The impact of immune checkpoint inhibitors on prognosis in unresectable hepatocellular carcinoma treated with TACE and lenvatinib: a meta-analysis
Wei Zhang, Zirong Liu, Hongjin Liu, Zhangkan Huang, Xiaozhun Huang, Lin Xu, Xu Che, Zhengyin Zhan

TL;DR
Adding immune checkpoint inhibitors to TACE and lenvatinib improves survival and response rates in unresectable liver cancer, but increases hypothyroidism risk.
Contribution
This meta-analysis evaluates the combined effect of TACE, lenvatinib, and ICIs in unresectable hepatocellular carcinoma.
Findings
TACE+L+I significantly improved complete and partial response rates compared to TACE+L.
TACE+L+I showed better overall and progression-free survival than TACE+L.
Hypothyroidism was more common with TACE+L+I, but other adverse events were similar.
Abstract
Combination of multiple therapies is a common approach to treating patients with unresectable hepatocellular carcinoma (uHCC). The impact of immune checkpoint inhibitors (ICIs) on prognosis in uHCC patients treated with transarterial chemoembolization (TACE) and lenvatinib remains unclear. The purpose of this study was to compare the efficacy and safety of TACE plus lenvatinib plus ICIs (TACE+L+I) with TACE plus lenvatinib (TACE+L) in the treatment of patients with uHCC. Publicly available studies comparing the efficacy and safety of TACE+L+I and TACE+L in the treatment of uHCC were collected from the databases PubMed, Embase and Cochrane Library, with a cut-off date of November 1, 2024. Stata SE 15 software was used for analysis. Fifteen studies with a total of 1365 patients were included, 688 in the TACE+L+I group and 677 in the TACE+L group. Meta-analysis showed that the TACE+L+I…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
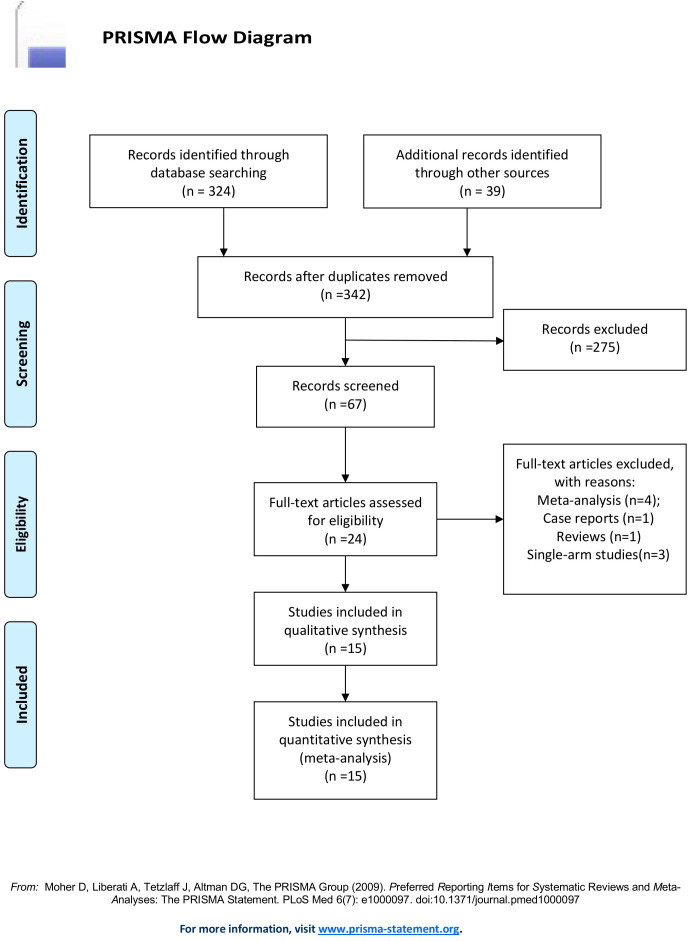 Figure 1
Figure 1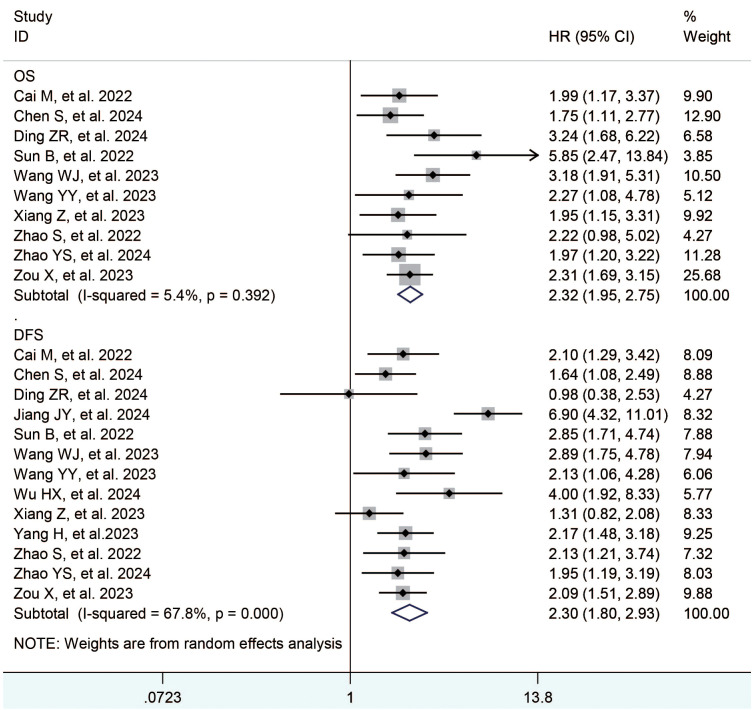 Figure 2
Figure 2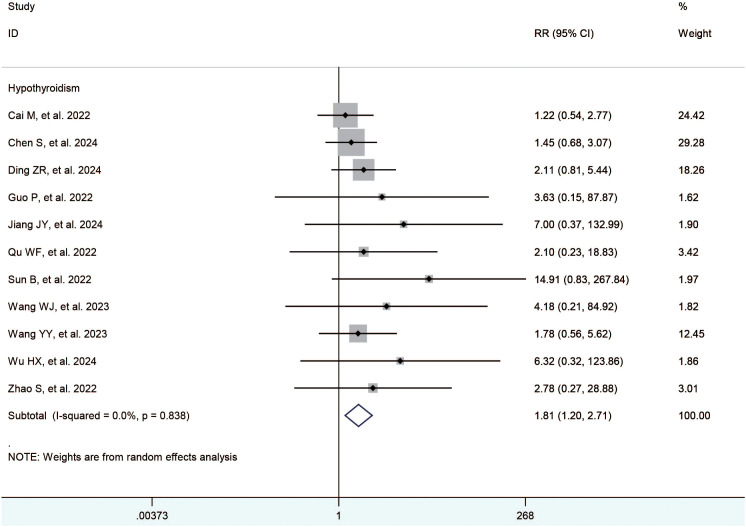 Figure 3
Figure 3| Study | Country | Study period | Study type | Case | Gender(F/M) | Age | Quality* | ||
|---|---|---|---|---|---|---|---|---|---|
| TACE+L+I vs. TACE+L | TACE+L+I | TACE+L | TACE+L+I | TACE+L | |||||
| Cai M, et al., 2022 ( | China | 2019-2020 | R | 41 vs. 40 | 4/37 | 7/33 | 51.9 ± 10.3 | 54.6 ± 11.0 | 7 |
| Chen S, et al., 2024 ( | China | 2016-2020 | R | 70 vs. 72 | 37/33 | 38/34 | NA | NA | 7 |
| Ding ZR, et al., 2023 ( | China | 2019-2022 | R | 19 vs. 16 | 1/18 | 3/13 | 57.0 [47.0, 64.5] | 61.5 [53.0, 65.0] | 7 |
