First Experiences of Patients and Healthcare Professionals with Routine Use of Patient-Reported Outcome Measures for Venous Thromboembolism
Cindy M.M. de Jong, Sophie N.M. ter Haar, Willem Jan W. Bos, Paul L. den Exter, Menno V. Huisman, Marlon H.C. Kosterink, Thijs E. van Mens, Frederikus A. Klok

TL;DR
This study explores how patients and healthcare professionals experience using patient-reported outcome measures for venous thromboembolism in routine care.
Contribution
The paper presents initial experiences and feedback on integrating PROMs into VTE outpatient care through a digital tool.
Findings
Most patients and professionals viewed the use of PROMs as neutral to positive.
Patients suggested reducing the number of questions and improving the digital tool.
PROMs were seen as adding value to appointment preparation and consultations.
Abstract
Venous thromboembolism (VTE) can considerably limit patients' functioning and quality of life. Using patient-reported outcome measures (PROMs), the full impact of VTE on individual patients can be captured. To evaluate the experiences of patients and healthcare professionals with the routine use of PROMs for VTE patients visiting the outpatient clinic, a mixed-methods study was performed at Leiden University Medical Center, the Netherlands. VTE PROMs were incorporated into routine care since March 2023, through a digital application sending patients invitations to complete PROMs. Quantitative and qualitative data were obtained from semi-structured interviews with patients and involved healthcare professionals. The NoMAD (normalization measure development) questionnaire was used to assess the implementation process from the professionals' perspective. Patients aged ≥18 years who…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1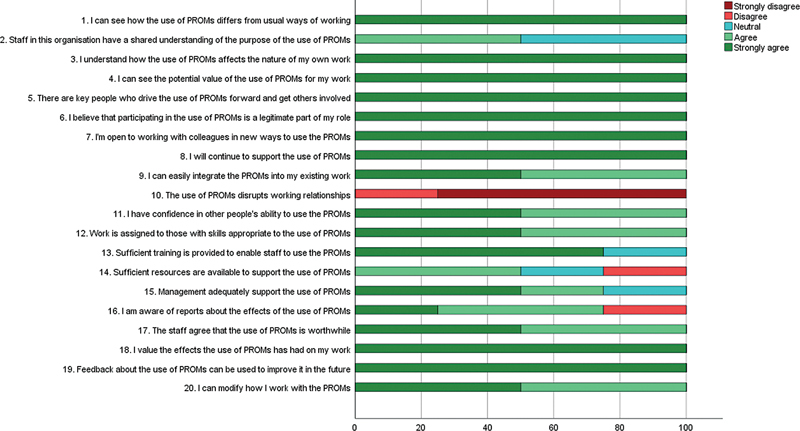 Fig. 2
Fig. 2| Patient-centered outcome | Patient-reported outcome measure |
|---|---|
| Quality of life | PROMIS Scale v1.2—Global Health |
| Functional limitations (including ability to work) | Post-VTE Functional Status Scale |
| Pain (including symptom severity) | PROMIS Short Form v2.0—Pain Intensity—3a |
| Dyspnea (including symptom severity) | PROMIS Short Form v1.0—Dyspnea Severity—10a |
| Psychosocial wellbeing | Patient Health Questionnaire (PHQ-9) |
| Satisfaction with treatment | Single question: “Are you satisfied with your VTE treatment?” |
| Changes in life view | Single question: “Have you experienced a change in your expectations, aspirations, values, or perspectives on life opportunities since the diagnosis of VTE?” |
| Patients who completed PROMs | 1. What is your experience with filling out the questionnaires? On a scale of 1 to 5 (1 negative, 5 positive)? |
| 2. How much time did you need to complete the questionnaires? | |
| 3. The number of questions was a. too few, b. too many, c. just right | |
| 4. The next three questions are about the questionnaires | |
| 5. Did the care provider follow up on the responses you provided in the questionnaires? | |
| 6. Did you experience that attention was paid to the symptoms and/or issues you wanted to discuss during the appointment? | |
| 7. Did you feel prepared for the appointment after completing the questionnaires? On a scale of 1 to 5 (1 not at all, 5 very well prepared)? | |
| 8. Do you have any suggestions for improvement? | |
| Patients who did not complete PROMs | 1. Did you start filling out the questionnaires, or were you unable to start the questionnaires? |
| 2. What caused you not to complete the questionnaires? | |
| 3. What would have prompted you to fill out the questionnaires? | |
| 4. Did you experience that attention was paid to the symptoms and/or issues you wanted to discuss during the appointment? | |
| 5. Did you feel prepared for the appointment? On a scale of 1 to 5 (1 not at all, 5 very well prepared)? | |
| Professionals | 1. How many patients at your outpatient clinic have completed PROMs? |
| 2. What is your experience with the use of PROMs? On a scale of 1 to 5 (1 negative, 5 positive)? | |
| 3. Did you use PROMs during preparation for the patient appointment and/or during the appointment? | |
| 4. What is your perception of the value of the use of PROMs at the outpatient clinic? And specifically, during the preparation for the patient appointment, and during the appointment? On a scale of 1 to 5 (1 none, 5 significant added value)? | |
