Device-based measurement of physical activity and sedentary behaviour after critical illness: A scoping review
Darren Murphy, Annette Henderson, Judy M. Bradley, Bronwen Connolly, Jason J. Wilson, Brenda O’Neill, Hidetaka Hamasaki, Hidetaka Hamasaki, Hidetaka Hamasaki

TL;DR
This review examines how devices are used to measure physical activity and sedentary behavior in patients recovering from critical illness.
Contribution
The study identifies the need for standardized protocols for device-based data analysis in post-critical illness recovery.
Findings
Twenty-two studies used 11 different devices to measure activity and sedentary behavior after critical illness.
Physical activity levels remained low even after hospital discharge.
There is a lack of standardized data processing methods across studies.
Abstract
Measuring and promoting physical activity could support rehabilitation and recovery after critical illness. In recent years, there has been an emergence of the use of devices to measure both physical activity and sedentary behaviour in this population. Understanding device selection and processes for data analysis could be helpful for future research and practice when used with this population. The aim of this review was to explore the current use of device-based physical activity instruments to measure physical activity and sedentary behaviour during and following critical illness. A scoping review was conducted which followed the Arksey and O’Malley (2005) framework. A comprehensive search of four electronic databases (Medline, ProQuest, Scopus and CINAHL) was conducted using pre-agreed search terms. Screening and data extraction was conducted by two independent reviewers. Data were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
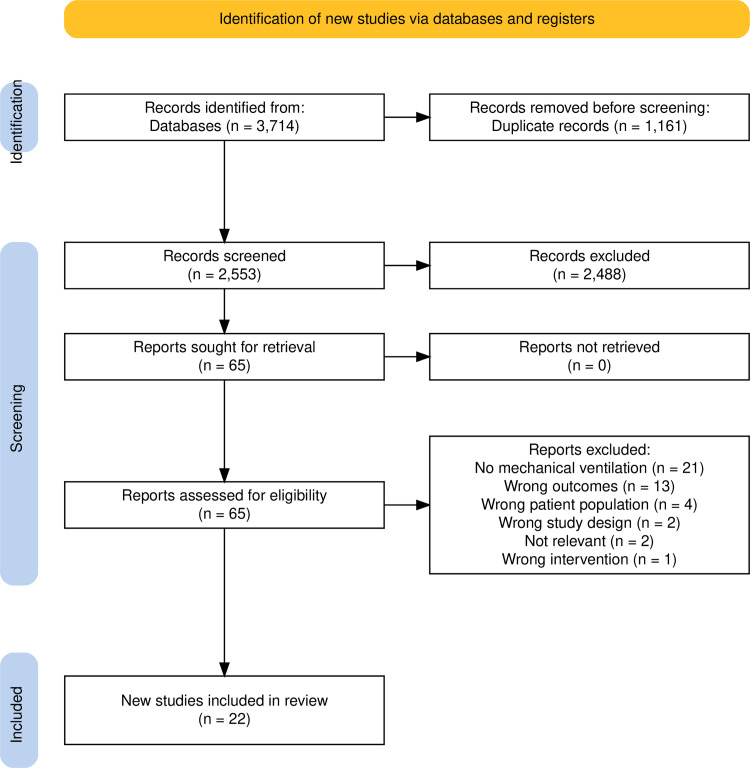 Fig 1
Fig 1- —http://dx.doi.org/10.13039/100016337Department for the Economy
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular and exercise physiology · Physical Activity and Health · Long-Term Effects of COVID-19
Introduction
After critical illness, reduced function, mobility, and strength may negatively impact quality of life and capacity to perform routine daily tasks [1–3]. In addition, patients often have difficulty achieving pre-illness physical activity levels [4]. These functional limitations are likely to prevent survivors of critical illness from achieving the recommended weekly levels of physical activity. Adults are recommended to undertake ≥150 mins of moderate intensity, ≥75 minutes of vigorous-intensity physical activity, or a suitable combination of both [5]. Guidelines also recommend a reduction in sedentary behaviour [5]. The effects of high levels of sedentary behaviour have been well documented, with sedentary behaviour having negative effects on health and increasing the risk of mortality in older adults [6,7]. Negative physiological effects of sustained levels of sedentary behaviour include insulin resistance, vascular dysfunction and a reduction in muscle mass and strength [8]. Reallocation of the length of time spent in sedentary behaviour into moderate to vigorous physical activity (MVPA) can result in health benefits, with researchers reporting that changes of as little as 4–12 minutes can be useful [9]. The consequences of critical illness, as well as excessive sedentary behaviour, have the potential to impact patients’ recovery and return to activity after hospital discharge. However, physical activity is not routinely measured in this population, and it is not clear which device/s should be used [10]. There is also limited data to quantify and describe levels of physical activity and sedentary behaviour after critical illness.
