Epidemiology and Treatment of Olecranon Fractures: a nationwide register-based analysis of 27,880 cases in Denmark from 1999 to 2018
Walid Zeyghami, Dennis Karimi, William M. Hagemann, Per H. Gundtoft, Bjarke Viberg, Tazio Maleitzke

TL;DR
This study analyzed 27,880 olecranon fracture cases in Denmark from 1999 to 2018, finding increasing incidence rates and shifts in treatment preferences over time.
Contribution
The study provides a nationwide, long-term epidemiological analysis of olecranon fractures and treatment trends in Denmark.
Findings
The incidence of olecranon fractures increased by 29% from 1999 to 2018.
Non-surgical treatment was predominant, but surgical treatment increased in older patients.
Plate fixation became more popular while tension-band wiring decreased over time.
Abstract
Olecranon fractures (OFs) account for approximately 20% of proximal forearm fractures. Displaced or unstable OFs are typically treated surgically with tension-band wiring (TBW) or plate fixation (PF). While comparative works on surgical OF management exist, epidemiological studies are limited by short time spans and small sample sizes. This study investigates OF incidence rates (IRs), and treatment trends in Denmark over a 20-year period from 1999 to 2018. Population-based Danish National Patient Register study on OFs in adult patients from 1999 to 2018. Patients ≥ 20 years diagnosed with OF (ICD-10: S520) were included. Age, sex, and treatment were recorded. Treatment was classified as surgical if relevant surgical procedure codes were recorded within 21 days of OF diagnosis. In the absence of such codes, treatment was classified as non-surgical. A total of 27,880 OF cases (61%…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1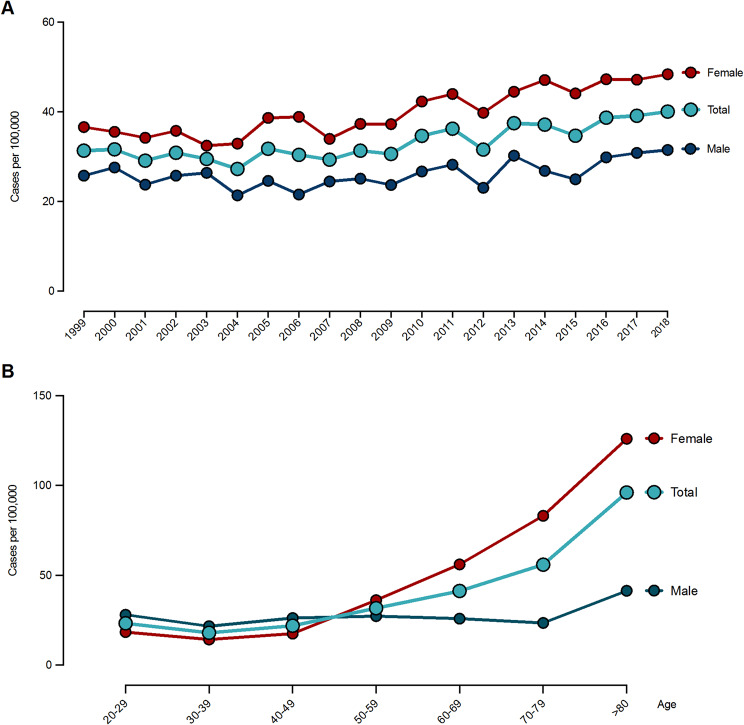 Figure 2
Figure 2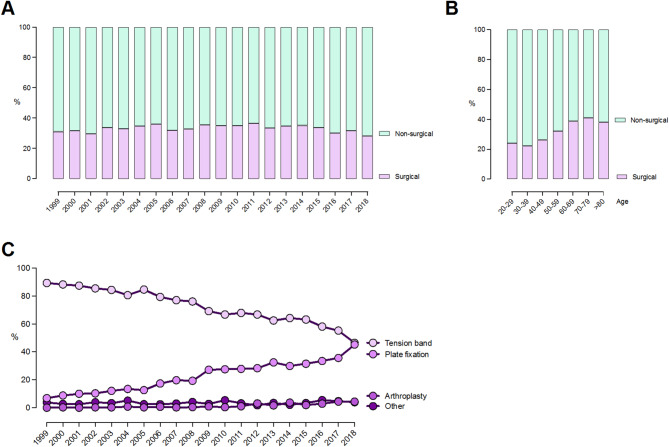 Figure 3
Figure 3- —Charité - Universitätsmedizin Berlin (3093)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsElbow and Forearm Trauma Treatment · Orthopedic Surgery and Rehabilitation · Bartonella species infections research
Background
Olecranon fractures (OFs) account for approximately 20% of all proximal forearm fractures [1, 2]. Displaced and unstable OFs are typically treated surgically with tension-band wiring (TBW) or plate fixation (PF) [3–6], while undisplaced OFs may be treated non-surgically with cast immobilization of the elbow [7, 8].