| Guo P, et al., 2022 ( | China | 2018-2022 | R | 48 vs. 48 | 1/47 | 2/46 | NA | NA | 6 |
| Jiang J, et al., 2023 ( | China | 2018-2022 | R | 42 vs. 45 | 9/33 | 4/41 | 61.71 ± 9.48 | 61.24 ± 12.10 | 7 |
| Qu WF, et al., 2022 ( | China | 2018-2021 | R | 30 vs. 21 | 4/26 | 1/20 | 55.5 (47.8, 64.3) | 50.0 (45.0, 61.0) | 6 |
| Sun B, et al., 2022 ( | China | 2018-2021 | R | 31 vs. 52 | 6/25 | 6/46 | 54.84 ± 9.249 | 51.77 ± 9.791 | 7 |
| Wang WJ, et al., 2023 ( | China | 2019-2020 | R | 51 vs. 45 | 5/49 | 2/43 | 57.0 ± 9.9 | 60.8 ± 9.4 | 7 |
| Wang YY, et al., 2023 ( | China | 2017-2022 | R | 45 vs. 20 | 3/42 | 5/15 | 54 (18-79) | 62 (26-75) | 7 |
| Wu XH, et al., 2024 ( | China | 2019-2020 | R | 18 vs. 23 | 3/15 | 5/18 | 56.9 ± 8.1 | 58.1 ± 9.4 | 7 |
| Xiang Z, et al., 2023 ( | China | 2018-2021 | R | 33 vs. 49 | 5/28 | 4/45 | 51.0 ± 12.2 | 51.7 ± 11.2 | 7 |
| Yang H, et al.2023 ( | China | 2019-2022 | R | 64 vs. 58 | 13/64 | 11/58 | 61.4 ± 9.3 | 63.2 ± 8.5 | 7 |
| Zhao S, et al., 2022 ( | China | 2018-2020 | R | 23 vs. 32 | 0/23 | 1/31 | 52.83 ± 7.14 | 57.38 ± 9.44 | 7 |
| Zhao YS, et al., 2024 ( | China | 2021-2023 | R | 103 vs. 66 | 24/78 | 7/59 | NA | NA | 7 |
| Zou X, et al., 2023 ( | China | 2018-2022 | R | 70 vs. 90 | 11/59 | 13/77 | 53.6 ± 15.1 | 52.3 ± 14.8 | 7 |
| Measured Outcomes | No. Studies | Heterogeneity Test | Model | RR/HR | 95%CI |
| |
|---|---|---|---|---|---|---|---|
|
|
| ||||||
| Complete response | 15 | 0 | 0.94 | Random | 2.34 | 1.53,3.59 |
|
| Partial response | 15 | 0 | 0.73 | Random | 1.45 | 1.28,1.64 |
|
| Stable disease | 15 | 30 | 0.13 | Random | 0.85 | 0.69,1.03 | 0.10 |
| Progressive disease | 15 | 8 | 0.36 | Random | 0.39 | 0.30,0.51 |
|
| Objective response rate | 15 | 0 | 0.51 | Random | 1.55 | 1.39,1.73 |
|
| Disease control rate | 15 | 83 | <0.00001 | Random | 1.22 | 1.10,1.36 |
|
| Overall survival | 10 | 5.4 | 0.392 | Random | 2.32 | 1.95, 2.75 |
|
| Progression free survival | 13 | 67.8 | 0 | Random | 2.30 | 1.80, 2.93 |
|
| Adverse events | Grade | No. Studies | Heterogeneity Test | Model | RR | 95%CI |
| |
|---|---|---|---|---|---|---|---|---|
|
|
| |||||||
| Hypertension | Any Grade | 15 | 0 | 0.97 | Random | 1.19 | 1.00,1.41 | 0.05 |
| Diarrhea | Any Grade | 12 | 0 | 1 | Random | 1.18 | 0.95,1.46 | 0.14 |
| Hand-foot syndrome | Any Grade | 13 | 0 | 0.97 | Random | 1.04 | 0.87,1.24 | 0.7 |
| Fatigue | Any Grade | 12 | 0 | 0.97 | Random | 1.1 | 0.93,1.30 | 0.28 |
| Elevated AST | Any Grade | 6 | 0 | 0.55 | Random | 1.02 | 0.92,1.13 | 0.72 |
