Development and Technical Validation of an Integrated Risk Calculator for Acute Coronary Syndrome Using ChatGPT-Assisted Coding
Musab Egaimi, Pierfrancesco Corvo, Hasan Al Houri, Ji Min Chang, Heeyoung Seo, Alghafek Almorraweh, Wonsuk Choi, Hassan Badreldin, Sahla Bashir, Mohamed H Serour, Lara Merghani, Mohammed Al Natour, Musab Mukhtar, Fabrizio Clementi

TL;DR
This paper introduces a digital tool that combines three risk models for heart attacks into one interface, using AI to speed up development and improve accuracy.
Contribution
The novel contribution is an integrated calculator for TIMI, GRACE, and Mehran scores using AI-assisted coding, validated against clinical registries.
Findings
The calculator showed perfect agreement with TIMI and GRACE scores from clinical registries.
Manually reviewed Mehran scores were consistent with the tool's output.
The tool reduced data entry duplication and maintained accuracy.
Abstract
Introduction Acute coronary syndrome (ACS) remains a major contributor to cardiovascular morbidity and mortality, necessitating efficient and accurate risk-stratification tools. Widely used models such as the Thrombolysis in Myocardial Infarction (TIMI), Global Registry of Acute Coronary Events (GRACE), and Mehran scores require separate manual inputs, leading to workflow inefficiencies and transcription errors. This study introduces an integrated digital tool that consolidates these scoring systems into a single interface and explores the feasibility of AI-assisted development in clinical software design. Objective The objective of this study is to develop and technically validate an integrated ACS risk calculator that streamlines the computation of TIMI, GRACE, and Mehran scores while demonstrating the utility of AI-assisted coding in clinical applications. Methods A web-based…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
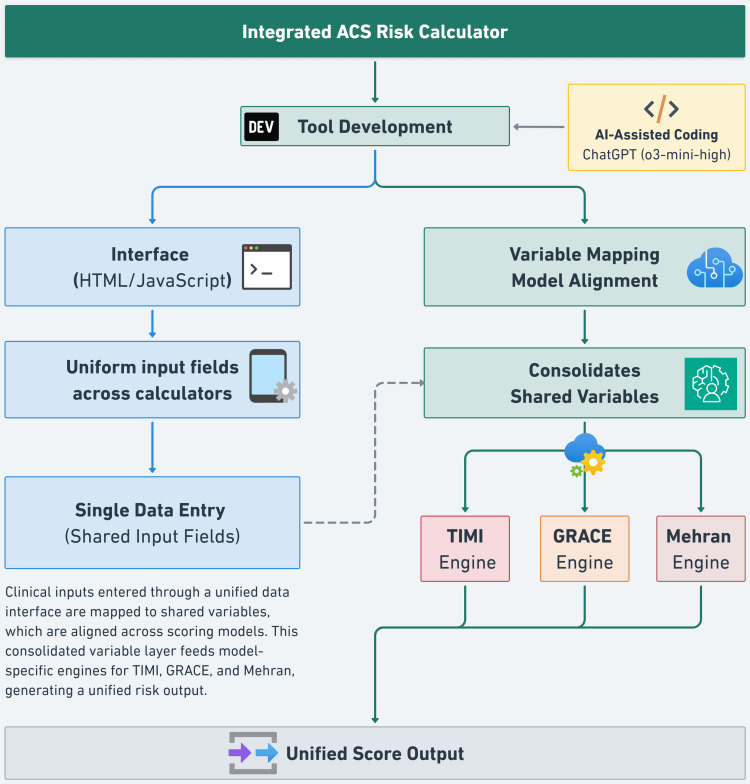 Figure 1
Figure 1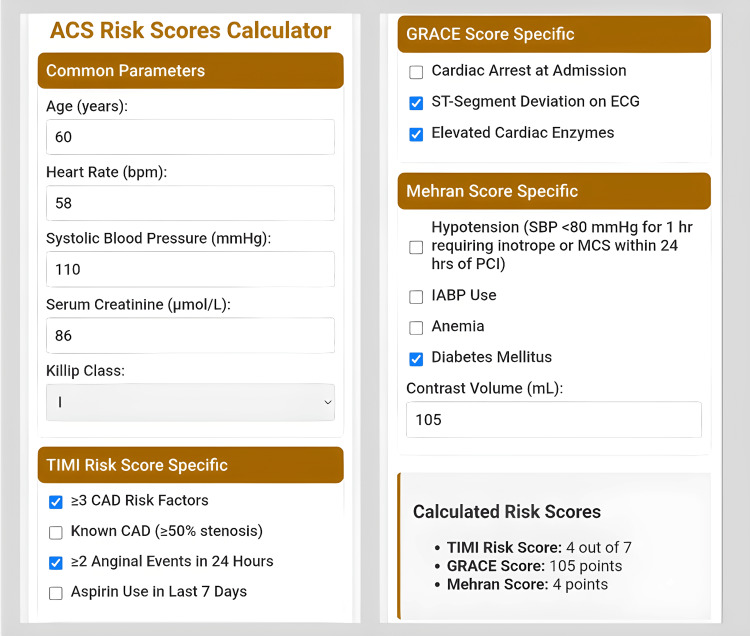 Figure 2