Although OF management is widely studied [6, 7, 9, 10], only two studies examine the epidemiology of OFs [1, 11]. Both studies are limited by their short time spans, ranging from one to four years, and only one study reports incidence rates [1]. To date, no large-scale, long-term population-based studies have described the incidence or treatment patterns of OFs. Despite the relatively high prevalence of OFs, there is limited high-quality evidence defining optimal treatment strategies. As a result, a variety of treatment approaches are currently used in clinical practice. Large-scale register works are important to study incidences of representative populations as well as current and past treatment practices and how these are distributed across different age groups.
Over time, treatment approaches for OFs have shifted in response to evolving surgical techniques and a better understanding of patient-specific needs. While TBW has historically been the most common surgical method, PF has gained popularity due to enhanced stability and lower risk of hardware-related complications [10, 12–15]. Furthermore, management strategies now increasingly reflect patient age and activity level, with non-surgical approaches considered for elderly patients with low functional demands [6, 16]. These trends emphasize the importance of analyzing long-term treatment patterns to optimize care for diverse patient groups.
This study aimed to evaluate incidence rates (IRs), and treatment trends of OFs in Denmark over two decades, from 1999 to 2018.
Methods
Study design
This is a population-based register study on OFs in adult patients from the Danish National Patient Register (DNPR) between 1999 and 2018. Study results are reported according to the RECORD guidelines [17].
Setting
The study was conducted in Denmark, where all permanent residents are assigned a unique, 10-digit identification number. This enables linkage of patients on an individual level across all Danish medical databases [18]. The Danish National Health Service provides free access to healthcare including access to general practitioners and general hospital care with emergency service for all permanent residents [19]. Private emergency treatment are not available in Denmark, therefore nearly all fracture treatment is conducted at public hospitals.
Data source
Patient data were extracted from the DNPR covering a period from 1999 to 2018. The DNPR was established in 1977, and is a comprehensive administrative database covering 98.8% of all hospital contacts in Denmark [20]. It is mandatory to report administrative data such as age, sex, diagnosis and procedure codes monthly for all public and private hospitals. Since 1995 diagnosis codes are registered using the International Statistical Classification of Diseases version 10 (ICD-10) and surgical procedure codes according to The Nordic Medico-Statistical Committee (NOMESCO) system [21].
Participants
The study population included patients ≥ 20 years with an OF diagnosis (ICD-10: S520). The accuracy of the OF diagnosis code in the DNPR has not yet been validated, however Schmidt, et al. reported a positive predictive value of 83% for all orthopedic diagnosis codes registered in the DNPR [20]. The diagnosis codes for humerus fractures, hip fractures and ankle fractures have been independently validated and demonstrated positive predictive values ranging from 78 to 92% [22–24]. Foreign patients without a permanent residence in Denmark have no records of their sex in the DNPR and were thus excluded from the study population.