| Elevated ALT | Any Grade | 7 | 0 | 0.87 | Random | 1.08 | 0.93,1.26 | 0.31 |
| Decreased appetite | Any Grade | 9 | 0 | 0.98 | Random | 0.98 | 0.71,1.37 | 0.92 |
| Hypothyroidism | Any Grade | 11 | 0 | 0.84 | Random | 1.81 | 1.20,2.71 |
|
| Abdominal pain | Any Grade | 12 | 9 | 0.36 | Random | 1.04 | 0.91,1.18 | 0.55 |
| Thrombocytopenia | Any Grade | 6 | 0 | 0.98 | Random | 1.16 | 0.81,1.66 | 0.43 |
| Rash | Any Grade | 9 | 0 | 0.85 | Random | 1.13 | 0.92,1.39 | 0.24 |
| Nausea | Any Grade | 13 | 0 | 0.90 | Random | 1.00 | 0.85,1.17 | 1 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatocellular Carcinoma Treatment and Prognosis · Liver Disease Diagnosis and Treatment · Ferroptosis and cancer prognosis
Introduction
1
Hepatocellular carcinoma (HCC), one of the most common fatal malignancies, accounts for 75-85% of primary liver malignant tumors (1). Although surgical resection, ablation, and liver transplantation are effective on early-stage HCC, most patients with HCC are diagnosed with advanced disease and have a poor prognosis, with an expected median survival of 6–8 months (2–4). Transarterial chemoembolization (TACE) is recommended by various guidelines for the treatment of unresectable HCC (uHCC) (2–4). The use of TACE can effectively slow down the local progression of intrahepatic tumors, but may not be as effective in treating extrahepatic metastases, making it a less satisfactory treatment option (5). Hypoxia occurs in liver after TACE, which induce tumor angiogenesis and potentially lead to tumor recurrence and progression. The combination of anti-angiogenic drugs with TACE can effectively counteract the angiogenesis caused by hypoxia after TACE, resulting in better inhibition of HCC (6, 7). Lenvatinib is a new tyrosine kinase inhibitor approved in 2018 as a first-line treatment for uHCC (8). Some studies have shown that the combination of TACE and lenvatinib can induce a satisfactory effect in the treatment of uHCC (9–13), and the combination of TACE and antiangiogenic drugs has become a promising choice for the treatment of advanced-stage HCC.
Immune checkpoint inhibitors (ICIs), including programmed death 1 (PD-1) and programmed death ligand 1 (PD-L1) inhibitors, have recently shown clinical benefit in patients with a variety of solid tumors (14). Some encouraging results suggest that the combination of TACE, lenvatinib, and ICIs has promising therapeutic potential for patients with HCC (15, 16). In theory, hypoxia