From Velocity to Acceleration: A Perspective on Age-Related Visual Field Progression in Glaucoma
Masaki Tanito, Tomoki Shirakami

TL;DR
This paper argues that measuring visual field decline in glaucoma should include acceleration, not just rate, to better predict progression in older patients.
Contribution
The paper introduces the concept of incorporating acceleration into visual field progression assessments for glaucoma.
Findings
VF sensitivity decline is inherently nonlinear with age, as shown by a cubic model for healthy eyes.
A quadratic model captures the interaction between disease duration and baseline age in glaucomatous eyes.
Progression accelerates over time, suggesting treatment should consider acceleration based on age and disease course.
Abstract
The conventional evaluation of visual field (VF) progression in glaucoma often relies on linear regression to estimate the rate of decline, focusing on velocity (dB/year). However, this approach may underestimate future progression, particularly in elderly patients. This editorial highlights the importance of incorporating acceleration (dB/year²) into clinical assessments of VF loss. Using physiological and pathological models, we demonstrate that VF sensitivity decline is inherently nonlinear with age. A cubic model illustrates age-related sensitivity loss in healthy eyes, while a quadratic model captures the interaction between disease duration and baseline age in glaucomatous eyes. These models emphasize that progression accelerates over time and suggest that individualized treatment intensity should consider not only the current rate of VF decline but also its likely acceleration…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
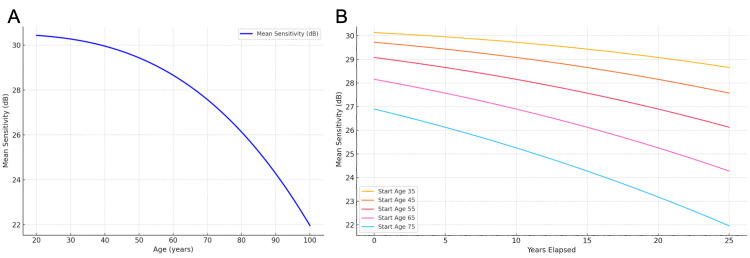 Figure 1
Figure 1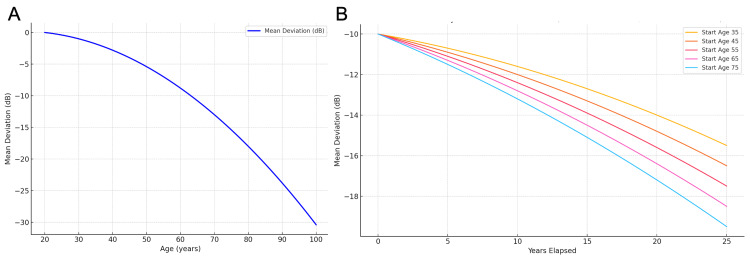 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlaucoma and retinal disorders · Corneal surgery and disorders · Retinal Imaging and Analysis
Editorial
The primary goal of glaucoma therapy is to preserve visual function and the associated quality of life throughout the patient's lifetime [1]. Slowing visual field (VF) loss by lowering intraocular pressure (IOP) remains the most reliable strategy for glaucoma treatment. Therefore, regular assessment of the rate of VF progression is essential when deciding whether the current target IOP is adequate or if additional intervention is required. Large-scale studies have demonstrated that older age is a risk factor for both the onset and progression of ocular hypertension, primary open-angle glaucoma, exfoliation glaucoma, and primary angle closure disease [2-8]. Given that glaucoma is a chronic and progressive disease, these findings suggest that the impact of age on glaucoma progression increases over time.
VF progression is conventionally assessed by determining the rate of change in sensitivity values via linear regression. For example, the Guided Progression Analysis module of the Humphrey Field Analyzer (Carl Zeiss Meditec, Jena, Germany) employs the annual visual field index (VFI) slope (VFI/y) [9], and commercial software such as BeeFiles (BeeLine, Tokyo, Japan) likewise reports the mean deviation (MD) slope (MD/y) [10]. Although these metrics are useful for quantifying current progression speed, they may not fully predict future VF decline. Indeed, age-related vulnerability of neural tissues can lead to accelerated thinning of the retinal nerve fiber layer even at constant IOP levels [11]. Therefore, when evaluating VF progression, it is essential to consider not only the current rate (velocity, dB/y) but also the potential for increasing rate (acceleration, dB/y²). This editorial emphasizes the importance of incorporating the concept of acceleration alongside that of velocity.
Spry and Johnson demonstrated that even in normal eyes, VF sensitivity declines with age in a nonlinear fashion [12]. Their analysis of healthy subjects demonstrated that age-related changes in sensitivity were better captured by a cubic function. The position function (S), which represents the VF sensitivity in decibels at age x in years, is defined as \begin{document}\text{S}\left( \text{x} \right)=-8.54×10^{⁻⁶}×\text{x}^{³}+30.5\end{document} .