Variables
Data on age, sex, diagnosis code, date of diagnosis, procedure code and date of procedure were extracted. Treatments were classified as surgical if relevant surgical procedure codes were recorded within 21 days of the initial OF diagnosis. This time frame was chosen to (i) cover patients receiving surgery primarily, and (ii) those treated conservatively, who were converted to surgery following secondary fracture displacement. In Denmark, patients that are primarily treated conservatively, are usually seen for a 1-week-follow-up where they are screened for secondary displacement and planned for subsequent surgery if required.
In the absence of surgical procedure codes, treatment was classified as non-surgical. The surgical procedure codes were divided into four categories: TBW (KNCJ40), plate fixation (KNCJ60), arthroplasty (KNCB0, KNCB1, KNCB2, KNCB3 and KNCB4), and other procedures (nailing [KNCJ50], external fixation [KNCJ20], combined method [KNCJ80] and unspecified method [KNCJ90]).
Statistics
Descriptive statistics were used to report age, sex, number of OFs and treatment. We report incidences as cases per 100,000 persons a year, where the population data for each year were obtained from Statistics Denmark [25]. Incidences were reported by age in 10-year intervals: 20–29, 30–39, 40–49, 50–59, 60–69, 70–79, 80–89 and ≥ 90 years. In addition, treatment is reported for patients between 20 and 70 and > 70 years.
Ethics
DNPR data are based on diagnosis and procedure codes, with all information being anonymized to ensure patient identities remain confidential. According to Danish Law ethical approval is not applicable (Table 1).
Table 1. Demographics of olecranon fracture (OF) patients from 1999 to 2018 in DenmarkTotal19992000200120022003200420052006200720082009201020112012201320142015201620172018N2788012711287118612601204111412991246120512941273144915251337159915971506170017361792Fracture incidence per 10^5^33.131.331.629.130.929.527.331.830.429.331.330.634.636.231.637.537.134.738.739.140.1SexFemale171167607397137466776878078147137867909029438589661030973105410611097Male10764511548473514527427492432492508483547582479633567533646675695Age20–29318818020117315416211511711613514014615914515815616118420017421230–392710168174138164152139147125114116991481621211279612711512715140–49343815915414816315113418516816115816118117619120723117017518617950–59470622420417722120317420220519821620727827522326326323129632532160–69503016315418115117319119521520023524426231724134333331737336637670–79443819218417720617616921018219119719519621718824228426130233433580–893398146172145164151158197189165169189176166168203159163185165168≥ 909723944473736344646416332496747587053545950Median6055.855.657.656.756.862.46060.459.863.16158.560.859.861.464.461.361.761.761.5
Results
We included 28,351 patients with an OF diagnosis code from 1999 to 2018. A total of 471 foreign patients were excluded, which resulted in a total of 27,880 patients (Fig. 1).
Fig. 1. Study population of olecranon fractures based on the Danish National Patient Register (DNPR)
Epidemiology
The mean age was 61 years and 61% of patients were female. The incidence of OFs increased by 29% over the study period from 31/100,000/year in 1999 to 40/100,000/year in 2018. The overall mean incidence was 33/100,000/year (Fig. 2A). Males aged 20–49 had higher IRs than females in the same age group. This changed to predominately females in the ≥ 50 years group (Fig. 2B). Overall, the highest IR was observed among patients ≥ 80. While this was true for males and females, females still had higher IRs than males in this age group (Fig. 2B). The overall and sex-stratified age-specific IR gradually increased with advancing age in females but remained stable in males (Fig. 2B).
Fig. 2. Incidence rates of olecranon fractures from 1999 to 2018 in Demark. Distribution stratified by sex over time (A), and according to age groups (B)
Treatment
Overall, 67% of cases were treated non-surgically (range: 64% in 2005 to 72% in 2018, Fig. 3A). This remained stable throughout the study period. Additionally, females were more likely to undergo surgical treatment than males throughout the entire study period with 36% of females undergoing surgery (range: 30–42%) compared to 28% of males (range: 25–34%). Surgical treatment was more frequent in patients ≥ 50 years (37%, range: 32–41%) than in patients < 50 years (24%, range: 22–26) (Fig. 3B).