following TACE promotes angiogenesis and disrupts antitumor immunity. However, lenvatinib not only inhibits angiogenesis but also normalizes vasculature and reduces the immunosuppressive environment of tumors, creating a favorable setting for T cell trafficking into tumors, thereby enabling the efficacy of ICIs (17–19); thus the combination of TACE, lenvatinib, and ICIs may induce a synergistic antitumor effect on HCC, improving clinical outcomes and inducing manageable side effects. Some studies comparing the efficacy and safety of TACE+L+I versus TACE combined with lenvatinib (TACE+L) in the treatment of patients with uHCC are available, but with inconsistent conclusions. Therefore, the purpose of this meta-analysis was to evaluate the efficacy and safety of ICIs in patients with uHCC treated with TACE+L, to be used as a clinical reference.
Materials and methods
2
A systematic evaluation and meta-analysis of preferred reporting items was performed according to the PRISMA guidelines (20). This study did not require formal institutional review board approval or patient informed consent because it was a secondary study using publicly available data.
Search strategy
2.1
A literature search on the EMBASE, PubMed, and Cochrane Library databases was performed to identify relevant available articles up to November 1, 2024. The search strategy for each database is shown in the Supplementary File S1. The authors were contacted to obtain extra information if necessary. If multiple studies were performed by the same authors or medical centers with duplicates in patients, the highest quality study was selected.
Inclusion criteria
2.2
(1) Study population: confirmed diagnosis of uHCC; (2) Publicly available literature reporting comparative efficacy of TACE+L+I and TACE+L; (3) No restriction on the study sample size; (4) No restriction on the duration of the follow-up; (5) No restriction on the type of language used to write the articles; (6) Human studies only; and (7) Study results were evaluated by the Response to Criteria for Evaluation of the Efficacy of Solid Tumors (RECIST), Common Terminology Criteria for Adverse Events v5.0.
Extraction criteria
2.3
(1) Studies with incomplete information, no access to valid data, no response from the authors after contacting them, duplicates and unpublished studies; (2) single-arm studies of TACE+L+I or TACE+L; (3) other treatments such as radiofrequency ablation; and (4) reviews, case reports, and animal experiments.