Figure 2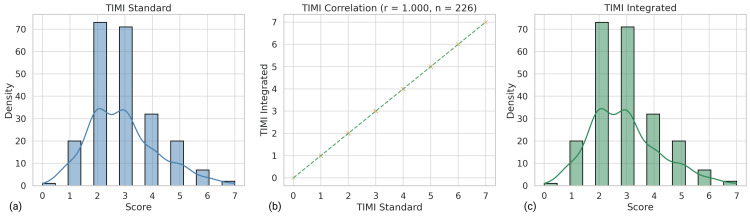 Figure 3
Figure 3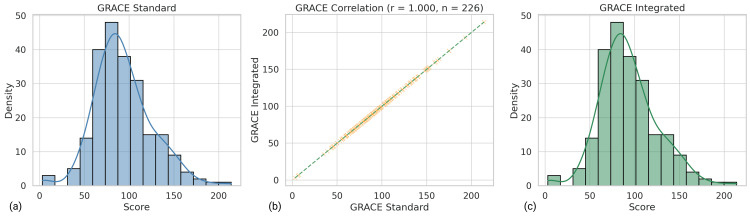 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Myocardial Infarction Research · Cardiac Imaging and Diagnostics · Artificial Intelligence in Healthcare and Education
Introduction
Acute coronary syndrome (ACS) remains a leading cause of cardiovascular morbidity and mortality worldwide, necessitating accurate risk stratification tools to guide clinical management and improve patient outcomes. Among the most widely used risk scores are the Thrombolysis in Myocardial Infarction (TIMI) score [1], the Global Registry of Acute Coronary Events (GRACE) score [2], and the Mehran score [3]. These models incorporate key clinical and laboratory parameters to predict short-term mortality, major adverse cardiac events (MACE), and procedural risks such as contrast-induced nephropathy (CIN).
Despite their clinical utility, a major limitation in practice is the need for separate data entry across multiple risk calculators, increasing the risk of transcription errors and workflow inefficiencies. To address this, we developed an integrated risk calculator that consolidates the TIMI, GRACE, and Mehran scoring systems into a single interface, aiming to streamline risk assessment and improve clinical workflow efficiency.
This study leverages data from the Get With The Guidelines-Coronary Artery Disease (GWTG-CAD) registry, an initiative by the American Heart Association (AHA) designed to enhance ACS outcomes and adherence to guideline-directed therapy [4]. The GWTG-CAD registry provides a structured national framework for quality improvement in cardiovascular care, systematically capturing clinical data, including TIMI and GRACE scores. While our integrated risk calculator incorporates TIMI, GRACE, and Mehran scores, validation of TIMI and GRACE was performed using the GWTG-CAD dataset, whereas Mehran score validation was explored through selective manual extraction and comparison of random patient samples.
