“Defect-in-the-defect sign” after non-exposed endoscopic full-thickness resection
Chung-Ying Lee, Kuang-I Fu, Ding-Ek Toh, Ming-Yao Chen, Yen-Ying Chen

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
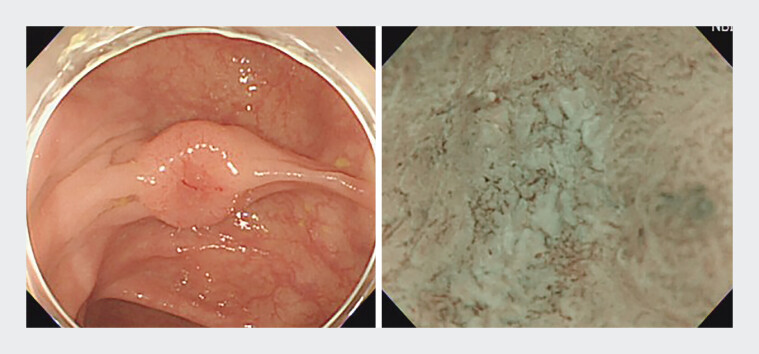 Fig. 1
Fig. 1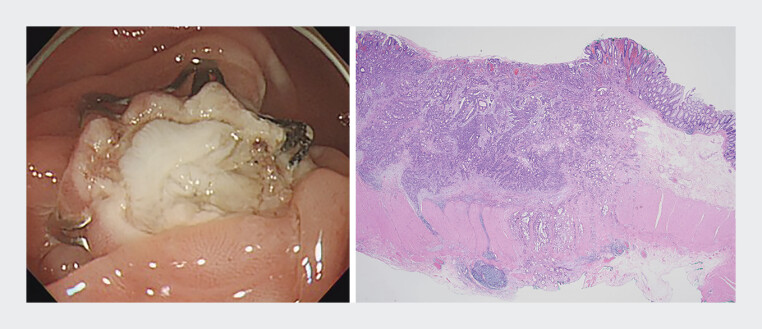 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Gastric Cancer Management and Outcomes · Pancreatic and Hepatic Oncology Research
Non-exposed endoscopic full-thickness resection (EFTR) has become a valuable technique for managing colorectal cancers (CRCs) with suspected deep invasion, particularly when conventional endoscopic resection is insufficient for safely obtaining adequate tissue beyond the submucosal layer. It enables en bloc resection while preserving GI wall integrity, with studies reporting high R0 resection rates and diagnostic accuracy, aiding treatment decisions for T1 CRCs, especially for those 20 mm or smaller 1 2 3 4 . Still, CRCs harboring far deeper invasion beyond endoscopic expectations could exist. Here, we present a unique case that revealed unexpectedly deep invasion (T4a) after non-exposed EFTR using a Padlock Clip.
During surveillance colonoscopy, a 75-year-old man was incidentally found to have a 12-mm depressed transverse colon lesion (IIa+IIc) ( Fig. 1 ). Image-enhanced endoscopy with magnification showed JNET classification type 3 within the depressed area, suggesting deep submucosal invasion (T1b). Abdominal CT revealed no lymph node involvement or distant metastasis. After shared decision-making, EFTR using a Padlock Clip (Aponos Medical) was performed ( Video 1 ).
A 12 mm lesion (IIa+IIc, JNET classification type 3) with multiple-fold convergences was identified in the transverse colon.
“Defect-in-the-defect sign” after non-exposed EFTR for a colon lesion with deep invasion.Video 1
After resection, a deeper defect, “defect-in-the-defect sign”, was observed in the resected wound of exposed muscularis propria. Pathologically, the deeper defect corresponded to the site of unexpectedly advanced cancer extending beyond the serosal layer with lympho-vascular invasion ( Fig. 2 , left & right). The patient subsequently underwent laparoscopic left hemicolectomy 3 weeks after the endoscopic resection, and a 0.4 cm residual cancer was found in the pericolic tissue without lymph node metastasis, and thus it was finally determined to be stage II (T4aN0M0).
Endoscopic and histopathologic correlation of non-exposed EFTR. (Left) The post-resection defect demonstrates the “defect-in-the-defect sign.” (Right) Histopathologic analysis confirmed adenocarcinoma with visceral peritoneum invasion (pT4a), correlating with the unexpected deep invasion detected post-EFTR. Abbreviation: EFTR, endoscopic full-thickness resection.
As non-exposed EFTR gains broader clinical use, endoscopists should remain vigilant for cases where invasion depth exceeds expectations. This “defect-in-the-defect sign” could serve as a key endoscopic finding, indicating deeper cancer invasion beyond resection that warrants further detailed histological assessment to avoid underestimation or residual leading to fatal recurrence subsequently.
Endoscopy_UCTN_Code_TTT_1AQ_2AD_3AF
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zwager LW Bastiaansen BA Jvan der Spek BW Endoscopic full-thickness resection of T 1 colorectal cancers: a retrospective analysis from a multicenter Dutch e FTR registry Endoscopy 20225447548534488228 10.1055/a-1637-9051 · doi ↗ · pubmed ↗
- 2Backes Y Kappelle WFW Berk L Colorectal endoscopic full-thickness resection using a novel, flat-base over-the-scope clip: a prospective study Endoscopy 2017491092109710.1055/s-0043-11473028753696 · doi ↗ · pubmed ↗
- 3Dolan RD Bazarbashi AN Mc Carty TR Endoscopic full-thickness resection of colorectal lesions: a systematic review and meta-analysis Gastrointest Endosc 2022952162.24E 2034627794 10.1016/j.gie.2021.09.039 · doi ↗ · pubmed ↗
- 4Mc Kechnie T Govind S Lee J Endoscopic Full-Thickness Resection for Colorectal Lesions: A Systematic Review and Meta-Analysis J Surg Res 202228044044910.1016/j.jss.2022.07.01936054955 · doi ↗ · pubmed ↗