Quality assessment
2.4
In all the included studies, RCTs conducted a risk assessment of the risk according to the “risk assessment tool” recommended by the Cochrane Collaboration Network. The Cohort Studies are based on the Newcastle-Ottawa Scale. The results are shown in the Supplementary File S2.
Statistical analysis
2.5
Statistical analysis in this meta-analysis was performed using Stata SE 15 software. Relative risk (RR) was calculated in comparison of dichotomous variables by Mantel-Haenszel method, and hazard ratio (HR) was calculated in the comparison of survival variables by Inverse Variance method. The level of heterogeneity among studies was evaluated using I ^2^ statistics. A randomized model was used in this study. Sensitivity analysis was performed by removing 1 study at a time to assess whether the results were markedly affected by a single study. Funnel plots were used to qualitatively assess publication bias, and the results are shown in the Supplementary File S3. Begg’s test and Egger’s test were quantitatively used to assess publication bias in the included studies, and their significance level was limited to 0.05, as shown in the Supplementary File S4.
Results
3
Search results and study selection
3.1
A total of 363 articles were collected. The duplicates were excluded; then 342 articles remained. Then, reviews, case reports, and other types of articles were excluded. Finally, 15 articles remained (21–35). The detailed steps of our literature search are shown in Figure 1. Fifteen studies with a total of 1365 patients were included in the final analysis. A total of 688 patients (50.40%) received TACE+L+I, and 677 (49.60%) patients received TACE+L. The characteristics of these studies are listed in Table 1.
PRISMA flow diagram.
Meta-analysis results
3.2
The treatment effects of TACE+L+I and TACE+L were compared by assessing tumor response, long-term survival outcome, and adverse events. The results are listed in Tables 2, 3.
Tumor response
3.2.1
Fifteen studies (21–35) reported complete response, partial response, stable disease, progression of disease, objective response rate, and disease control rate. The meta-analysis showed that the TACE+L+I group was significantly better than the TACE+L group in complete response (RR = 2.34, 95%CI:1.53, 3.59, p < 0.0001), partial response (RR = 1.45, 95%CI:1.28, 1.64, p < 0.0001), progression of disease (RR = 0.39, 95%CI:0.30, 0.51, p < 0.00001), objective response rate (RR = 1.55, 95%CI:1.39, 1.73, p < 0.00001), disease control rate (RR = 1.22, 95%CI:1.10, 1.36, p = 0.0003), whereas the TACE+L+I group was not significantly different from the TACE+L group in stable disease (RR = 0.85, 95%CI:0.69, 1.03, p = 0.10). As shown in Table 2.
Long-term survival outcome
3.2.2
Thirteen studies (23, 25, 27–35) reported the overall survival and progression free survival. The meta-analysis showed that the TACE+L+I group was significantly better than the TACE+L group in terms of overall survival (HR = 2.32, 95%CI:1.95, 3.15, p < 0.05) and progression free survival (HR = 2.30, 95%CI:1.80, 2.93, p < 0.05), as shown in Table 2 and Figure 2.
Forest plots survival (OS) and disease-free survival.
Adverse events
3.2.2.1
The included studies (21–35) reported the hypertension, diarrhea, hand-foot syndrome, fatigue, elevated ast, elevated alt, decreased appetite, hypothyroidism, abdominal pain, thrombocytopenia, rash, and nausea. The meta-analysis showed no significant difference between the TACE+L+I and TACE+L group regarding hypertension (RR = 1.19, 95%CI:1.00, 1.41, P = 0.05), diarrhea (RR = 1.18, 95%CI:0.95,1.46, P = 0.14), hand-foot syndrome (RR = 1.04, 95%CI:0.87,1.24, P = 0.70), fatigue (RR = 1.10, 95%CI:0.93, 1.30, P = 0.28), elevated AST (RR = 1.02, 95%CI:0.92,1.13, P = 0.72), elevated ALT (RR = 1.08, 95%CI:0.93,1.26, P = 0.31), decreased appetite (RR = 0.98, 95%CI:0.71,1.37, P = 0.92), abdominal pain (RR = 1.04, 95%CI:0.91, 1.18, P = 0.55), thrombocytopenia (RR = 1.16, 95% CI:0.81,1.66, P = 0.43), rash (RR = 1.13, 95%CI. 0.92, 1.39, P = 0.24), and nausea (RR = 1.00, 95%CI:0.85,1.17, P = 1.00). However, hypothyroidism was significantly higher in the TACE+L+I group (RR = 1.81, 95%CI: 1.20, 2.71, P = 0.004) than in the TACE+L group, as shown in Table 3 and Figure 3.