Additionally, this study highlights the feasibility of clinician-led software development, utilizing AI-assisted coding tools such as ChatGPT (o3-mini-high) (OpenAI, San Francisco, CA) to facilitate rapid prototyping and deployment [5]. By integrating multiple risk stratification models into a single interface, we aim to improve accuracy, efficiency, and accessibility in ACS risk assessment.
Materials and methods
Study design
We conducted a technical validation study comparing the integrated tool’s performance against conventional TIMI and GRACE calculations. The calculator captures all three scores (TIMI, GRACE, and Mehran); however, validation was conducted for TIMI and GRACE using the GWTG-CAD dataset. The Mehran score is not captured in GWTG-CAD and was therefore validated separately against values retrieved from the hospital information system (HIS).
Tool development
A web-based Hypertext Markup Language (HTML)/JavaScript interface was designed to unify TIMI, GRACE, and Mehran scores into a single workflow. Overlapping clinical parameters were mapped into a streamlined data entry process, reducing redundancy and minimizing errors. The tool follows a structured input-to-output mapping system, allowing simultaneous calculation of multiple risk scores with minimal user input. Overlapping variables across TIMI, GRACE, and Mehran are entered once, optimizing efficiency and ensuring computational accuracy. The decision logic automates data processing, minimizes manual errors, and enables real-time risk assessment (Figure 1).
Figure created by the authors to illustrate the workflow schematic of the Integrated ACS Risk Calculator. The tool was developed using AI-assisted coding (ChatGPT o3-mini-high) and combines a standardized interface, built with HTML/JavaScript, with a unified backend logic for real-time calculation of TIMI, GRACE, and Mehran scores. Shared clinical variables are entered once and mapped across risk models via a consolidated data layer, enabling efficient and consistent risk stratification.ACS - Acute Coronary Syndrome; GRACE - Global Registry of Acute Coronary Events; HTML - Hypertext Markup Language; TIMI - Thrombolysis in Myocardial Infarction
To ensure compatibility across scoring systems, we implemented standardized variable mappings where clinically appropriate. For the Mehran score, congestive heart failure (CHF) was inferred based on Killip class, with CHF points assigned for Killip class > I (i.e., II-IV). This approach enabled harmonized data capture while maintaining alignment with the original Mehran definition of CHF as New York Heart Association (NYHA) class III/IV or pulmonary edema. Given the established use of Killip classification in ACS risk models and its ability to capture bedside evidence of pulmonary congestion, it serves as a pragmatic, if not direct, substitute in the acute setting where functional NYHA assessment is infeasible.
ChatGPT (o3-mini-high) was leveraged to assist in coding, debugging, and refining the tool’s user interface, demonstrating the potential of AI-driven clinician-led innovation [6]. The integrated system provides a single-point data entry, eliminating the need for repeated manual input and improving workflow efficiency (Figure 2).
User interface of the Integrated ACS Risk Calculator developed in this study. The screenshot illustrates a streamlined, single-entry system for calculating TIMI, GRACE, and Mehran scores. The design minimizes redundant data entry and consolidates outputs into a unified interface, improving clinical workflow.ACS - Acute Coronary Syndrome; CAD - Coronary Artery Disease; GRACE - Global Registry of Acute Coronary Events; TIMI - Thrombolysis in Myocardial Infarction
Technical validation
A de-identified dataset of 226 ACS patients admitted to Sheikh Khalifa Specialty Hospital (SKSH) between 2022 and 2023 was used for validation. For each patient, we computed TIMI and GRACE using the integrated tool and compared them against the values extracted from the GWTG-CAD registry methods. A Pearson correlation analysis was performed to assess the consistency between captured values and recalculated values using the integrated tool.
Because the Mehran score is not captured in our GWTG-CAD dataset, validation was performed on a subsample of 30 patients - selected to span the observed score distribution - whose required clinical variables (age, baseline creatinine, contrast volume, Killip class, etc.) were extracted from the HIS and input into the calculator, then cross-referenced against the Mehran score already calculated and stored in the HIS. A working version of the calculator, including all source HTML/JavaScript, is publicly accessible (see Appendices).