| 5. What could be improved about the PROMs, implementation, and/or use in practice? |
| Characteristics |
Patients who completed PROMs (
|
Patients who did not complete PROMs (
|
|---|---|---|
|
Female (
| 2 (40) | 2 (67) |
| Age, in y (median, range) | 54 (34–75) | 59 (48–84) |
|
Venous thromboembolic event (
| ||
| –Acute pulmonary embolism | 4 (80) | 1 (33) |
| –Acute deep vein thrombosis | 1 (20) | 2 (67) |
| Theme | Shared experience |
|---|---|
| Patients' experiences | |
| Completion of the PROMs | –User-friendly |
| Relevance of the questions | –The questions also reveal things I would not have thought of |
| Purpose of the PROMs | –Makes you wonder why you are filling this out |
| Communication between patient and care provider, from the patient's perspective | |
| Follow up on responses to the questionnaires during the appointment | All five patients had experienced that the care provider did not follow up on the responses to the questionnaires during the appointment, but also none of them initiated a conversation about the questionnaires themselves; three patients did not feel the need to do so, and one patient did not know that the doctor was aware of the questionnaires. |
| Attention to symptoms and/or issues | –Pleasant experience, everything was discussed without me having to initiate anything |
| Preparation of the patient for the appointment | |
| Better prepared after completion of the PROMs | –I gained insights from some of the questions, there were questions where I thought “could that also be related,” or where I wanted to ask about during the appointment |
| Not better prepared after completion of the PROMs | –I felt prepared regardless of the questionnaires |
| Professionals' experiences | |
| Impression of the patient's well-being | –PROMs provide valuable insights, focusing on physical and social aspects, which help understand the patient's condition; I find the responses entrusted to be very useful |
| Direction of the conversation | –The PROMs provide insights that could guide the conversation |
| Value of use of PROMs | –PROMs allow to better help patients, to pay more attention to what is important to them |
| Application of the PROMs by professionals | |
| Preparation of the appointment | All four professionals used the PROMs during their preparation of the consultation. |
| During the appointment | Three professionals used the PROMs during the appointment. |
| Note in the medical records | –The responses to PROMs are implicitly part of my documentation |
| Interpretation of the PROM responses | –Interpretation of the PROMs in the dashboard is good, the scores and colors are clear |
| Topic for improvement | Suggestions and considerations |
|---|---|
| Completion of the PROMs | –The option to fill out the questionnaires at the outpatient clinic would be convenient; for instance, completing PROMs on a tablet in the waiting room, potentially with the help of a volunteer (P, HCP) |
| Accessibility for patients | –Clear instructions on where the questionnaires can be filled out (P) |
| Purpose of the PROMs and relevance to the patient | –Adding a sentence to the appointment letter, to announce that an invitation link will be sent (HCP) |
| Content of the PROMs | |
| Shortening the questionnaires | –Reduce the question load (HCP) |
| Modifications to the PROMs | –Adding questions about the effectiveness of the medication and about side effects (P) |
| Accessibility for professionals | –All professionals who work with PROMs should have access to the dashboard (HCP) |
| Timing | –Timing of the PROMs measurements; attention to proper alignment between the invitation links and the appointments (HCP) |
| Digital PROMs application | |
| Technical aspects | –Manual activation/deactivation of PROMs invitations (HCP) |
| Interpretation of the PROM responses | –Cleaner layout (HCP) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVenous Thromboembolism Diagnosis and Management · Diagnosis and Treatment of Venous Diseases · Acute Ischemic Stroke Management
Introduction
