When Vomiting Isn’t Just a Bug: Unmasking Two Rare Causes of Pediatric Dysphagia
Noora AlSuwaidi, Bachir Farzat, Imad Hannoun

TL;DR
This paper discusses two rare cases of esophageal obstruction in children, emphasizing the need for thorough diagnosis beyond common causes.
Contribution
The paper contributes by highlighting two uncommon pediatric conditions causing dysphagia and vomiting through case reports.
Findings
A 10-year-old boy with Angelman syndrome was found to have a double aortic arch causing esophageal compression.
A 13-year-old child with chronic vomiting was diagnosed with primary achalasia.
The cases underscore the importance of considering structural disorders in pediatric dysphagia.
Abstract
Pediatric vomiting and feeding difficulties are common presentations in both emergency and outpatient settings. Although these symptoms are often attributed to benign causes such as infections or gastroenteritis, structural and functional esophageal disorders must also be considered. This report describes two diagnostically challenging cases of esophageal obstruction in children. The first involves a 10-year-old boy with Angelman syndrome, ultimately diagnosed with a double aortic arch causing extrinsic esophageal compression. The second case features a previously healthy 13-year-old with chronic vomiting, later identified as having primary achalasia. These cases highlight the importance of maintaining a broad differential diagnosis and employing targeted imaging to prevent delays in diagnosis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
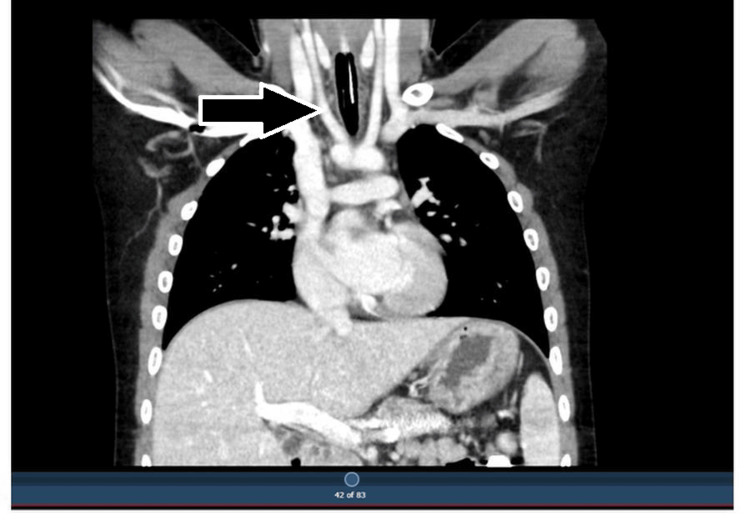 Figure 1
Figure 1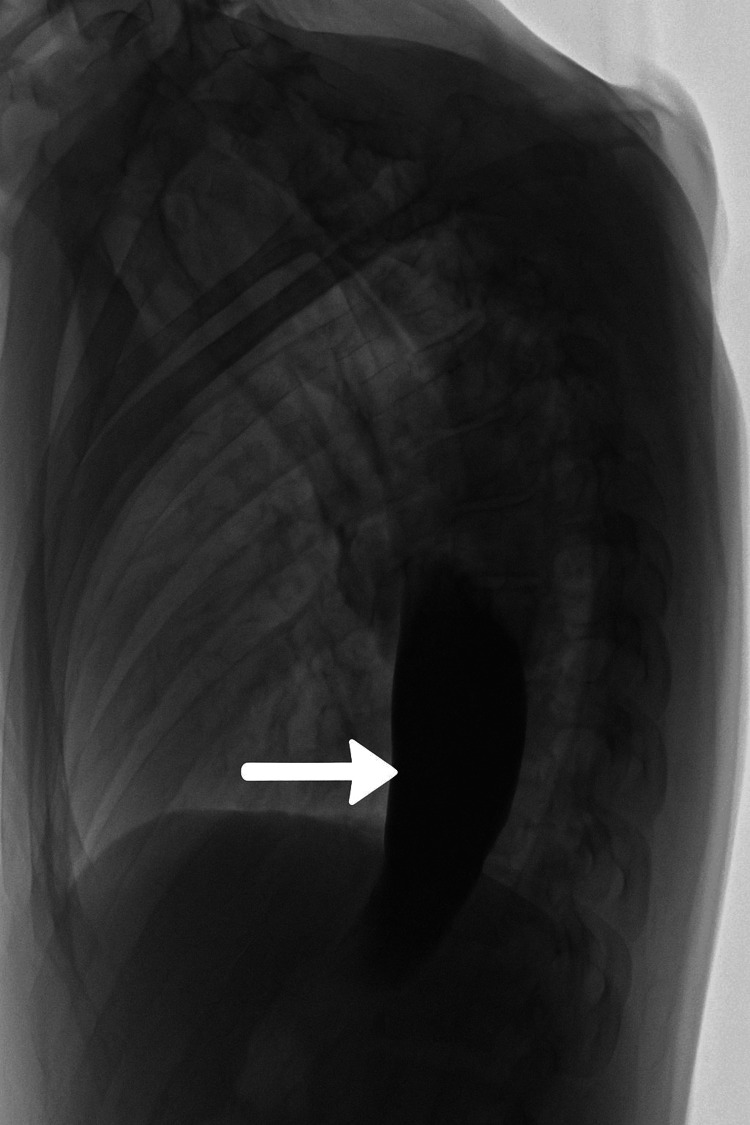 Figure 2
Figure 2| Test | Result | Reference range |
| WBC | 6.9 | 4.5-13.5 × 10⁹/L |
| Hemoglobin | 13.9 | 11.5-15.5 g/dL |
| Platelets | 229 | 150-400 × 10⁹/L |
| Lipase | 21 | 0-60 U/L |
| Amylase | 31 | 28-100 U/L |
| Sodium | 139 | 135-145 mmol/L |
| Potassium | 4 | 3.5-5.0 mmol/L |
| Bicarbonate | 19 | 20-28 mmol/L |
| Creatinine | 0.58 | 0.5-1.0 mg/dL |
| Urea | 29 | 2.5-7.5 mmol/L |
| Liver function tests | Normal | Normal |
| Test | Result | Reference range |
| WBC | 7.9 | 4.5-13.5 × 10⁹/L |
| Hemoglobin | 12.4 | 11.5-15.5 g/dL |
| Platelets | 272 | 150-400 × 10⁹/L |
| Sodium | 136 | 135-145 mmol/L |
| Potassium | 4.2 | 3.5-5.0 mmol/L |
| Bicarbonate | 19 | 20-28 mmol/L |
| Urea | 21 | 2.5-7.5 mmol/L |
| Glucose | 89 | 70-110 mg/dL |
| Liver function tests | Normal | Normal |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastroesophageal reflux and treatments · Dysphagia Assessment and Management · Esophageal and GI Pathology
Introduction
Vomiting and feeding difficulties are among the most common presenting complaints in pediatric practice. While these symptoms are often attributed to benign, self-limiting conditions such as viral gastroenteritis, clinicians must remain alert to more insidious and diagnostically challenging causes. Structural anomalies like vascular rings [1-3] and functional disorders such as achalasia [4-7] can closely mimic more common gastrointestinal conditions, frequently leading to significant diagnostic delays.