Forest plots of the incidence of hypothyroidism.
Sensitivity analysis and publication bias
3.3
The results of each meta-analysis were stable when the sensitivity analysis was performed. Begg’s funnel plot with pseudo 95% confidence limits is shown in Supplementary File S3. Publication bias was not found using Begg’s test and Egger’s test, as shown in Supplementary File S4.
Discussion
4
HCC is the fifth most common cancer worldwide and the second most common cause of cancer-related deaths (1). First-line treatment options for HCC include surgical resection, ablation, liver transplantation, TACE, and drugs, but despite that, the prognosis of uHCC remains poor (36). The TACE is the standard treatment recommended by the European Association for the Study of the Liver guidelines and the Barcelona Clinic Liver Cancer (BCLC) treatment strategy for intermediate and advanced HCC (37, 38), and it may result in tumor response in up to 50% of HCC, resulting in a survival benefit. However, TACE alone has limited therapeutic efficacy as a local-regional therapy, which may promote anti-tumor immunity by releasing tumor antigens and inducing damage-associated molecules that induce “immunogenic cell death” (39, 40). Furthermore, the hypoxic microenvironment after TACE may result in the expression of VEGF and PD-L1 (39–42). Antiangiogenic drugs combined with ICIs represent a promising addition to TACE (43–48). So far, the conclusions of various studies regarding the survival benefit from TACE+L+I of patients with uHCC are inconsistent.
The results of our meta-analysis found that complete response, partial response, objective response rate, and disease control rate were significantly higher in the TACE+L+I group, while progression of disease was significantly lower in the TACE+L+I group than in the TACE+L group, suggesting that the addition of ICIs has a significantly enhanced the tumor response rate. Different therapeutic approaches at different clinical stages are needed to combat HCC, and combination therapy may be used (49, 50). Although tumor response rates suggest that the TACE+L+I is superior to the TACE+L, the effectiveness of antitumor treatments should be based on more direct evidence of clinical benefit, such as prolonged survival, improved quality of life, or reduction of associated symptoms. These clinical benefits are sometimes not predicted by tumor response rates. Therefore, the survival data were analyzed, revealing that the overall survival and progression-free survival were longer in the TACE+L+I group than in the TACE+L group.
Currently, the combination of TACE and lenvatinib is considered clinically safe. Our meta-analysis found that the TACE+L+I group had a significantly higher incidence of hypothyroidism compared to the TACE+L group, while the TACE+L+I group was not significantly different from the TACE+L group in other adverse events, such as hypertension, diarrhea, hand-foot syndrome, fatigue, elevated ast, elevated alt, decreased appetite, hypothyroidism, abdominal pain, thrombocytopenia, and rash, nausea. Common adverse events with lenvatinib included hand and foot skin reactions, diarrhea, and hypertension, while common adverse events with TACE included pain and transient transaminase elevations. Fortunately, treatment-related adverse events were predominantly grade 1 or 2 and were resolved or eliminated after appropriate and prompt management. Therefore, the adverse events associated with TACE+L+I were acceptable.
Several meta-analyses are available on similar topics, but all of them have limitations. Gao Y, et al. (51) performed a meta-analysis and concluded that TACE or hepatic arterial infusion chemotherapy (HAIC) combined with lenvatinib plus PD-1 inhibitor could effectively delays the progression of HCC, prolong the survival, and improve the quality of life of HCC patients with portal vein thrombosis. The intervention in that study included HAIC in addition to TACE. In another meta-analysis by Liu J, et al. (52), the authors compared the efficacy of TACE plus tyrosine kinase inhibitors and ICIs (T+T+I) with that of TACE plus tyrosine kinase inhibitors (T+T) for the treatment of uHCC, concluding that T+T+I for advanced HCC had better objective response rate, as well as longer progression-free survival and overall survival than TACE+T, with no significant increase in adverse events. They did not distinguish between lenvatinib and other tyrosine kinase inhibitors in the study, making the conclusions too broadly applicable. The first systematic review on T+L+I for uHCC was conducted by Sun L, et al. (53), but no further meta-analysis was performed. The first meta-analysis on the same topic was conducted by Liu J, et al. (54) in 2023. Eight cohort studies on TACE plus lenvatinib with or without ICIs for uHCC were included. The T+L+I group had significantly longer overall and progression-free survival in that meta-analysis, as well as higher objective response and disease control rates, which was consistent with our findings; however, there was a higher incidence of hypertension, vomiting or nausea, and hypothyroidism in the T+L+I group, which was inconsistent with our study. Our meta-analysis only found that the T+L+I group was significantly higher than the T+L group in hypothyroidism. The conclusions of our meta-analysis may be more in line with the first-line clinic, as the latest studies we included allowed for a larger number of patients to reduce the potential bias in previous meta-analyses.