After experiencing deep vein thrombosis (DVT) or acute pulmonary embolism (PE), patients may encounter a wide spectrum of health effects and long-term consequences. 1 2 3 4 5 6 7 8 Venous thromboembolism (VTE) and its sequelae may affect both physical and psychosocial functioning, considerably limiting patients' ability to work, psychological well-being, and quality of life. 9 10 11 12 13 14 15 16 17 Assessment of patient-centered outcomes may therefore contribute to a better understanding of the impact of the venous thromboembolic event on individual patients, help guide the agenda for the consultation, and tailor management decisions to the patient's needs and values. Such outcomes can be measured using patient-reported outcome measures (PROMs). PROMs are standardized questionnaires that are completed by patients, to assess their symptom burden, perceived health status, and well-being, capturing outcomes of care and the impact of disease from the patient's perspective. 18 19 20 Routine use of PROMs could empower patients to make informed healthcare decisions. 18 21 Moreover, complementing traditionally measured clinical outcomes with patient-reported outcomes is an important step toward patient-centered health care. 22
To facilitate the use of patient-centered outcomes in daily clinical practice, the multidisciplinary ICHOM-VTE project (International Consortium for Health Outcomes Measurement project for VTE) established a standardized set of patient-relevant outcome measures for patients with VTE. 23 During a modified Delphi process, an international working group consisting of VTE experts as well as patient representatives selected the outcomes that were considered to matter most to patients. This set of outcomes along with recommended outcome measures, including PROMs, resulted from a thorough process of development with the engagement of patient representatives and was designed to apply to all patients diagnosed with VTE aged 16 years and older. The PROMs that are part of this core set of outcomes have been embedded in routine care at the thrombosis outpatient clinic of the Leiden University Medical Center (LUMC; the Netherlands). Important lessons can be learned from the implementation process and the first experiences of patients and healthcare professionals. The aim of this study was to assess the feasibility of PROMs completion and experiences with the routine use of PROMs for VTE patients treated in our center.
Methods
Setting
PROMs for adult VTE patients have been incorporated into our routine patient pathway since March 2023. During the implementation phase, PROMs based on the outcome measures that were selected during the ICHOM-VTE project ( Table 1 ) were implemented using a digital application (Brightfish), which is integrated into the electronic health records system. 23 With the use of this digital tool, an invitation link is sent to the patient by email ahead of the scheduled appointment at the outpatient clinic. The link leads the patient to an online page where the questionnaires can be completed. This allows the patients to fill out the PROMs at home before their visit to the outpatient clinic. All patients who experienced VTE and had a scheduled first appointment at the thrombosis outpatient clinic were sent an invitation link to complete PROMs.
PROM results are immediately visible in a dashboard within the electronic medical records facilitated by the embedded digital tool, displaying the results in an intuitive way ( Fig. 1 ). Healthcare professionals can access the dashboard to review the completed questionnaires and graphical display of PROM results, which helps to interpret the responses and visualizing the course of PROM results when multiple measurements become available during follow-up. The PROM results can be used to optimally prepare for the patient appointment, as well as to guide the conversation with the patient during the consultation.
PROMs dashboard in the electronic medical records. Example of the dashboard in the electronic medical records (in the Dutch language), showing the summary of PROM results per questionnaire (above in the figure) along with a graphical display (below in the figure). The answers to each of the questions of the completed questionnaires can also be reviewed in the dashboard. Note: in our center, the PROMIS short form “Physical Function” (left in the figure) and short form “Ability to Participate in Social Roles and Activities” (right in the figure) were implemented, which contain additional questions about physical health and social activities and roles compared to the PROMIS short form “Global Health” to delve deeper into these domains. PROMs: patient-reported outcome measures.