There is increasing awareness about the need to evaluate and promote rehabilitation and physical activity in the critical care population during and after hospitalisation [11]. A previous scoping review (n=7 studies) aimed to evaluate the use of wearable devices in the intensive care unit (ICU) and found that device-based physical activity measurement was used infrequently in people after critical illness [12]. However, this is an emerging area of research and several papers about physical activity after critical illness have been published since the Gluck at al. (2017) review [13,14]. Researchers and clinicians will need to be able to accurately assess physical activity and sedentary behaviour levels to identify activity patterns across the trajectory of recovery, evaluate the prevalence of physical activity engagement, and assess the effectiveness of interventions designed to change physical activity and sedentary behaviour. It is anticipated that this review will advance knowledge about device-based instruments, and any challenges for the measurement of physical activity and sedentary behaviour in this population. This review will inform the potential use and implementation of device-based measurement of physical activity and sedentary behaviour following critical illness in future research and in clinical practice.
Aims
This scoping review aimed to explore the current use of device-based physical activity instruments to measure physical activity and sedentary behaviour during and following critical illness. The objectives were, in patients following critical illness, to identify device-based instruments and the parameters used to describe patterns and levels of physical activity and sedentary behaviour, report device clinimetric properties; describe the relationship between physical activity and sedentary behaviour with other health-related outcomes and explore the levels and patterns of physical activity and sedentary behaviour across the trajectory of recovery.
Methods
We chose a scoping review as the most appropriate review method in order to synthesise the evidence to address specific questions relating to the device-based measurement of physical activity and sedentary behaviour [15]. The scoping review applied the framework by Arksey and O’Malley [16], which was further refined by Levac [17]. The methodology is described in the study protocol (published in advance https://osf.io/278mc/) and is reported according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) [18]. There was one deviation from the published protocol as two electronic databases, PubMed and Embase, were removed based on a recommendation from the subject librarian and were replaced with Scopus and ProQuest. This scoping review aimed to address the following questions:
What device-based instruments are currently used to measure physical activity and sedentary behaviour during and following critical illness?What parameters have been used to describe patterns and levels of physical activity and sedentary behaviour in patients following critical illness?What are the clinimetric properties (validity, reliability, responsiveness), user acceptability, and minimal clinically important differences (MCIDs) of device-based instruments to measure physical activity and sedentary behaviour specifically in patients following critical illness?What is the relationship between physical activity and sedentary behaviour with other health-related outcomes (e.g., quality of life, hospital readmission, exercise capacity, function and emotional status) in patients following critical illness?What are the levels and patterns of physical activity and sedentary behaviour in patients following critical illness across the trajectory of recovery?
Search strategy
The research team collaborated with a research librarian to develop the search strategy, including the selection of the databases and refining the keywords and phrases. A comprehensive search of four electronic databases (Medline, ProQuest, Scopus and CINAHL) was conducted using the agreed-upon search terms. Medical subject headings (MeSh) terms were expanded and included in the relevant databases (Supplement 1). The research team met to provide their experience and methodological expertise to further guide the identification of relevant studies.
