Lingual hamartoma‐like lipoblastoma: the diagnostic value of routine whole‐genome sequencing
Sheng‐Yuan Kan, Ashley Ferro, James A Watkins, Sam Behjati, Matthew J Murray, Nicholas Coleman, Thomas Roberts, Justin Cross, Jamie Trotman, Patrick Tarpey, C Elizabeth Hook, Malcolm Cameron, John A. Tadross

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
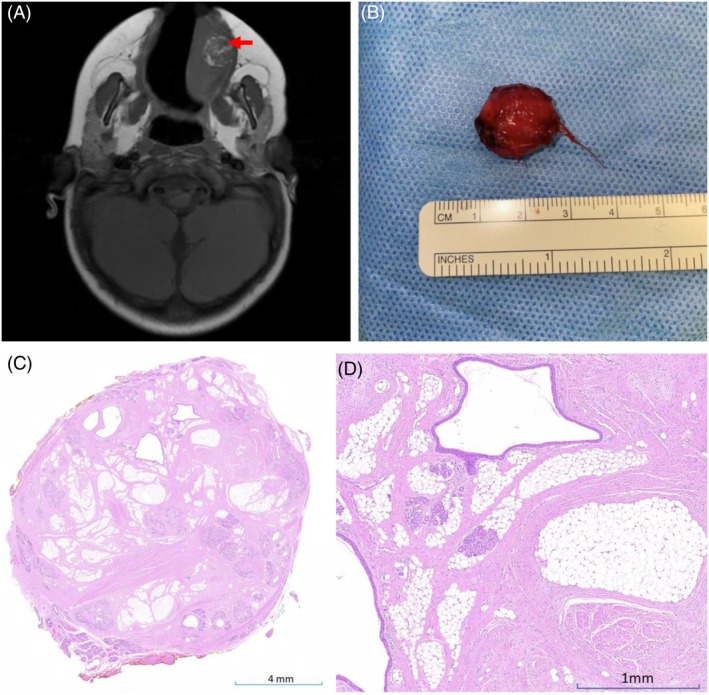 Figure 1
Figure 1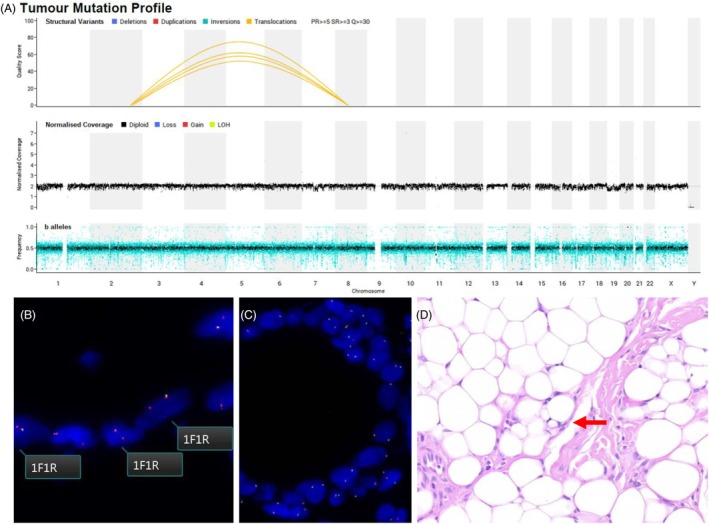 Figure 2
Figure 2- —Medical Research Council 10.13039/501100000265
- —Wellcome Trust 10.13039/100010269
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTumors and Oncological Cases · Histiocytic Disorders and Treatments · Sarcoma Diagnosis and Treatment
Paediatric tongue lesions are rare, and diagnostically challenging as a result.1 Histopathology often suffices for diagnosis, but some lesions require molecular assessment for precise characterization. All patients under 25 years of age with a differential that includes neoplasia are eligible for whole‐genome sequencing (WGS) on the NHS, and widespread adoption has the potential to disrupt routine pathology practice by providing comprehensive genomic characterization within days.2, 3, 4 Here we describe a 2‐year‐old with a tongue lesion that highlights the diagnostic value of routine WGS.
Case report
A 2‐year‐old girl presented with a 2‐week history of left tongue swelling, irritability, and drooling. She was otherwise healthy, with no feeding or respiratory issues. Examination revealed a 2‐cm diameter submucosal swelling. Magnetic resonance imaging (MRI) confirmed a 1.5‐cm diameter well‐defined lesion with nodular high‐intensity areas on T1 and moderate gadolinium enhancement, suggestive of a lipoma or hamartoma, with liposarcoma as a differential (Figure 1A). The lesion was surgically excised, appearing as an encapsulated nodule (Figure 1B). Histological examination revealed a mixture of fibrous and adipose tissues, atrophic skeletal muscle, and disorganized salivary glandular elements (Figure 1C,D). The initial diagnosis, based on the consensus of one paediatric and two head and neck pathologists, was of a benign lingual hamartoma.
