Acute Kidney injury of glomerular origin in Asian population: Causes and outcomes - Meta-Analysis
Sakina Abbas, Aleena Aftab, Ahya Aziz, Rubina Naqvi

TL;DR
This meta-analysis summarizes the causes and outcomes of glomerular acute kidney injury in Asian populations based on 21 studies.
Contribution
The study compiles and analyzes data on glomerular acute kidney injury in Asia, highlighting regional patterns and outcomes.
Findings
Most studies were from China and India, with 4,077 patients analyzed in total.
Outcomes varied widely, with renal replacement needs from 7-80% and recovery rates from 9-96%.
Lupus nephritis and AAV were among the most common causes identified.
Abstract
To collect all studies on acute kidney injury of glomerular origin, published from Asia, even with their limitations, and look for causes and outcome in this particular population. As of June 2024, a comprehensive literature search was conducted in the databases of PubMed, Cochrane Library, Web of Science, Embase, Google Scholar and PubMed Central, for full-text articles in English language, describing original articles on acute kidney injury of glomerular origin published from Asia. There was no time limit set for searching year of publication. Combinations of key words used were ‘acute kidney injury’ or ‘acute renal failure’ or ‘acute kidney injury of glomerular origin’ or ‘glomerular diseases causing acute kidney injury’ along with using ‘Asia’. Data was extracted and analyzed. Of the 21 studies subjected to detailed analysis, 10(47.61%) had been published from China, 4 (19 %) from…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
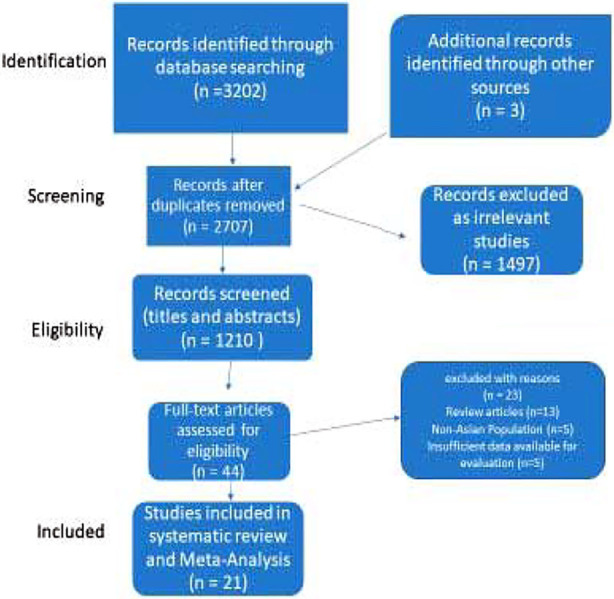 Fig.1
Fig.1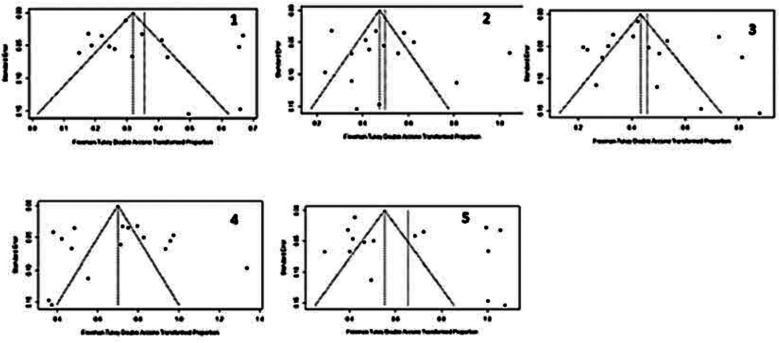 Fig.2
Fig.2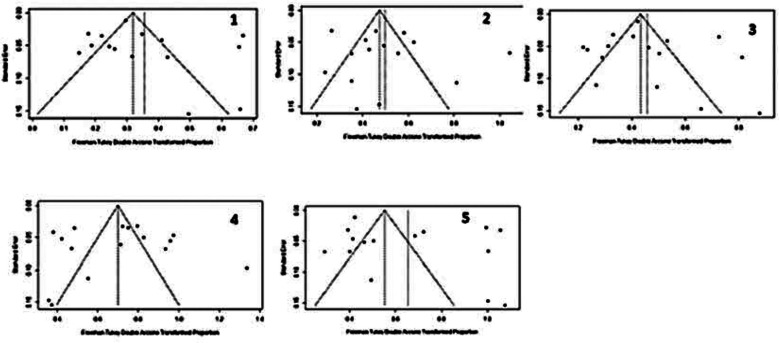 Fig.3
Fig.3| Author | Year of Publication | Study design | Study population | Country | Gender n(%) | Age in years mean±sd (range) | Glomerular injury | Duration of follow-up (months) | Definition of AKI | Need for RRT (%) | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Alexander S | 2020 | observational retrospective cohort | 200 | India | M=80 (40) | 40.6±14.6 | Mixed (Lupus=41AAV=38 ANCA neg vas =37 PIGN=23 IgA=21 Anti GBM=21Dual Anti GBM and AAV=10 MPGN=4C1q Neph=3 HSP=1) | 9.4±15 | Histological presence of crescents | 87 (43.5) | Rec=43 (21.5) |
| Chan PCK | 1989 | observational retrospective cohort | 11 | Hong-Kong | M=0 F=11(100) | 33.5 | Lupus Nephritis | 12-144 (mean 76.5) | Histology based | 8(72) | Rec=1 (9) |