Results
Among the 226 patient records analyzed, every TIMI and GRACE value produced by the calculator matched its corresponding registry entry exactly. This identity is reflected in the Pearson coefficients (TIMI r = 1.000, p < 0.001; GRACE r = 1.000, p < 0.001), as shown in Figure 3 and Figure 4, confirming that the tool reproduces the arithmetic logic of both scores. A random, blinded audit of 30 cases for the Mehran algorithm likewise revealed 100% concordance between manual and automated calculations, supporting accurate implementation across all three models.
Visual validation of TIMI score agreement between the standard method and the integrated ACS Risk Calculator. (a) Distribution of TIMI scores from the standard method based on registry values. (b) Scatter plot illustrating perfect correlation (r = 1.000, n = 226) between integrated and standard TIMI scores. (c) Distribution of TIMI scores generated by the integrated calculator. These panels confirm that the integrated tool reproduces TIMI scores with full fidelity across the dataset.ACS - Acute Coronary Syndrome; TIMI - Thrombolysis in Myocardial Infarction; r - Pearson correlation coefficient; TIMI Standard - TIMI score calculated using the standard method; TIMI Integrated - TIMI score generated by the integrated calculator
Visual validation of GRACE score agreement between the standard method and the integrated ACS Risk Calculator. (a) Distribution of GRACE scores calculated using the standard method from the registry dataset. (b) Scatter plot showing perfect correlation (r = 1.000, n = 226) between GRACE scores computed by the integrated tool and the registry-based standard values. (c) Distribution of GRACE scores generated by the integrated tool. All subpanels demonstrate full computational agreement, confirming the integrated tool's accuracy.ACS - Acute Coronary Syndrome; GRACE - Global Registry of Acute Coronary Events; GRACE Standard - GRACE score calculated using the standard method; GRACE Integrated - GRACE score generated by the integrated calculator; r - Pearson correlation coefficient
While perfect correlation demonstrates numeric equivalence, it does not by itself exclude subtle systematic bias. Accordingly, a follow-up phase will apply full agreement analyses, including intraclass-correlation coefficients and Bland-Altman plots, to complement these initial findings and provide a more granular assessment of measurement fidelity.
Discussion
This study demonstrates that an integrated risk calculator can successfully consolidate TIMI, GRACE, and Mehran scores into a single tool, reducing redundant data entry while maintaining the accuracy of validated risk models. By eliminating multiple data entry points, the tool enhances workflow efficiency, mitigates transcription errors, and facilitates faster clinical decision-making.
Technical validation demonstrated exact replication of TIMI and GRACE scores (Pearson r = 1.000 for both; p < 0.001) and 100 % concordance in a blinded audit of 30 Mehran cases, confirming the calculator’s computational accuracy across all three risk models. However, perfect correlation alone does not preclude subtle systematic bias, highlighting the importance of subsequent agreement studies, such as intraclass‐correlation coefficients and Bland-Altman analyses, to deepen assessment of measurement fidelity. Future work will focus on evaluating real-world clinical adoption, including time savings and user experience studies.
To pragmatically implement the heart failure component of the Mehran score in a real-time digital tool, we used Killip class > I as a surrogate for CHF. Although the original Mehran model defines CHF as NYHA class III/IV or pulmonary edema, NYHA classification is impractical at initial presentation, whereas Killip class is routinely applied and reflects bedside assessment of pulmonary congestion and hemodynamic compromise. This substitution is supported by studies showing that Killip class ≥2 correlates with objective markers of acute heart failure and predicts post-discharge CHF risk. For example, in the INFUSE-AMI trial, Killip class ≥2 at presentation was an independent predictor of NYHA class ≥2 symptoms at 30 days, which were in turn associated with a four-fold increase in heart failure hospitalization and mortality at one year [7]. Similarly, in the AMI-Kyoto Risk Study, Killip class ≥2 patients undergoing percutaneous coronary intervention (PCI) exhibited significantly higher in-hospital mortality and rates of left ventricular dysfunction, hallmarks of NYHA class III/IV CHF [8]. Additionally, Sgura et al. demonstrated that higher Killip class and CHF presence at admission were strong predictors of long-term rehospitalization for heart failure and adverse outcomes following primary PCI, directly validating the CHF component of the Mehran score in this clinical context [9].