Results were searched from inception to December 2023 and were limited to human research and English language.
Eligibility criteria
Studies which reported the outcome of physical activity or sedentary behaviour in survivors of critical illness or ICU were included. The full inclusion criteria were as follows:
Adult patients admitted to an ICU (≥18 years old).Patients who have been mechanically ventilated in ICU.Critically ill patients previously admitted to an ICU, e.g., medical, surgical, neurological, cardiac and trauma diagnoses.Physical activity monitoring that had commenced: during ICU stay, post-ICU discharge (on the ward) or post-hospital discharge.Included some form of device-based physical activity measurement used to assess “physical activity” and/or “sedentary behaviour”, including but not limited to accelerometers, pedometers, activPAL, ActiGraph, smartphone apps etc.
Study selection
The search results from each of the databases were imported into Covidence, which was used as a screening and data extraction tool. Duplicates were removed automatically. Each study title and abstract from the systematic search was screened by two independent reviewers [DM and AH] against the inclusion and exclusion criteria. The full text was retrieved for all of those that appeared to meet the inclusion criteria, and for those where there was insufficient information regarding whether the criteria were met.
All full-text papers were then independently reviewed by the two reviewers [DM and AH] to determine inclusion. Any disagreements were addressed via discussions, or with the consultation of a third reviewer [BON or JW] when required.
Data extraction and analysis
The studies were randomly divided between the two reviewers for completion of data extraction (DM & AH). The data were transferred to tables on an Excel database, which was drafted specifically to capture all the information required to answer the research questions. The data extracted included study characteristics, device details, parameters of physical activity and sedentary behaviour, correlations with other outcomes and levels of physical activity and sedentary behaviour. Once completed, the tables were reviewed by DM and AH to ensure all relevant data were captured and collated. Data were analysed descriptively by summarising and describing results that linked to the review questions. Thorough discussion took place among the review team to agree all results
Results
Study selection
The identification and selection of studies is summarised in Fig 1. There were 22 studies included.
Prisma flow diagram for selection of studies [19].
Study characteristics
Study characteristics are summarised in Table 1 (with further details in Supplemental S2 Table). The studies were undertaken in Europe (n=6), North America (n=8), South America (n=3) and Oceania (n=5). There was heterogeneity in the study designs utilised; the majority (n=12) were observational studies, with one randomised control trial [29], and one conference abstract [22] included. Studies collected data across the continuum of recovery, with the earliest timepoint occurring at awakening in ICU [13,25] through to 18 months post-hospital discharge [24]. The years of publication were 2005–2022.
Table 1: Physical activity devices including details of wear time, activity parameters and data processing per device.
Several studies (n=14) provided data at one time point only, while six provided data across two time points and two studies provided data at three or more time points. Control or comparator groups were included in four studies [29,23,24,37].
Population studied
Supplemental S2 Table summarises the characteristics of this heterogeneous population. Length of stay in the ICU varied from 4 [27] to 21 [28] days, and the duration of mechanical ventilation was reported in 17/22 (77%) studies. The population sample sizes in the included studies ranged between 8 [26] and 715 [37] participants.
Device-based instruments used to measure physical activity and sedentary behaviour
Eleven different devices were used across the 22 studies (Table 1). Actiwatch Spectrum (n=5), activPAL3 (n=3) and the SenseWear armband (n=3) were the most commonly used devices. Location worn was dependent on the device used, and when reported, the most common was the wrist (n=9), thigh (n=4), and ankle (n=4). Ten studies reported device placement: this was on the dominant (n=6) or non-dominant limb (n=5). Wear-time duration was reported in 18/22 studies (81%). Wear-time duration varied depending on the aims of the study. When validation studies were excluded, wear-time ranged from two hours [20] to 14 days [37]. In studies where accelerometry was used for more than one day, for analysis the parameters for a valid day varied from a minimum of 8 hours of data per day [25] to ≥90% of on-body time per day for ≥5 days [24].