The distribution of surgical and non-surgical treatment remained stable throughout the study period for patients aged 20–69 years, with 25–33% treated surgically and 67–75% treated non-surgically. In patients aged ≥ 70 years, surgical treatment decreased, and non-surgical treatment increased from 2013 onwards (Fig. 3A, B).
Fig. 3. Treatment of olecranon fractures from 1999 to 2018 in Demark. Distribution stratified by surgical or non-surgical treatment over time (A), and according to age groups (B). Distribution of different surgical treatments over time (C)
The choice of surgical implants changed considerably over time, with the use of TBW continuously decreasing and the use of PF significantly increasing from 1999 to 2018. In 1999, TBW was utilized in 89% of surgically treated patients, whereas PF was used in only 7% of cases. By 2018, the use of PF had increased to 45%, matching TBW, which was used in 46% of cases. The use of other surgical techniques remained stable throughout the period (Fig. 3C).
Discussion
In this study, we assessed the epidemiology and treatment of OFs over a 20-year period in Denmark. The IR increased over time from 31 in 1999 to 40 in 2018. While IRs generally increased with age, this was especially relevant in females ≥ 50 years. Most patients were treated non-surgically (67%). Interestingly, surgical treatment became more frequent in patients ≥ 50 years. While most surgically treated patients underwent TBW in 1999, we found an even distribution of TBW and PF in 2018.
Reported IRs of OFs vary widely in the literature, mostly due to differences in study design and fracture classification. Duckworth, et al. reported a much lower IR (12/100,000/year) [1], and Axenhus, et al. a much higher IR (333/100,000/year) [26]. This is likely due to alternating inclusion criteria, time periods and demographic populations. Despite these differences, both studies, like ours, observed a similar increase in IRs among patients with increasing age > 50 years, highlighting rising fracture rates with age.
We found that in the Danish population 67% of patients were treated non-surgically, which remained stable through the study period. With increasing age, people were more likely to be treated surgically. In the 20–29 years group, 24% were treated surgically, while in the 70–79 years group, 41% were operated. While this suggests an increased likelihood of surgical treatment with age, it is important to note that the majority (59%) of elderly patients were still treated non-surgically. A reason for this may be more complex fracture patterns, resulting from osteoporosis and less controlled falls due to higher frailty scores in the elderly [27, 28]. A similar trend was seen in a Swedish observational study [11]. However, since we have no data on fracture patterns, it is difficult to directly compare our findings with the study by Brüggemann et al. [11].
The choice between surgical and non-surgical treatment for displaced OFs remains a topic of debate, particularly in elderly patients [9, 16, 29]. Retrospective cohort data indicate that non-surgical treatment in patients ≥ 70 with displaced OFs provides satisfactory functional range of motion and a high level of patient satisfaction [29]. A randomized controlled trial showed that patients over 75 years who underwent surgery with either TBW or PF experienced a high complication rate of 81.8% compared to 14.3% in those receiving conservative treatment, which led to the trial being prematurely terminated [16].
As a reaction to those results, new guidelines which favor a more conservative approach for OF patients ≥ 75 years were introduced in Denmark in 2018 [30]. We observed a noticeable shift toward more non-surgical treatment in elderly patients from 2013 onwards, potentially driven by study results showing that non-surgical treatment is a viable alternative in elderly patient cohorts [1, 2, 16, 29, 31].
In 1999, TBW was the preferred surgical method to treat OFs. However, a gradual shift toward an increased use of PF was observed from 2002 onwards, with both methods showing parity in 2018. The introduction of locking plates around 2000 may have contributed to this trend [32], which is likely to have continued beyond 2018.
Additionally, multiple studies have highlighted the advantages of PF over TBW, including a lower risk of implant irritation, reduced rates of implant removal, superior biomechanical properties, and enhanced interfragmentary compression [10, 12, 15, 33–35]. Despite these benefits, no significant differences in functional outcomes, such as range of motion or Disabilities of the Arm, Shoulder, and Hand (DASH) score, have been observed comparing the two techniques [15, 33, 34].