| Chen S | 2016 | observational retrospective | 307 | China | M=120 (39) | 37.6±16.4 | Crescentic GN | 120 | Histological presence of crescents | 216 (70) | NA |
| Chen XY | 2011 | observational retrospective cohort | 92 | China | M=48 (52) | 57.7±16.75 | AAV | 12- 132 | RIFLE Criteria | 18 (20) | Rec=15 (16) |
| Chen Z | 2022 | observational retrospective cohort | 56 | China | M=26 (46) | 54.29±15.90 | AGN | 12-96 | Histological presence of crescents | 40 (71) | Rec=NA CKD=42 (75) |
| Fatemi A | 2013 | observational retrospective cohort | 82 | Iran | M=17 (21) | 32.3± 11.4 (13–69) | Lupus nephritis | 96 | Creatinine >1.5 mg/dl | NA | Rec=55 (67) |
| Gandhi TS | 2024 | observational prospective | 100 | India | M=56 (56) | 40-60 | PIGN | 7.8 | Abrupt reduction in GFR | 23 (23) | Rec=54 (54) |
| Ge H | 2020 | observational retrospective cohort | 26 | China | M=18 (70) | 13 (10-15) | AGN | 16-73 | Abrupt reduction in GFR | 0 | Rec=25 (96) |
| Hari P | 2009 | observational retrospective cohort | 54 | India | M=14 (26) | 10.4 ± 2.6 (3-15) | Lupus Nephritis | 6-123 | Abrupt reduction in GFR | 4 (7.4) | Rec=35 (65) |
| Herath N | 2017 | observational retrospective cohort | 20 | Sri Lanka | NA | 28 (13–60) | Lupus nephritis | 12-72 | Doubling of serum creatinine | NA | Rec=NA CKD=2 (10) |
| Huang X | 2021 | observational retrospective | 141 | China | M=65 (46) | 59.6 (median) | AAV | 64 | KDIGO | 56 (40) | Rec=19(13.4) |
| Jin SY | 2017 | observational retrospective cohort | 242 | China | M=55 (23) | 11.7 ±2.8 | Lupus Nephritis | 21.5 ±18.4 | Abrupt reduction in GFR | 35 (14.46) | Rec=123 (71) |
| Koubar SH | 2019 | observational retrospective | 55 | China | M=13 (24) | 29±11 | Lupus Nephritis | 120 | Rise of creatinine of 0.3 mg/dl from baseline | 8 (15) | Rec=11 (20) |
| Lee H | 2013 | observational retrospective cohort | 1943 | Korea | M=911 (47) | median 42 | Mixed | median 90 | Abrupt reduction in GFR | 325 (16.7) | Rec=NA CKD=NA ESRF=325 (16.7) |
| Li FK | 2004 | observational retrospective cohort | 10 | Hong Kong | M=2 (20) | 58.6 ± 21.7 | Anti-GBM disease | 12 -144 | Abrupt reduction in GFR | 8 (80) | Rec=1 (10) |
| Mosaad FG | 2018 | observational retrospective cohort | 19 | Saudi Arabia | M= 13 (68.5) | 8.52±3.15 | PIGN (63.2%), LN (21.1%) | 12-120 | pRIFLE | 4 (21) | Rec=5 (26) |