The first invitation to complete PROMs is sent out to patients 1 week before the first follow-up contact, which is scheduled around 7 to 10 days following the VTE diagnosis according to the local patient pathway. Following the first measurement time point (T0), the PROMs are scheduled by the digital tool at fixed time points: patients receive invitations after 3 months (T1), after 6 months (T2), at 1-year follow-up (T3) and then yearly up to 3 years after the VTE diagnosis, for as long as the patient is under care. For the first time point (T0), the questionnaires could be answered 1 week before the first visit until 1 week after the visit. From the second time point (T1) onward, a 2-week window around the measurement time point was applied for the questionnaires to be open.
Design
The objective of this study was to evaluate the feasibility of the completion and application of PROMs and experiences with the use of PROMs in routine care for patients with VTE visiting our outpatient clinic. We aimed to assess the experiences of both patients and involved healthcare professionals. Evaluation of the scores and results of the PROMs was not within the scope of the current study.
A mixed-methods study was performed utilizing both quantitative and qualitative data. Quantitative data were obtained from statistics recorded by the digital PROMs tool, from 5-point Likert scale questions applied in semi-structured interviews with patients and healthcare professionals, and from the NoMAD (normalization measure development) questionnaire completed by healthcare professionals. 24 25 Qualitative data were obtained from semi-structured interviews with patients and healthcare professionals. The Institutional Review Board of the LUMC approved the study (protocol 132775).
Participants
Patients aged 18 years and older who were diagnosed with acute PE and/or DVT of the lower or upper extremity and received follow-up for at least 3 months at the outpatient clinic were identified in September 2023 based on scheduled appointments. Patients who completed PROMs at the first two time points (around 7 to 10 days after VTE diagnosis [T0] and after 3 months [T1]) were asked to participate in a semi-structured interview, as well as patients who were invited but did not complete PROMs at both follow-up time points. Patients were asked for consent to the use of demographic and clinical data from the electronic medical records for the purpose of this evaluation study.
A convenience cohort of four healthcare professionals in various roles (nurse, resident internal medicine, fellow vascular medicine, and internist specialized in vascular medicine) who worked with PROM results at the outpatient clinic were interviewed about their experience with the use of PROMs. The same healthcare professionals were asked to complete the NoMAD questionnaire to assess the implementation process from their perspective.
Data Collection
Semi-structured interviews were conducted by one researcher (CdJ) in the Dutch language. Questions were asked in a fixed order, according to an interview guide that was prepared for this evaluation study ( Table 2 ). Patients who had completed PROMs were interviewed on their experiences with the PROMs in practice, including their experiences with the completion of the questionnaires and their experiences during the outpatient clinic visit. Patients who had not completed PROMs after invitations at the two-time points were interviewed about their experiences around the PROMs and during their outpatient clinic visit too. There was no established relationship between the interviewer and the patients prior to the start of the interview. Demographic and clinical data were collected from the electronic medical records. Healthcare professionals were interviewed on their experiences with the use of PROMs in preparation for the patient appointment and during the appointment, and their perception of the value of the use of PROMs at the outpatient clinic. Field notes were made during all interviews.
In addition, to assess the implementation process from the perspective of involved healthcare professionals, the NoMAD questionnaire was used. This instrument was developed based on the normalization process theory (NPT) which explains the normalization of changes (a new intervention becoming part of normal practice) and was validated for the assessment of staff perceptions of implementation processes. 24 25 Four constructs proposed by the NPT are measured with the NoMAD instrument: coherence, cognitive participation, collective action, and reflexive monitoring. 25 26 In the current study, the Dutch translation of the NoMAD questionnaire was used. 27
Data Analysis
Demographic variables of patients who were interviewed, completion rate, and quantitative data obtained with the interviews and NoMAD questionnaire were analyzed using descriptive statistics. The interviews were thematically analyzed. Themes were derived and identified from the data, and were described along with illustrative examples. All analyzes were performed using SPSS version 29.
Results
Completion Rate
From March to September 2023, 27 patients who had received follow-up for at least 3 months at the outpatient clinic (as identified per September 2023) received invitations to complete PROMs at the first (T0; 7 to 10 days after VTE diagnosis) and second-time point (T1; after 3 months). In response to the T0 invitation, PROMs were completed by 13/27 (48%) patients. At T1, 11 (41%) patients had completed the PROMs. PROMs were fully completed at both time points by five patients.