Moreover, this study highlights the growing role of AI-driven software development in clinical decision support. The successful utilization of ChatGPT (o3-mini-High) in the development process enabled rapid code generation, real-time debugging, and refinement of the tool. These findings align with recent studies emphasizing the potential of AI to accelerate clinician-led innovation in medical informatics [10].
While the integrated tool improves efficiency, future research should evaluate its clinical impact on decision-making and patient outcomes. Additionally, efforts should be made to integrate the calculator into electronic health records (EHRs) to further streamline risk assessment in hospital settings.
Limitations
This study focused exclusively on technical validation, assessing the integrated tool’s ability to replicate existing scores; it did not evaluate clinical outcomes, decision-making impact, or usability in real-time practice. Validation of Mehran scores was limited to a small subset of manually extracted records and was not conducted at scale; comprehensive validation remains a future direction. Additionally, while Killip class was used as a practical proxy for NYHA III/IV CHF, further validation comparing Killip and NYHA equivalence in this context would strengthen this mapping.
Conclusions
We successfully developed and technically validated an integrated ACS risk calculator that consolidates the TIMI, GRACE, and Mehran scoring systems into a single digital platform. The tool demonstrated full statistical consistency with conventional methods for TIMI and GRACE scores, and manual review confirmed accurate implementation of the Mehran scoring logic. By eliminating redundant data entry and harmonizing overlapping clinical variables, the tool improves workflow efficiency and supports real-time risk assessment in ACS settings. The integration of the Killip class as a surrogate for heart failure enables standardized input across models while preserving clinical coherence.
This study also highlights the feasibility of clinician-led, AI-assisted development in the design of decision-support tools. Future work should focus on clinical validation, real-world adoption, and integration with EHR systems to maximize the tool’s impact in practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The TIMI risk score for unstable angina/non-ST elevation MI: a method for prognostication and therapeutic decision making JAMA Antman EM Cohen M Bernink PJ 83584228420001093817210.1001/jama.284.7.835 · doi ↗ · pubmed ↗
- 2Prediction of risk of death and myocardial infarction in the six months after presentation with acute coronary syndrome: prospective multinational observational study (GRACE)BMJ Fox KA Dabbous OH Goldberg RJ 109133320061703269110.1136/bmj.38985.646481.55PMC 1661748 · doi ↗ · pubmed ↗
- 3A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention: development and initial validation J Am Coll Cardiol Mehran R Aymong ED Nikolsky E 139313994420041546431810.1016/j.jacc.2004.06.068 · doi ↗ · pubmed ↗
- 4Synthesizing lessons learned from get with the guidelines: the value of disease-based registries in improving quality and outcomes Circulation Ellrodt AG Fonarow GC Schwamm LH 2447246012820132416657410.1161/01.cir.0000435779.48007.5c · doi ↗ · pubmed ↗
- 5Chat GPT in action: analyzing its use in software development MSR Int Conf Min Softw Repos Champa AI Rabbi MF Nachuma C Zibran MF 1145102024
- 6Analysis Chat GPT potential: transforming software development with AI chat bots 2023 International Conference on Networking, Electrical Engineering, Computer Science, and Technology (I Con NECT) Purwoko JW Abdullah T Wijaya B Santoso Gunawan AA Saputra KE Bandar Lampung, Indonesia IEEE
- 7Correlates and prognostic impact of new-onset heart failure after ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention: insights from the INFUSE-AMI trial Eur Heart J Acute Cardiovasc Care Giustino G Redfors B Brener SJ 339347720182882888110.1177/2048872617719649 · doi ↗ · pubmed ↗
- 8Predictors of in-hospital outcomes after primary percutaneous coronary intervention for acute myocardial infarction in patients with a high Killip class Intern Med Shiraishi J Kohno Y Nakamura T 9339395320142478588310.2169/internalmedicine.53.1144 · doi ↗ · pubmed ↗