| Naqvi R | 2015 | observational retrospective | 236 | Pakistan | M= 103 (43.6) | 27.94 ± 12.79 | Mixed (GN with Crescents=118 GN without Crescents=78 AAV = 19 Anti-GBM = 8 Lupus=20 PIGN=34 MCGN=8) | 300 | RIFLE Criteria | 179 (76) | Rec=103 (44) |
| Shankar M | 2022 | observational retrospective | 114 | India | NA | 37.05 ± 18.26 | PIGN | 36 | Histology based | 18 (15.7) | Rec=78 (68.4) |
| Tang Z | 2009 | observational retrospective cohort | 94 | China | M=10 (10.6) | 27.9 ± 10.7 | Lupus nephritis, Crescentic GN | 37.9±38.5 | Histological presence of crescents | NA | Rec=NA CKD=NA ESRF=4 (4.2) |
| Wang Y | 2005 | observational retrospective | 209 | China | M=124 (59) | 56.4±16.1 (18-92) | Crescentic GN in 36%of Biopsies | 120 | Rise of creatinine upto 2 mg/dl over hours or days | NA | Rec=97 (46) |
| Zhu D | 2011 | observational retrospective cohort | 66 | China | M= 18 (27) | 33.3±11.9 | Lupus nephritis | 53.6±57.1 | Abrupt reduction in GFR | NA | Rec=28 (51) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Kidney Disease and Diabetes
INTRODUCTION
Acute kidney injury (AKI), formerly called acute renal failure (ARF), is a sudden decline in kidney function that often can be reversed. It leads to waste accumulation, electrolyte imbalances, and reduced urine output, marked by a rapid rise in serum creatinine or decreased urine output. The severity can vary from mild dysfunction to severe failure, sometimes requiring renal replacement therapy (RRT), like dialysis. Identifying the cause of AKI is essential for effective treatment and improving patient outcomes. AKI can result from various causes, broadly categorized into pre-renal, intrinsic (renal), and post-renal factors.1
Glomerulonephritis has frequently been reported as cause of AKI from some parts of world,2 whereas from Asian countries particularly from Pakistan it has been reported to contribute 4% of total community acquired AKI.3 Glomerular disorders which can cause AKI may arise from immune-mediated disorders, infections, or systemic diseases like diabetes and lupus. The high prevalence of infections such as hepatitis B and C, which are associated with glomerulonephritis has been reported from Korea.4 Additionally, autoimmune diseases like systemic lupus erythematosus (SLE), more common in certain Asian populations, contribute to the increased risk of glomerular disease-induced AKI.5 AKI caused by glomerular diseases often leads to variable outcomes, heavily influenced by the severity of the underlying condition and the timeliness of treatment.