Patients
Five consecutive patients who had completed PROMs at both time points were interviewed. Three patients who had not completed PROMs at any time point were interviewed as well. The eight interviewed patients (50% female) had a median age of 57 years. Five had been diagnosed with acute PE while three had experienced acute DVT (of the five patients who completed PROMs, four had experienced acute PE and one acute DVT; Table 3 ).
Experiences of Patients with Completing PROMs
Patients who did complete PROMs at the T0 and T1 time points were asked about their experience with completion of the PROMs on a scale from 1 “negative” to 5 “positive”, and were neutral to positive (range: 3.0–4.5; two expressed 3.0 referring to neutral). A summary of the patients' experiences with the PROMs, illustrated with examples, is provided in Table 4 . Three of the five patients felt that all questions were clear, of whom one stated that the questions were “understandable for everyone”. However, one patient felt that questions were confusing and found it difficult to determine whether symptoms were due to the thrombosis or comorbidities. Four out of five patients expressed that the number of questions was too high; one patient stated not to remember the length of the questionnaires.
Preparation for the Outpatient Clinic Visit
Two patients indicated that completion of the PROMs added to the feeling of being prepared for the visit; one of them described that some questions made her think about her situation and what she wanted to ask about. Of the other patients, two did not feel prepared for the outpatient clinic visit despite completing the questionnaires, and one felt prepared regardless of the PROMs. On a scale from 1 “not at all prepared” to 5 “very well prepared”, two patients felt not prepared at all, one patient expressed a neutral stance, and one patient felt very well prepared (range: 1.0–5.0).
The three patients who did not complete PROMs reported feeling neutral to very well prepared for the outpatient clinic visit (range: 3.0–5.0).
Experiences of Healthcare Professionals
The professionals reported that they had worked with PROM results in 2 to 15 patients who had completed the PROMs. On a scale from 1 “negative” to 5 “positive”, their experience with the use of PROMs was predominantly positive (range: 3.0–4.0; one expressed 3.0). They considerably valued the use of PROMs (range: 4.0–5.0; two expressed 5.0) and perceived additional value of PROMs both during the preparation for the patient appointment and during the appointment. The professionals' experiences with the PROMs are summarised in Table 4 .
Communication Between Patient and Healthcare Professional
All five patients answered that the care provider did not follow up on all the responses to the questionnaires during the appointment, and one patient had been asked by the care provider if the PROMs had been received well. Despite this, four of the five patients felt that attention was paid to the symptoms and/or issues they wanted to discuss.
Two of the three patients who did not complete PROMs felt that attention was paid to the symptoms and/or issues they wanted to discuss during the appointment.
Reasons to Not Complete PROMs
Of the patients who did not complete PROMs, one began filling out PROMs but paused during the questionnaires, and was unable to go back to continue with the remaining questions due to technical issues. For one patient, it was not clear how to answer the questionnaires. The third patient stated that she did not fill out PROMs because she did not feel the need to do so, as this was optional. Healthcare professionals noted that, in addition to patients who did not complete PROMs, some patients at the outpatient clinic had not received the invitations because they had not followed the complete care pathway, for instance when patients were referred from another hospital not directly after the VTE diagnosis.
NoMAD Questionnaire
Fig. 2 shows the responses to the NoMAD questionnaire, assessing the implementation process from the professionals' perspective. All four healthcare professionals strongly agreed with the potential value of the use of PROMs at the outpatient clinic and valued the effects that the use of PROMs had on their work. Also, they all stated to continue to support the use of PROMs, and all strongly believed that feedback about the use of PROMs can be used to improve its application in the future. They believed that key individuals play a crucial role in driving the use of PROMs and engaging others, and also considered participation in the use of PROMs as part of their own responsibilities (questions: 4–6, 8, and 18, 19).
Frequency distribution of responses to the NoMAD questionnaire assessing the implementation process from the healthcare professional's perspective. The bars show the percentages of healthcare professionals reporting “strongly disagree”, “disagree”, “neutral”, “agree”, or “strongly agree” to each of the questions. Constructs: questions 1 to 4: coherence, questions 5 to 8: cognitive participation, questions 9 to 15: collective action, and questions 16 to 20: reflexive monitoring. NoMAD: normalization measure development, PROMs: patient-reported outcome measures.
Healthcare professionals expressed positive views regarding the integration of the PROMs into their work and felt that they could adapt their approach to using PROMs (questions: 9 and 20).