The sampling frequencies used varied across studies, with many not reporting this (n=16), while other studies used 20–30 Hz (n=4), 50 Hz (n=1) and 90 Hz (n=1). Epoch length also varied, with the majority of studies not reporting this (n=12), while 60-second (n=4), 5-second (n=2), 15-second (n=2) and 30-second (n=1) epochs were reported in the other studies (Table 1).
Parameters to describe patterns and levels of physical activity and sedentary behaviour
Various parameters (n=4) have been used to describe the levels of physical activity and sedentary behaviour, including step counts, activity counts, time in activity (total daily time, percentage of time, and number of bouts), and intensity of physical activity (Table 1).
Clinimetric properties of the device-based instruments
Clinimetric properties were measured in five studies [25,24,26,28,36] (Table 1). Validity was assessed in three studies [24,26,28]. The ActivPAL demonstrated good validity when recording sit-to-stand transitions, time spent standing and sedentary behaviour when compared to direct observation, however, the validity of the ActivPAL to record step counts could not be confirmed [26]. In the hospital ward following ICU discharge, an ankle-placed ActiGraph was valid in measuring step counts, with the intraclass correlation (ICC) equalling 0.99, while step counts were shown to be underestimated using a thigh-worn device [28]. Accelerometry-measured step counts were shown to be a valid method of assessing frailty and health-related quality of life (HRQOL), with no floor or ceiling effect using the SenseWear device [24].
Reliability and responsiveness were not reported in any of the studies. Also, no studies reported on the minimal clinically important difference (MCID) for any metric with physical activity or sedentary behaviour. User acceptability was reported in three studies [25,24,36]. The SenseWear device was well-tolerated by participants [24] with 97% of participants wearing it for five days in the ICU [25]. The Axivity device was pilot tested on five participants, with no adverse effects noted while wearing it [36].
Association of physical activity and sedentary behaviour with other health-related parameters
Physical activity data were compared to other health-related outcomes in 15/22 studies (68%) (S3 Table).
Physical function.
Eight studies [13,14,22,24,25,29,27,33] showed positive correlations between physical activity levels and physical function. However, Rollinson et al. [38] did not show any significant associations. In addition, Baldwin et al. [13] showed there was no association between sedentary behaviour and physical function [13].
Exercise capacity.
A strong correlation was reported between physical activity and exercise capacity in the ICU and in the ward (r=0.728; p<0.001) [38].
Muscle strength.
Less time sitting or lying, more minutes spent upright and an increased number of STS transitions were associated with better muscle strength (MRC-ss and handgrip) at ICU discharge, however, there were no associations found at hospital discharge [13]. There was a positive association between post-ICU daytime activity and grip strength (r²=0.689, p<0.001) [33].
HRQOL.
Daily step count was shown to correlate with the physical function component of the SF-36 (r²=0.51; p<0.01) and a weaker correlation (r²=0.25; p<0.01) was shown with the physical component score of the SF-36 [24].
Hospital LOS.
Two studies [13] and [22] showed no associations between physical activity and/or sedentary behaviour and hospital length of stay, however, Elias and colleagues showed there was a significant relationship between post-ICU daytime activity and LOS [34].
Other.
Moderate correlations were shown between the Riker Sedation and Agitation scale (SAS) (rho=0.601; p<0.005) and the Richmond Agitation Sedation Scale (RASS) r=0.58 & r=0.52) and physical activity levels [22,20].
Lower levels of symptom severity, excluding cognition and anxiety, were associated with physical activity (p<0.05), with those experiencing the most severe acute illness having 1–2 mg lower volume of physical activity (p=0.045) and less time spent in MVPA (p=0.032) [37].
No studies explored the association between physical activity and/or sedentary behaviour with hospital readmissions.
Levels and patterns of physical activity and sedentary behaviour
Physical activity and sedentary behaviour patterns were reported from awakening in ICU [25,26] up to 18 months post-discharge [24] in Table 2.
Table 2: Measured Physical Activity and Sedentary Behaviour.