In their original work, only this position function was presented [12]. For the purpose of this editorial, we further derived the first and second derivatives of the position function to represent the rate of change and acceleration of VF loss with age. The velocity function (S/y), describing the yearly rate of VF sensitivity decline, is given by \begin{document}\text{S’}\left( \text{x} \right)= -2.562 × 10^{⁻⁵}×\text{x}^{²}\end{document} . The acceleration function (S/y²), indicating the age-related acceleration of sensitivity loss, is \begin{document}\text{S’’}\left( \text{x} \right)=-5.124×10^{⁻⁵}×\text{x}\end{document} .
These derived expressions demonstrate that even in the absence of disease, the decline in sensitivity is not constant but accelerates with age (Figure 1A, 1B). This physiologic baseline serves as a foundation for comparison with glaucomatous damage.
Age-related decline in VF sensitivity in normal eyes, based on Spry and Johnson's cubic model.(A) Projected lifelong trajectory of VF sensitivity for a baseline age of 20 years. (B) Projected 25-year trajectories of VF sensitivity for baseline ages of 35, 45, 55, 65, and 75 years.VF: visual fieldReference: [12]
In glaucomatous eyes, Shirakami et al. [13] proposed a quadratic model to describe the progression of VF loss over time, incorporating time since diagnosis (t) and baseline age (b). The position function (MD), also denoted as y(t), is given by \begin{document}\text{y}\left(\text{t}\right)=-0.004×\text{t}^{2}+\left(-0.004×\text{b}+0.02\right)×\text{t}+\text{C’}\end{document} , where C’ is a constant representing the baseline MD. The velocity function (MD/y), or y’(t), representing the yearly rate of MD change, is \begin{document}\text{y’}\left( \text{t} \right)= -0.008 ×\text{t}- 0.004 ×\text{b}+ 0.02\end{document} . The acceleration function (MD/y²), or y”(t), which describes the constant rate of acceleration in MD loss, is \begin{document}\text{y”}\left(\text{t}\right)= -0.008\end{document} .
In this model, the decline in MD is not only nonlinear but also dependent on the patient's age at diagnosis. Older patients exhibit a higher progression rate, highlighting the compounding effects of aging and disease duration (Figure 2A, 2B).
Age-related VF decline in glaucomatous eyes derived from the Shirakami et al. quadratic model.(A) Projected lifelong trajectories of VF sensitivity (starting MD = 0 dB; baseline age = 20 years). (B) Projected 25-year trajectories of VF MD in glaucomatous eyes starting from −10 dB for baseline ages of 35, 45, 55, 65, and 75 years.VF: visual field; MD: mean deviationReference: [13]
These VF progression models [12,13] demonstrate that relying solely on linear slopes risks underestimating true progression, especially in elderly patients. In the clinical setting, incorporating the concept of potential acceleration in disease progression may influence treatment strategies, patient counselling, and clinical outcomes, particularly when considering current progression rate and patient life expectancy. It is desirable that future software for VF assessment include metrics related to acceleration.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The Japan Glaucoma Society guidelines for glaucoma 5th edition Jpn J Ophthalmol Kiuchi Y Inoue T Shoji N Nakamura M Tanito M 1892546720233678004010.1007/s 10384-022-00970-9 · doi ↗ · pubmed ↗
- 2The Ocular Hypertension Treatment Study: baseline factors that predict the onset of primary open-angle glaucoma Arch Ophthalmol Gordon MO Beiser JA Brandt JD 71472012020021204957510.1001/archopht.120.6.714 · doi ↗ · pubmed ↗
- 3Validated prediction model for the development of primary open-angle glaucoma in individuals with ocular hypertension Ophthalmology Gordon MO Torri V Miglior S 101911420071709509010.1016/j.ophtha.2006.08.031PMC 1995665 · doi ↗ · pubmed ↗
- 4Risk factors for open-angle glaucoma in a Japanese population: the Tajimi Study Ophthalmology Suzuki Y Iwase A Araie M 1613161711320061682850410.1016/j.ophtha.2006.03.059 · doi ↗ · pubmed ↗
- 5The Advanced Glaucoma Intervention Study (AGIS): 3. Baseline characteristics of black and white patients Ophthalmology 113711451051998966321410.1016/s 0161-6420(98)97012-9 · doi ↗ · pubmed ↗
- 6Reduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma Trial Arch Ophthalmol Heijl A Leske MC Bengtsson B Hyman L Bengtsson B Hussein M 1268127912020021236590410.1001/archopht.120.10.1268 · doi ↗ · pubmed ↗
- 7Risk factors for visual field deterioration in the United Kingdom Glaucoma Treatment Study Ophthalmology Founti P Bunce C Khawaja AP DoréCJ Mohamed-Noriega J Garway-Heath DF 1642165112720203254032510.1016/j.ophtha.2020.06.009 · doi ↗ · pubmed ↗
- 8Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis Ophthalmology Tham YC Li X Wong TY Quigley HA Aung T Cheng CY 2081209012120142497481510.1016/j.ophtha.2014.05.013 · doi ↗ · pubmed ↗