Pediatric achalasia is an uncommon motility disorder that often presents with subtle, nonspecific symptoms that are easily mistaken for more prevalent conditions like gastroesophageal reflux. Similarly, vascular rings, including double aortic arch or aberrant subclavian artery, may present with chronic vomiting, feeding intolerance, or recurrent respiratory symptoms, and are typically diagnosed only after a careful and systematic evaluation.
In this manuscript, we present two illustrative cases that highlight the diagnostic complexity associated with esophageal achalasia and vascular ring anomalies in children. Although these conditions are well documented in the literature, the cases emphasize the importance of maintaining a broad differential diagnosis when evaluating persistent vomiting and feeding issues. Through these reports, we aim to share practical clinical insights and raise awareness of these uncommon yet clinically significant conditions to support timely and accurate diagnosis in similar presentations.
Case presentation
Case 1
In March 2025, a 10-year-old boy with a known diagnosis of Angelman syndrome was evaluated at the Pediatric Emergency Department of Al Jalila Children’s Specialty Hospital in Dubai, United Arab Emirates. He presented with a three-day history of progressively noisy breathing, accompanied by a two-day history of vomiting solids, while still tolerating liquids. Given the acute onset and his underlying neurodevelopmental condition, the initial differential diagnosis prioritized foreign body ingestion.
Clinical examination, including respiratory and abdominal assessments, was unremarkable. Baseline laboratory investigations were within normal limits (Table 1). A lateral neck radiograph revealed a soft tissue shadow in the prevertebral space at the level of C6-C7. Based on these findings, a barium swallow study was performed, which demonstrated an extrinsic posterior indentation of the esophagus. CT angiography subsequently confirmed the presence of a double aortic arch compressing the posterior esophageal wall (Figure 1) [3], establishing the diagnosis of a vascular ring anomaly.
Coronal CT angiography showing a double aortic arch encircling the trachea and esophagus, leading to posterior esophageal compression
Case 2
Another case seen in March 2025 involved a 13-year-old previously healthy male who was referred to the Pediatric Emergency Department at Al Jalila Children’s Specialty Hospital in Dubai, United Arab Emirates, with a one-month history of persistent, non-bilious vomiting. He had undergone multiple outpatient evaluations, none of which yielded a definitive diagnosis. On arrival, his vital signs were stable, and physical examination was unremarkable. Laboratory investigations, including a metabolic panel and inflammatory markers, were within normal limits (Table 2).