Step counts.
Step counts were reported in 8/22 studies [14,22–25,29,26,28] Step counts were initially low but increased progressively from ICU to hospital discharge and home recovery. After awakening in ICU, ambulation was almost non-existent, with a median of four steps/day [25]. Daily step counts gradually increased to 95 at three days before ICU discharge, and 257 three days before hospital discharge [14]. There were minimal increases in daily step counts from 1,223 steps at three days and 1,278 steps up to eight days after hospital discharge [14]. At 18 months post-hospital discharge, daily step counts had risen to 5,803 steps, which was still significantly lower (p<0.001) than healthy age-matched controls (i.e., 11,735 steps) [24].
Activity counts.
Activity counts were reported in nine studies [20,21,27,31,33,30,32,34,35]. At awakening, a mean of 31,590 counts per day was reported, increasing to a mean of 50,483 counts per day at ICU discharge [30]. Activity counts averaged 2,233 per hour, within 24–48 hours of ICU discharge, where 1,140 counts per day equate to resting or lying down while awake [32]. Following discharge from the ICU, mean activity counts during the daytime (07:00-16:00) were shown to be 43,699 [27].
Eight studies reported on the time spent being physically active [13,22,25,37,36,38,30,39]. During the ICU admission, time spent being physically active was low, with values of 17.8, 16.8 & 9.3 minutes per day [22,25,30]. This time increased at ICU discharge to 35.5 minutes per day [30], and to the hospital ward was 52.8 minutes per day [38]. A similar trend was shown by Baldwin [13] and colleagues, where time spent being physically active (>200g/min) increased from awakening (27 minutes) to 61 minutes at ICU discharge and to 96.8 minutes at hospital discharge [13].
Sedentary behaviour.
Sedentary behaviour was reported in eight studies [13,29,23,37,31,36,30,39]. These studies show the trajectory and change in sedentary behaviour over time, from awakening in the ICU [13,30] to eight months post-hospital discharge [37]. High levels of sedentary behaviour and inactivity were reported in the ICU. At awakening, Baldwin et al. [13] reported that their participants spent 98.1% of their time sedentary.
At ICU discharge, many participants typically spent 97.5% of their day being inactive [30]. Those in the study by Baldwin et al. [13] reduced their percentage of time spent inactive to 95.7% at ICU discharge, while this number reduced further to 93% at hospital discharge. At three months post-hospital discharge, sitting or lying time was reduced to 58% (from 89.2% in the hospital ward) by those observed by Borges et al. [23].
Discussion
This scoping review has demonstrated that a wide range of devices have been used to measure physical activity and sedentary behaviour. There is a clear lack of standardisation regarding the data processing methods and there are no consistent parameters used when reporting physical activity levels or sedentary behaviour. There are some associations between physical activity and other outcomes such as physical function, strength, and exercise capacity. Overall, in people who have been admitted to ICU for critical illness, the levels of physical activity are generally low in ICU, on hospital wards and in the 18-month period after hospital discharge.
Device-based instruments used to measure physical activity and sedentary behaviour
The most common devices used to measure physical activity and sedentary behaviour included the Actiwatch Spectrum, activPAL and SenseWear Armband. This finding reflects the wider literature related to accelerometry measurement in various clinical populations. However, researchers and clinicians should also be aware of the strengths and weaknesses of each of the devices. For example, a thigh-worn activPAL device may be more suited to tracking and recording sedentary behaviour and transitions from various positions, while potentially underestimating step counts [13]. If the goal is to measure positional changes, choosing this device or similar would be more appropriate. Future literature to support the use of a particular device and the protocols for wearing the device, including for example, location worn, should be based on research in the critical care population as opposed to healthy populations or other cohorts to be most applicable [40,41]. While various accelerometers have been utilised in individuals admitted to ICU, it is important for researchers and clinicians to be aware that there is likely to be a certain amount of measurement error with each device. For example, Baldwin and colleagues [26] compared activPAL-measured outcome variables with direct observation in ICU survivors. The authors found that although sit-to-stand transitions, sedentary behaviour and upright time were well-recognised by the activPAL, there were under-estimations of standing and stepping time compared to direct observation (22% and 19%, respectively). In healthy populations, free-living step counts have been shown to vary across seven activity monitors by around 1,700 steps/day (ranging from 1265 to 2275 steps/day) [42]. This shows that even though two activity monitors are supposedly measuring the same variable, there are likely to be error margins to consider. Unfortunately, few studies have currently explored validity and reliability of different devices in ICU survivors.