Studies indicate that from very low to moderately high i.e. 7-76% of patients with glomerular disease-induced AKI require RRT, during the acute phase due to significant loss of kidney function.6,7 Despite treatment, the recovery rates can vary widely. Complete renal recovery has been reported from 9-96% 8,9 4-75% of these patients may recover sufficient kidney function to discontinue dialysis within weeks to months.9,10 However, a substantial proportion, particularly those with severe or inadequately managed glomerular diseases, may experience end stage kidney failure, reported 4-44% in different studies.11,12 Considering the importance of timely referring and managing the patients with any sort of glomerulonephritis leading to AKI, we aimed to collect published studies on subject from Asia and perform a meta-analysis. So that awareness lacking about the seriousness of issue can be highlighted.
METHODS
This Meta-Analysis was performed in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 expanded checklist.13 During month of June 2024 search was made using following combinations on search engines PubMed/ PubMed Central, Cochrane, Elsevier, Science Direct, Embase, Web of Science and Google Scholar. {(“acute kidney injury” OR “AKI”) AND (“RPGN” OR “Rapidly progressive glomerulonephritis”) AND (“lupus nephritis”) AND (“ANCA positive vasculitis”) AND (“pauci immune glomerulonephritis”) AND (“Anti GBM disease”) AND (“Asian” OR “asian population”) OR “Afghanistan” OR “Bangladesh” OR “China” OR “India” OR “Pakistan” Or “Nepal” OR “Sri Lanka”)} AAz, SA and AAb independently completed the search. The relevant studies were imported to Endnote X9 (Clarivate Analytics, US). After removing duplicates, titles and abstracts were screened by AAz, SA and AAb for relevance. Full text of potentially relevant articles were then reviewed for eligibility.
Inclusion Criteria:
- Was based on the following: language, study design, intervention, patient population, comparison, definition, and outcomes of interest.
- Language: English publications.
- Study design: eligible completed randomized clinical trials or observational studies.
- Patient population: Adults and Children with acute kidney injury of glomerular origin in Asia only.
- Definitions: AKI definitions used were RIFLE, KDIGO, abrupt decline in GFR or histological based.
- Intervention: need for renal replacement therapy.
- Causes: all types of glomerulonephritis (GN), whether labeled as acute GN, Crescentic GN, Post Infection GN (PIGN), ANCA associated vasculitis (AAV), anti GBM disease.
- Outcomes of interest: complete renal recovery, Chronic Kidney Disease (CKD), End Stage Renal Failure (ESRF), or mortality during acute illness.
Exclusion Criteria:
- No clear definition of population and types of glomerular diseases.
- Duplicates of previous publications.
- Insufficient data for estimating mean difference (MD) with a 95% confidence interval (CI).
- Children and adults with glomerular disease but no AKI.
- Systematic reviews, comments, reviews, single-arm studies, case-controlled studies.
The three investigators (AAz, SA and AAb) then independently extracted data which comprised authors names, publication year, country from study published, study design, age, gender, definition of AKI, type of glomerular disease, need for RRT, duration of follow-up and outcome in categories of complete renal recovery, progression to CKD or ESRF and mortality. R studio (version 4.16-2) was used for statistical analysis of studies, including drawing of Forest and Funnel plot. Quality of included study was checked and it was scored 8-9 in all.
RESULTS
Literature Search Results:
Following an extensive search (done by three authors independently) across the following electronic databases: PubMed, PubMed Central, Embase, Google Scholar, Cochrane Library, Web of Science, a total of 3,205 records were identified. After the removal of 498 duplicate studies and 1,497 irrelevant records, 1,210 studies (abstracts) were assessed for eligibility. Subsequently, 44 studies found eligible, underwent full-text review and ultimately 21 studies were included in the systematic review and meta-analysis. The PRISMA flow diagram of the study selection procedure is summarized in Fig.1.
PRISMA Flow Chart.
Study Characteristics:
Among the 21 studies retained after screening and full-text review, ten originated from China, four from India, two from Hong-Kong, and one each from Iran, Pakistan, Korea, Saudi Arabia and Sri Lanka. The studies included were published between 1989 and 2024. The studies varied in sample size and event rates contributing to a comprehensive analysis of a total of 4,077 participants with a female: male ratio of 1.32:1 (Females=57.06%, Males=42.93%). In the selection of 21 studies, only one was a prospective observational study, while the remaining 20 studies were retrospective observational studies. The average age of the subjects differed across all studies, primarily encompassing young adults to middle-aged participants. The primary characteristics of the articles are shown in Table-I.