There was unanimous disagreement with the statement that the use of PROMs disrupts working relationships (question: 10).
Not all agreed that sufficient resources are available to support the use of PROMs and one of the healthcare professionals felt unaware of reports about the effects of the use of PROMs (questions: 14 and 16).
Furthermore, some healthcare professionals took a neutral stance on whether the training provided is sufficient to enable staff to use PROMs, whether management adequately supports the use of PROMs, and whether there is a shared understanding among staff regarding the purpose of PROMs (questions: 2, 13, and 15).
Suggestions for Improvement
Patients and professionals were asked how the (use of) PROMs could be improved. Suggestions were shared to enhance the PROM completion rate and improve accessibility ( Table 5 ). Clarifying the purpose and relevance of PROMs in the e-mail with invitation link sent to patients, including the explanation that not all questions may be applicable to each individual, could enhance patient experiences and their willingness to complete the questionnaires. Also, the number of questions could be reduced. In addition, some patients indicated to have missed certain specific questions, for example, questions about the effectiveness of the medication and side effects, or about work, sports, and needs toward rehabilitation. Lastly, ensuring proper alignment of the outpatient appointments and measurement time points, and suggestions for improvement of technical aspects related to the digital PROMs application and to the dashboard facilitated by the digital tool were mentioned by professionals.
Discussion
This first evaluation after the implementation of routine use of PROMs for VTE patients visiting our outpatient clinic revealed that both patients and healthcare professionals when asked about their experiences, felt neutral to positive about the use of PROMs. Notably, PROMs were completed by less than half the patients who received the invitation. Professionals perceived additional value of PROMs both during preparation for the patient appointment and during the appointment. Patients who completed the PROMs, however, indicated that their responses to the questionnaires were not always addressed during the appointment, but despite this, felt that the symptoms and/or issues they wanted to discuss had been paid attention, while patients who did not complete PROMs also felt that they had been given proper attention. For some patients, the PROMs enhanced the preparedness for the outpatient clinic visit, while others did not feel prepared for the visit despite completing the questionnaires or felt prepared regardless of the PROMs. The majority of the patients felt that the PROMs contained too many questions.
Implementation of PROMs into routine care comes with challenges. Web-based data entry may support PROMs completion and processing, by enabling to automatically incorporate the data into the electronic health records or other digital platforms that are designed to capture patient data. 28 Electronic data processing could also facilitate the interpretation of the PROM responses through analysis and (visual) presentation of the results, which could facilitate the use of PROM results by care providers in clinical decision-making. The completion of PROMs by patients requires (digital) literacy and skills. Also, not all questionnaires are available in multiple languages. Both the available resources and local context could affect the implementation success. 23 Moreover, the engagement of involved staff and dedicated personnel to coordinate the implementation process is essential for the integration of PROMs into routine care. 29 In our study, the involved healthcare professionals all felt committed to continue providing support to the use of PROMs.
The results of this early evaluation are encouraging, affirming the potential of routine use of PROMs for VTE patients, while key lessons can be learned that will benefit further implementation and application of PROMs in routine care. First, resources to increase and optimize the use of PROMs could be made available, including the potential to generate overviews of the distribution of PROM invitations, as well as the technical resources to support data processing and interpretation of the PROM responses. Second, patients should be better informed about the purpose and relevance of the questionnaires. Third, training and education on the application and interpretation of PROMs and their effects could improve healthcare professionals' ability to use the PROMs and enhance patients' experiences. One example would be to share the instruction to always discuss PROM results with the patient and follow up on responses to the questionnaires during the appointment. Lastly, reduction of the question load could improve the completion and use of PROMs.
The feasibility of implementation of other ICHOM standard sets has been demonstrated in several studies. 29 30 31 32 33 34 35 In a study evaluating the implementation of the ICHOM standard set for stroke, PROMs were considered relevant by patients, although they were found to have a limited understanding of the purpose of PROM assessment. 36 This is in line with our findings based on patients' experiences. Reported facilitators for successful implementation include the direct value of PROMs on individual patient care, professional education and feedback, and efforts to motivate patients to complete PROMs. 37 38 All professionals participating in the current study believed that feedback about the use of PROMs can indeed further improve its successful and meaningful application. Studies in the field of nephrology provided insights into the application of PROMs and guidance for optimal discussion of PROM results. 39 40 Both patients and healthcare professionals highlighted the importance of always discussing PROM results, with active participation of patients and a guiding role of professionals. Key enablers included a trustful relationship between the patient and care provider, a safe and private setting during a face-to-face consultation, an announcement of the discussion about PROM results during the appointment, and focusing on the most important topics during the consultation to deal with time constraints. These findings can be used for training of healthcare professionals.