Parameters of physical activity and sedentary behaviour
There are inconsistencies across the studies when defining physical activity and sedentary behaviour, the intensity of activity, and the thresholds used for the analysis of data on sedentary behaviour, making comparisons between studies difficult [43]. For the measurement of physical activity and sedentary behaviour, specific activity counts, milligravity (mg) units and METs have all been used. For METs, previous research has determined a cut-off point of <1.5 METs to define levels of sedentary behaviour, while 3 METs is commonly used as the cut-off point of LIPA/MVPA [44–46]. Survivors of ICU are often left with reduced exercise capacity and reduced levels of oxygen consumption, possibly due to mitochondrial dysfunction [47]. Therefore, it may be more appropriate to use lower MET values, such as those used in older populations, which could be as low as 2.8 ml/O2/kg [48–50] to avoid underestimation of the intensity of effort [51]. This was considered in one study [25], where a value of 1 MET was used (as opposed to 1.5 METs) as the threshold for physical activity. There are also other processing decisions that must be considered, such as epoch length, device placement and sampling frequency.
An epoch is defined as the time-period which allows data to be grouped together for analysis and usually varies from 1–60 seconds. Using different epoch lengths can affect the results by either over- or under-estimating physical activity and sedentary behaviour [52,53]. For example, the use of a 10-second epoch has been shown to increase the total daily sedentary behaviour time of older adults by almost 80 minutes when compared to a 60-second epoch [53]. The optimal epoch length for data analysis for assessing device-based physical activity within the critical care population has not been determined. In addition, the location the device is worn (e.g., thigh, wrist) alongside the dominant/non-dominant side worn have been shown to impact on important physical activity parameters, such as step counts. For example, daily steps have been shown to be significantly different between wrist and hip locations in adults wearing a pedometer [54], while another study [55] demonstrated dominant wrist placement resulted in 1,253 more daily steps compared to the non-dominant side (p=0.006).
The use of various sampling frequencies can also have an impact on the results and classification of physical activity and sedentary behaviour [56–58]. When using an ActiGraph GT3X, it has been recommended to use multiples of 30Hz [56,58], however, it is worth noting that using multiples of 30 may lead to filtering out of signals generated by vigorous activity and may result in an underestimation of vigorous activity [56].
The current heterogeneous approach to selecting and reporting parameters for the measurement of physical activity and sedentary behaviour is a clear limitation of the existing body of research, as this impacts on the ability to compare and contrast study results or undertake meta-analysis. There is a need to clearly define and establish cut-points across the different MET thresholds, epoch lengths and sampling frequencies for analysis of physical activity data that relate to ICU survivors, as this would lead to a more consistent approach to measuring and reporting physical activity and sedentary behaviour. Table 3 provides a summary of some considerations and suggestions to help guide the use of device-based measurement in future critical care research and practice.
Table 3: Practical considerations and suggestions to guide device based physical activity measurement and analysis for the critical care population.
To overcome the challenges of measuring step counts in those with slow gait speed, and misclassification with standing, a low-frequency filter may be used (LFE). However, it is important to note that the use of a LFE may end up being overly sensitive. Some studies have demonstrated inflated step counts in adults when using the LFE [53,66,67], in some instances by up to 5,502 steps per day [53,66]. It is worth noting that Anderson et al. [28] used a LFE filter and concluded it provided a valid measurement of step counts from an ankle-worn ActiGraph in hospital inpatients recovering from critical illness. In line with the recommendations for the COPD population, validation of devices to accurately measure step count using the LFE should be determined before use in the critical illness population [67].