Plain abdominal radiography revealed a dilated esophagus, raising suspicion for an underlying motility disorder. A barium swallow study showed a characteristic smooth tapering at the gastroesophageal junction, with delayed contrast transit that improved with the administration of water. These radiological findings were consistent with primary achalasia (Figure 2) [4-7].
Lateral view from a barium swallow showing smooth tapering at the gastroesophageal junction, consistent with the “bird’s beak” sign of achalasia
Discussion
Both double aortic arch and achalasia are rare but significant causes of esophageal obstruction in children [1-7]. Although they stem from fundamentally different pathologies - one congenital and structural, the other functional and neuromuscular - their overlapping symptoms can complicate the diagnosis.
Double aortic arch is the most common type of complete vascular ring, accounting for approximately 42% of all symptomatic vascular rings in children [1,2]. It results from the persistence of both fourth aortic arches during fetal development, forming a ring that compresses the trachea and esophagus. The incidence of symptomatic vascular rings is estimated to range from 1 in 10,000 to 1 in 50,000 live births. These anomalies often present in infancy or early childhood with feeding difficulties, stridor, or recurrent respiratory infections. CT angiography has become the preferred imaging modality for diagnosis due to its ability to clearly delineate vascular anatomy [3].
In contrast, achalasia is a primary motility disorder characterized by failure of the lower esophageal sphincter to relax and the absence of esophageal peristalsis. It is extremely rare in pediatrics, with an estimated incidence of 0.1 to 0.18 per 100,000 children per year [5]. Pediatric patients typically present with vomiting, weight loss, and dysphagia. A barium swallow classically shows a “bird’s beak” appearance of the distal esophagus, while esophageal manometry is the gold standard for diagnosis [4,6,7]. However, access to pediatric manometry may be limited in many centers.
These two cases highlight the importance of maintaining a broad differential diagnosis in children presenting with persistent vomiting or dysphagia, especially in those with neurodevelopmental disorders, where communication challenges can obscure classic symptoms. A high index of suspicion, coupled with early use of targeted imaging like barium swallow studies and CT angiography, can significantly aid in identifying esophageal abnormalities. Barium swallow remains a valuable diagnostic tool, particularly when endoscopy or manometry are not readily available. Additionally, incorporating cross-sectional imaging early in the diagnostic workup is crucial when symptoms persist despite an unremarkable initial evaluation. A systematic and vigilant approach to assessment allows for timely diagnosis and intervention, ultimately improving clinical outcomes and reducing the risk of long-term morbidity.
Conclusions
Persistent vomiting and dysphagia in children should prompt consideration of rare structural and functional esophageal disorders, such as vascular rings and achalasia, particularly when standard evaluations yield inconclusive results. Early use of targeted imaging and maintaining a high index of suspicion are critical to ensuring timely diagnosis and effective management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Trends in vascular ring surgery J Thorac Cardiovasc Surg Backer CL Mavroudis C Rigsby CK Holinger LD 1339134712920051594257510.1016/j.jtcvs.2004.10.044 · doi ↗ · pubmed ↗
- 2Decade of experience with vascular rings at a single institution Pediatrics Humphrey C Duncan K Fletcher S 08117200610.1542/peds.2005-167416585275 · doi ↗ · pubmed ↗
- 3Computed tomography in the evaluation of vascular rings and slings Insights Imaging Etesami M Ashwath R Kanne J Gilkeson RC Rajiah P 507521520142500843010.1007/s 13244-014-0343-3PMC 4141344 · doi ↗ · pubmed ↗
- 4ACG clinical guideline: diagnosis and management of achalasia Am J Gastroenterol Vaezi MF Pandolfino JE Vela MF 1238124910820132387735110.1038/ajg.2013.196 · doi ↗ · pubmed ↗
- 5Variation in esophageal anastomosis technique—the role of collaborative learning Dis Esophagus Halliday LJ Doran SL Sgromo B 33202010.1093/dote/doz 07231665408 · doi ↗ · pubmed ↗
- 6Achalasia in children—clinical presentation, diagnosis, long-term treatment outcomes, and quality of life J Clin Med Jarzębicka D Czubkowski P Sieczkowska-Gołub J KierkuśJ Kowalski A Stefanowicz M Oracz G 10202110.3390/jcm 10173917 PMC 843217534501361 · doi ↗ · pubmed ↗
- 7Clinical features of achalasia in children J Pediatr Gastroenterol Nutr Sodikoff JB Loening-Baucke V Raasch RH Colombo JM 487492492009