim DJ, Lee JH, Kim W (2014) A comparison of total versus partial omentectomy for advanced gastric cancer in laparoscopic gastrectomy. World J Surg Oncol 12:6410.1186/1477-7819-12-64PMC 398688224669875 · doi ↗ · pubmed ↗
- 4Zizzo M, Zanelli M, Sanguedolce F, Palicelli A, Ascani S, Morini A et al (2022) Gastrectomy with or without complete omentectomy for advanced gastric cancer: a meta-analysis. Med (Kaunas) 58(9):124110.3390/medicina 58091241 PMC 950372436143918 · doi ↗ · pubmed ↗
- 5Deeks JJ, Bossuyt PM, Leeflang MM, YT (2023) Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy. Version 2.0 (updated July 2023). Cochrane 10.1002/14651858.ED 000163 PMC 1040828437470764 · doi ↗ · pubmed ↗
- 6Manzanedo I, Pereira F, Pérez-Viejo E, Serrano Á (2023) Gastric Cancer with peritoneal metastases: current status and prospects for treatment. Cancers (Basel) 15(6):177710.3390/cancers 15061777 PMC 1004617336980663 · doi ↗ · pubmed ↗
- 7Ruiz Hispán E, Pedregal M, Cristobal I, García-Foncillas J, Caramés C (2021) Immunotherapy for peritoneal metastases from gastric cancer: rationale, current practice and ongoing trials. J Clin Med 10(20):464910.3390/jcm 10204649 PMC 853917734682772 · doi ↗ · pubmed ↗
- 8Yeh JH, Yeh YS, Tsai HL, Huang CW, Chang TK, Su WC et al (2022) Neoadjuvant chemoradiotherapy for locally advanced gastric cancer: where are we at? Cancers (Basel) 14(12):302610.3390/cancers 14123026 PMC 922103735740693 · doi ↗ · pubmed ↗