Decisions on minimum daily wear time also need to be carefully considered, to appropriately represent activity and sedentary data while also maintaining sample sizes [53,58]. A valid daily wear time of ≥600 minutes (Table 3) has been suggested [53], and the results of this review show that only four studies met this criterion [13,24,37,36].
Clinimetric properties
An understanding of the clinimetric properties of devices used in the ICU population is important to help guide the selection of the appropriate device for research. While studies have shown promise in validating devices for the critical care population when used under controlled conditions [13,28], researchers also cite validation studies from other populations (COPD, older adults) and this might not be the best approach. No studies in this review reported an MCID for physical activity or sedentary behaviour variables in this population, making it difficult to establish the change that is important to the patient or to establish the clinical effectiveness of an intervention [68,69]. This gap needs to be addressed in future research.
Relationship between physical activity and sedentary behaviour with other health-related outcomes
In this review, levels of physical activity were shown to correlate with physical function, which provides evidence of the validity of physical activity as a construct [13,14,22,24,25,29,27,33]. However, correlations between physical activity and other outcome measures such as cognitive function and frailty, that are recommended in core outcome sets, have not been extensively studied [70]. It is worth noting that not all studies showed significant correlations of physical activity with all the same health-related outcome measures. Potential reasons for this could be down to the specific device which was used in each study, but also the test used to collect the health-related outcome measure. For example, physical function was measured using a battery of four tests by Rollinson et al. [38], while Estrup et al. [27] used the Chelsea Critical Care Physical Assessment tool (CPAx) which assesses ten aspects of physical function. These two studies had contrasting findings when it came to the association of physical function with physical activity.
Levels of physical activity and sedentary behaviour
Physical activity levels in ICU survivors are low compared to healthy populations, even up to 18 months post-discharge [24], with a high prevalence of sedentary behaviour. This could contribute to the negative long-term effects of sedentary behaviour that have been well-documented [8]. While it is important to increase levels of physical activity in ICU survivors [11], efforts should also be made to encourage less sedentary behaviour where possible [71,72]. Prolonged periods of sedentary behaviour when recumbent (lying) may result in little-to-no activity counts being recorded on the device and may give the impression of sleep. Similar challenges were found in the COPD population, and the algorithm developed for using the ActiGraph wGT3X-BT accelerometer to help determine when the person may be sleeping or indeed waking up could be useful [62].
Only one of the 22 included studies was a randomised control trial investigating the effect of an intervention (a mobility programme) on physical activity in a cohort of patients within 48 hours of admission to ICU [18]. Improvements reported in the study were consistent with findings supporting the benefits of early mobilisation in the ICU [73], therefore, accelerometry could be an applicable outcome in future research exploring effects of early mobilisation in the ICU or investigating the effectiveness of rehabilitation interventions after ICU discharge. High-quality experimental studies are required to establish cause and effect relationships between physical activity and sedentary behaviour with important patient outcomes. At present, nearly all research is observational in nature. Therefore, there is a clear need for future experimental studies exploring the impact of changing physical activity and sedentary behaviour on important patient outcomes. Investigation is also needed to test the best way to support recovery of physical activity and reduction of excessive sedentary behaviour following discharge from hospital.
The strengths of this scoping review include a comprehensive search strategy and pre-identified rigorous methodology (15,16) as well as the inclusion of studies across the entire recovery trajectory following ICU. The review protocol was registered a priori to ensure transparency. Limitations of this scoping review were that we did not contact authors to ask whether further details about their data processing could be made available and our results were limited by the lack of a standardised approach to measurement used in the included papers making it difficult to compare across studies.