The study has some limitations. First, the number of participants is small. As this was an evaluation study at a single academic hospital, performed a few months after implementation of the PROMs as part of routine care, we included as many patients who encountered the PROMs during follow-up at the outpatient clinic as were available. Consequently, our findings may not be generalizable to other hospitals or settings. We described the insights based on the first experiences of patients and healthcare professionals, but could not draw definitive conclusions due to the small sample size. Second, the patients who had completed PROMs at both follow-up time points could not accurately recall the time they spent completing the questionnaires. However, as patients indicated that the number of questions was too large, we still gained insight into their experience with the time burden associated with the completion of the PROMs.
Future studies are needed to assess how insights gained from the questionnaires are used in daily care, as well as to determine appropriate follow-up actions and evaluation in relation to specific PROM results, and their impact on outcomes such as quality of life.
Conclusion
We gained insights based on the first experiences of patients and healthcare professionals with the use of PROMs in routine outpatient thrombosis care. PROMs were considered valuable by the healthcare professionals, and are believed to provide additional value during preparation for the visit to the outpatient clinic as well as during the visit. Patients, however, expressed that the PROMs contained too many questions and that their responses were not always addressed during the visit, but despite this, felt that they had been given proper attention. Some patients felt better prepared for the visit due to the completion of the PROMs, while others did not. The experiences and suggestions for improvement can be used to improve the application of PROMs in clinical practice and support further implementation of PROMs in daily thrombosis care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1American Heart Association Council on Peripheral Vascular Disease, Council on Clinical Cardiology, and Council on Cardiovascular and Stroke Nursing Kahn S R Comerota A J Cushman M The postthrombotic syndrome: evidence-based prevention, diagnosis, and treatment strategies: a scientific statement from the American Heart Association Circulation 2014130181636166125246013 10.1161/CIR.0000000000000130 · doi ↗ · pubmed ↗
- 2Wolberg A S Rosendaal F R Weitz J I Venous thrombosis Nat Rev Dis Primers 201511500627189130 10.1038/nrdp.2015.6 · doi ↗ · pubmed ↗
- 3Huisman M V Barco S Cannegieter S C Pulmonary embolism Nat Rev Dis Primers 201841802829770793 10.1038/nrdp.2018.28 · doi ↗ · pubmed ↗
- 4Klok F A Mos I C Broek L Risk of arterial cardiovascular events in patients after pulmonary embolism Blood 2009114081484148819549987 10.1182/blood-2009-05-220491 · doi ↗ · pubmed ↗
- 5Klok F A Zondag Wvan Kralingen K W Patient outcomes after acute pulmonary embolism. A pooled survival analysis of different adverse events Am J Respir Crit Care Med 20101810550150619965808 10.1164/rccm.200907-1141 OC · doi ↗ · pubmed ↗
- 6Klok F Avan der Hulle Tden Exter P L Lankeit M Huisman M V Konstantinides S The post-PE syndrome: a new concept for chronic complications of pulmonary embolism Blood Rev 2014280622122625168205 10.1016/j.blre.2014.07.003 · doi ↗ · pubmed ↗
- 7Barco S Mahmoudpour S H Valerio L Trends in mortality related to pulmonary embolism in the European Region, 2000-15: analysis of vital registration data from the WHO mortality database Lancet Respir Med 202080327728731615719 10.1016/S 2213-2600(19)30354-6 · doi ↗ · pubmed ↗
- 8FOCUS Investigators Valerio L Mavromanoli A C Barco S Chronic thromboembolic pulmonary hypertension and impairment after pulmonary embolism: the FOCUS study Eur Heart J 202243363387339835484821 10.1093/eurheartj/ehac 206PMC 9492241 · doi ↗ · pubmed ↗