In recent years, tension band suture repair has been introduced as an alternative fixation method for certain stable OF types [4, 9, 36]. However, potential advantages of tension band suture repair are still under investigation [36–38] with two multicenter randomized controlled trials currently underway [39, 40].
One of the strengths of this study is the use of the DNPR, which provides nationwide data. In Denmark, public and private hospitals are legally mandated to report data to the DNPR, ensuring comprehensive and reliable data collection [18–20]. Therefore, missing data likely only include patients who did not seek emergency treatment for OFs. We believe this represents a very small group, as healthcare is free in Denmark [19].
A limitation of this study is the lack of validation for the OF diagnosis and surgical procedure codes in the DNPR. However, the overall validation of orthopedic diagnoses and procedures in the DNPR is known to be high [20, 22, 41], and we have no reason to believe that the reporting practices to the register changed during the study period. Moreover, the use of register-based data introduces the risk for misclassification bias, as coding errors or variations in reporting may affect the accuracy of fracture diagnoses and treatment classifications. Additional limitations include the lack of information on patients’ comorbidities, such as osteoporosis and trauma mechanism. Furthermore, we were unable to provide specific details about fracture patterns and severity, which limits the interpretation of treatment decisions, as fracture severity is usually required to determine surgical or non-surgical management.
Conclusions
The incidence of OFs increased by 29% from 1999 to 2018, with an exponential increase in females ≥ 50 years, likely due to osteoporosis. Non-surgical treatment was predominant across all ages, yet older patients were more likely to be operated than younger patients. The use of PF steadily increased during the study period showing equal numbers for PF and TBW in 2018.
Future research may identify which patients benefit most from surgical or non-surgical treatment by incorporating patient-specific factors such as age, activity level, and comorbidities, thereby refining decision-making and optimizing outcomes that matter to patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Duckworth AD, Carter TH, Chen MJ, Gardner MJ, Watts AC. Olecranon fractures: current treatment concepts. The bone & joint journal. 2023;105-b(2):112– 23.10.1302/0301-620X.105B 2.BJJ-2022-0703.R 136722062 · doi ↗ · pubmed ↗
- 2Hamoodi Z, Duckworth AD, Watts AC. Olecranon fractures: A critical analysis review. JBJS Reviews. 2023;11(1).10.2106/JBJS.RVW.22.0015036638218 · doi ↗ · pubmed ↗
- 3Sørensen ST, Kristensen FP, Troelsen FS, Schmidt M, Sørensen HT. Health registries as research tools: a review of methodological key issues. Dan Med J. 2023;70(4).36999820 · pubmed ↗
- 4Karimi D, Houkjær L, Gundtoft P, Brorson S, Viberg B. Positive predictive value of humeral fractures in the Danish National patient registry. Dan Med J. 2023;70(4).36999816 · pubmed ↗
- 5Gundtoft PH, Danielsson FB, Houlind M, Mortensen SO, Corap Y et al. The positive predictive value of ankle fracture diagnosis in the Danish National patient registry. Dan Med J. 2022;69(12).36458605 · pubmed ↗
- 6Denmark S. 2024 [cited 2024 7. Nov]. Available from: https://www.dst.dk/en
- 7Migliorini F, Giorgino R, Hildebrand F, Spiezia F, Peretti GM et al. Fragility fractures: risk factors and management in the elderly. Med (Kaunas). 2021;57(10).10.3390/medicina 57101119 PMC 853845934684156 · doi ↗ · pubmed ↗
- 8Society DOS. Treatment of Displaced Stable Olecranon Fractures (Mayo Type II A + B) in Elderly Patients with Low Functional Capacity 2018 [Available from: https://www.ortopaedi.dk/wp-content/uploads/2018/09/Olecranon_ver 2.pdf