In future, researchers and clinicians will need to be able to select appropriate device-based physical activity instruments to accurately assess physical activity and sedentary behaviour. This review highlights the devices that could be used and the associated challenges. There are some existing guidelines for the assessment of physical activity in other populations [59,60]. There is a clear need for an agreed protocol(s) to guide the processing and analysis of data for the critical care population, therefore, to address this limitation, we have made some practical suggestions/recommendations that researchers and clinicians could use until such evidence-informed guidelines are available (Table 3). Future research may also benefit from the use of machine learning to develop protocols and assist in differentiating between different physical activity behaviours/patterns [74].
Conclusion
The use of device-based physical activity measurement in critical illness is an active and evolving research area. A serious issue we have highlighted is that there appears to be inconsistent reporting and usage of various physical activity and sedentary behaviour parameters related to accelerometry in critical illness. This review supports the need for the development of a strategy or protocol to guide the future use of devices and standardise processing and analysis when assessing physical activity and sedentary behaviour in the population with critical illness. In addition, there is a need for researchers to establish the typical MET values required for completing common types of physical activity specifically in this population, in order to guide more effective physical activity prescription. Physical activity levels remain low in both ICU and following ICU discharge, and investment is needed to support recovery of physical activity and reduce sedentary behaviour following discharge from hospital.
Supporting information
S1 TextSearch strategy.(DOCX)
S2 TableStudy characteristics.(DOCX)
S3 TableCorrelations device measured physical activity and other health outcomes measured.(DOCX)
S4 TextPRISMA-ScR Checklist.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pfoh ER, Wozniak AW, Colantuoni E, Dinglas VD, Mendez-Tellez PA, Shanholtz C, et al. Physical declines occurring after hospital discharge in ARDS survivors: A 5-year longitudinal study. Intensive Care Med. 2016;42(10):1557–66. doi: 10.1007/s 00134-016-4530-1 27637716 · doi ↗ · pubmed ↗
- 2Hopkins RO, Suchyta MR, Kamdar BB, Darowski E, Jackson JC, Needham DM. Instrumental activities of daily living after critical illness: A systematic review. Ann Am Thorac Soc. 2017;14(8):1332–43. doi: 10.1513/Annals ATS.201701-059SR 28463657 PMC 5566273 · doi ↗ · pubmed ↗
- 3Rai R, Singh R, Azim A, Agarwal A, Mishra P, Singh PK. Impact of critical illness on quality of life after intensive care unit discharge. Indian J Crit Care Med. 2020;24(5):299–306. doi: 10.5005/jp-journals-10071-23433 32728319 PMC 7358873 · doi ↗ · pubmed ↗
- 4Nedergaard HK, Haberlandt T, Reichmann PD, Toft P, Jensen HI. Patients’ opinions on outcomes following critical illness. Acta Anaesthesiol Scand. 2018;62(4):531–9. doi: 10.1111/aas.13058 29315454 · doi ↗ · pubmed ↗
- 5Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020;54(24):1451–62. doi: 10.1136/bjsports-2020-102955 33239350 PMC 7719906 · doi ↗ · pubmed ↗
- 6de Rezende LFM, Rey-López JP, Matsudo VKR, do Carmo Luiz O. Sedentary behavior and health outcomes among older adults: A systematic review. BMC Public Health. 2014;14:333. doi: 10.1186/1471-2458-14-333 24712381 PMC 4021060 · doi ↗ · pubmed ↗
- 7de Rezende LFM, Rodrigues Lopes M, Rey-López JP, Matsudo VKR, Luiz O do C. Sedentary behavior and health outcomes: an overview of systematic reviews. P Lo S One. 2014;9(8):e 105620. doi: 10.1371/journal.pone.0105620 25144686 PMC 4140795 · doi ↗ · pubmed ↗
- 8Pinto AJ, Bergouignan A, Dempsey PC, Roschel H, Owen N, Gualano B, et al. Physiology of sedentary behavior. Physiol Rev. 2023;103(4):2561–622. doi: 10.1152/physrev.00022.2022 37326297 PMC 10625842 · doi ↗ · pubmed ↗