(A) Baseline imaging with T1‐weighted axial MRI precontrast showing the lesion (red arrow). (B) Macroscopic image of the resected tumour. (C,D) Haematoxylin and eosin (H&E)‐stained sections demonstrating fibroconnective tissue and adipose tissue centrally, admixed distorted skeletal muscle, lobules of salivary glands, and ectatic ducts. [Color figure can be viewed at wileyonlinelibrary.com]
Fresh tissue from the lesion was submitted for WGS, which is routine practice in our hospital for all potential neoplasia in consenting patients under 25 years of age. Unexpectedly, WGS identified an in‐frame COL3A1::PLAG1 fusion (Figure 2A), which was subsequently confirmed by RNA fusion testing. This fusion is recurrent in lipoblastoma,5 and PLAG1 is also the most frequent fusion partner in pleomorphic adenoma (PA), a common salivary gland neoplasm that can exhibit both epithelial and mesenchymal differentiation. It is conceivable that a PA could present with lingual hamartoma‐like features, and data on the molecular landscape of lingual hamartomas is limited. We reasoned that were this an unusual PA rather than lipoblastoma, the epithelial and mesenchymal components would harbour the PLAG1 translocation. Fluorescence in situ hybridisation (FISH) analysis demonstrated that the rearrangement was restricted to adipocytes (Figure 2B,C), and the epithelial cells were nonneoplastic. Upon reexamination of the histology, subtle lipoblasts were noted interspersed among predominantly mature adipocytes (Figure 2D).
(A) Whole‐genome sequencing showing a quiescent genome with a single t(2;8) COL3A1::PLAG1 driver event. (B) FISH showing adipocytes with predominantly one fused (F) and one red probe (R) signal, indicating monoallelic loss of the 5′ region of the hybridized PLAG1 locus. (C) The epithelial component shows two fused signals with no evidence of PLAG1 break apart. (D) Sparse lipoblasts are seen on review. [Color figure can be viewed at wileyonlinelibrary.com]
The patient recovered well postsurgery and, given the diagnosis, remains under close surveillance due to the risk of recurrence.3
Discussion
Paediatric oral lesions often present nonspecific clinical and imaging features, complicating the differential diagnosis.1 In this case, the absence of immature lipoblasts and myxoid areas initially led to the exclusion of a lipoblastoma diagnosis.6 WGS, however, detected a pathognomonic COL3A1::PLAG1 fusion, underscoring its diagnostic utility in ambiguous cases. Lipoblastomas, unlike hamartomas, carry a risk of local recurrence and therefore necessitate closer postoperative surveillance.7
Routine WGS, as integrated into clinical practice by NHS England through initiatives such as the 100,000 Genomes Project, offers a powerful tool for comprehensive genomic assessment, substantially enhancing diagnostic accuracy, and informing treatment strategies. The rapid turnaround of WGS data will make it contemporaneously available with histological findings, allowing for seamless integration into diagnostic reports.1, 2 This has profound implications for histopathology, providing orthogonal diagnostic feedback, highlighting discrepancies (as in this case), and ultimately leading to better patient outcomes.
Author contributions
S.‐Y.K., A.F., and J.A.T. wrote the article and prepared the figures. J.A.W., S.B., M.J.M., T.R., P.T., J.T., C.E.H., and J.A.T., interpreted the whole‐genome sequencing data. All authors contributed to the conceptualisation, authorship, and review of the article.
Funding information
S.B. acknowledges funding from the Wellcome Trust (institutional grant; personal fellowships; grant number 108413/A/15/D and 223135/Z/21/Z). J.A.T. is supported by the MRC Metabolic Diseases Unit (MC_UU_00014/1).
Conflict of interest
The authors have nothing to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ruffle A , Cameron M , Jonas N et al. Lingual alveolar soft part sarcoma in a 1‐year‐old infant: youngest reported case with characteristic ASPSCR 1‐TFE 3 fusion. Pediatr. Dev. Pathol. 2019; 22; 391–395.30744536 10.1177/1093526619830290 · doi ↗ · pubmed ↗
- 2Shukla N , Levine MF , Gundem G et al. Feasibility of whole genome and transcriptome profiling in pediatric and young adult cancers. Nat. Commun. 2022; 13; 2485.35585047 10.1038/s 41467-022-30233-7PMC 9117241 · doi ↗ · pubmed ↗
- 3Deacon S , Cahyani I , Holmes N et al. ROBIN: a unified nanopore‐based sequencing assay integrating real‐time, intraoperative methylome classification and next‐day comprehensive molecular brain tumour profiling for ultra‐rapid tumour diagnostics. med Rxiv 2024; 2024.2009.2010.24313398. 10.1101/2024.09.10.24313398. · doi ↗
- 4Hodder A et al. Benefits for children with suspected cancer from routine whole‐genome sequencing. Nat. Med. 2024; 30; 1905–1912.38956197 10.1038/s 41591-024-03056-w PMC 11271414 · doi ↗ · pubmed ↗
- 5Yoshida H , Leiter SM , Kennedy J et al. Identification of COL 3A 1 and RAB 2A as novel translocation partner genes of PLAG 1 in lipoblastoma. Genes Chromosomes Cancer 2014; 53; 606–611.24700772 10.1002/gcc.22170 · doi ↗ · pubmed ↗
- 6Abdul‐Ghafar J , Ahmad Z , Tariq MU , Kayani N , Uddin N . Lipoblastoma: a clinicopathologic review of 23 cases from a major tertiary care center plus detailed review of literature. BMC. Res. Notes 2018; 11; 42.29343278 10.1186/s 13104-018-3153-8PMC 5773143 · doi ↗ · pubmed ↗
- 7Han JW , Kim H , Youn JK et al. Analysis of clinical features of lipoblastoma in children. Pediatr. Hematol. Oncol. 2017; 34; 212–220.29035641 10.1080/08880018.2017.1354949 · doi ↗ · pubmed ↗