This is the most comprehensive meta-analysis available assessing TACE+L+I for uHCC, and although most of the included studies were retrospective, which would be inherently subjected to selection and publication bias, retrospective studies can be reflective of the real world. Our findings assessed the real-world clinical efficacy of TACE+L+I for the treatment of uHCC, and provided a guidance for subsequent clinical studies, although this combination therapy needs further exploration in future randomized controlled trials.
Conclusions
5
TACE+L+I for advanced HCC resulted in significantly better tumor response rates, overall survival, and disease-free survival than TACE+L, while the incidence of hypothyroidism was higher in the TACE+L+I group than in the TACE+L group. The adverse events of ICIs were acceptable compared to the survival benefit of ICIs. These conclusions still need to be further confirmed in the future with high-quality randomized controlled trials.
Limitations
6
Our study has several limitations. First, this was a retrospective study, which may lead to selection bias. Second, there was significant heterogeneity across the included studies in terms of disease control rate. By exploring the source of the heterogeneity, we found that it was not originated from a particular study or studies, which may be related to the data distribution characteristics, because disease control rate corresponds to progressive disease, and inter-study heterogeneity is low in progressive disease. Therefore, subsequent scholars should be cautious in applying the outcome. Finally, most of the included studies were from a single institution with a limited number of cases and most came from China, leading to conclusions with little explanatory power.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H Ferlay J Siegel RL Laversanne M Soerjomataram I Jemal A . Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660 33538338 · doi ↗ · pubmed ↗
- 2Zhou J Sun H Wang Z Cong W Wang J Zeng M . Guidelines for the diagnosis and treatment of hepatocellular carcinoma (2019 edition). Liver Cancer. (2020) 9:682–720. doi: 10.1159/000509424 33442540 PMC 7768108 · doi ↗ · pubmed ↗
- 3Benson AB D’Angelica MI Abbott DE Anaya DA Anders R Are C . Hepatobiliary cancers, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. (2021) 19:541–65. doi: 10.6004/jnccn.2021.0022 34030131 · doi ↗ · pubmed ↗
- 4European Association For The Study Of The Liver . Corrigendum to ‘EASL recommendations on treatment of hepatitis C: Final update of the series’ [J Hepatol 73 (2020) 1170-1218. J Hepatol. (2023) 78:452. doi: 10.1016/j.jhep.2022.10.006 36464532 · doi ↗ · pubmed ↗
- 5Fu Z Li X Zhong J Chen X Cao K Ding N . Lenvatinib in combination with transarterial chemoembolization for treatment of unresectable hepatocellular carcinoma (u HCC): a retrospective controlled study. Hepatol Int. (2021) 15:663–75. doi: 10.1007/s 12072-021-10184-9 PMC 828694733877527 · doi ↗ · pubmed ↗
- 6Chang Y Jeong SW Young Jang J Jae Kim Y . Recent updates of transarterial chemoembolilzation in hepatocellular carcinoma. Int J Mol Sci. (2020) 21:8165. doi: 10.3390/ijms 21218165 33142892 PMC 7662786 · doi ↗ · pubmed ↗
- 7Kishore SA Bajwa R Madoff DC . Embolotherapeutic strategies for hepatocellular carcinoma: 2020 update. Cancers (Basel). (2020) 12(4):791. doi: 10.3390/cancers 12040791 32224882 PMC 7226474 · doi ↗ · pubmed ↗
- 8Kudo M Finn RS Qin S Han KH Ikeda K Piscaglia F . Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. (2018) 391:1163–73. doi: 10.1016/S 0140-6736(18)30207-1 29433850 · doi ↗ · pubmed ↗