Analysis of the Outcomes of AKI Secondary to Glomerular causes (Fig.2):
Forest plots for all-cause mortality. (l), CKD (2), ESRF (3), Complete Renal Recovery (4) and need for Renal Replacement Therapy (5). The red squares indicate point estimate of the effect of individual study with size representing weight of study and the horizontal lines represent the 95% confidence interval (CI). The dotted line represents the pooled estimate, and the diamond represents the overall effect estimate of meta-analysis. Heterogeneity outlined at near the bottom of forest plot.
i. ESRF: In a collective analysis of 16 studies encompassing 3,338 patients, the likelihood of end-stage renal failure (ESRF) following acute kidney injury (AKI) attributable to glomerular causes was evaluated. The risk of ESRF development was assessed using both fixed-effect and random-effects models, yielding odds ratios (OR) of 0.17 (95% CI= 0.15;0.18) and 0.19 (95% CI = 0.12;0.27) respectively. These findings suggest that individuals experiencing AKI stemming from glomerular injury are at a substantial risk of progressing to ESRF.
ii. CKD: A total of 15 studies involving 1,291 patients assessed the risk of progression to CKD after AKI of glomerular origin. The risk of CKD progression assessed using both fixed-effect and random-effects models was 0.20 (95% CI= 0.18;0.22) and 0.22 (95% CI= 0.14;0.32), respectively, suggesting 18% risk of CKD progression in patients with glomerular injury leading to AKI.
iii. Complete Renal Recovery: A total of 16 studies involving 1,657 patients assessed the likelihood of complete renal recovery after glomerular injury has caused AKI, the OR (95% CI) under fixed-effect and random-effects models was 0.41 (0.39; 0.43) and 0.41 (0.28; 0.54), respectively, indicating 29% odds of Complete Renal Recovery after glomerular injury induced AKI.
iv. Renal Replacement Therapy: A total of 15 studies involving 3,580 patients assessed the probability of Renal Replacement Therapy (RRT) requirement, revealing the OR (95% CI) of 0.27(0.25; 0.28) and 0.36 (0.23; 0.51) under fixed-effect and random-effects models respectively.
v. All-Cause Mortality: A total of 15 studies involving 3,536 patients assessed for the extent of All-Cause Mortality after AKI originated by Glomerular injury, the OR (95% CI) under both fixed-effect and random-effects models was 0.09 (0.08; 0.10) and 0.11 (0.06; 0.18), respectively.
Analysis of the Funnel Plots (Fig.3):
A funnel plot was constructed for each outcome by plotting the effect estimates from individual studies against their standard errors. The symmetry of the plot was assessed visually. All the funnel plots demonstrate considerable asymmetry, indicating significant heterogeneity and variability in the effect sizes. The asymmetry suggests potential biases, which may include publication bias or small-study effects.
Funnel Plots for different outcomes and need for RRT. 1= Mortality, 2= CKD, 3= ESRF, 4= Complete Renal recovery, 5= Need for RRT.
DISCUSSION
It is difficult to estimate actual burden and different causes of AKI, and outcome for these patients in Asian countries as many of these are lying in category of low income or lower middle income; according to World Bank classification based on per capita income, updated in July 2022.14 Budget spent on health care is very low in these countries and in majority of countries there is no proper state based health care provision. This results many of patients not reaching to proper nephrology set-up, those who reach tend to disappear amidst treatment mainly because of financial reasons. Furthermore, treated patients records are not maintained and health care providers lack facility of keeping records and enough funds to support publishing the results. This left us with very few published studies on topic of interest and hence lack of knowledge about complexity of disease and validity of management protocols.
Glomerular diseases causing AKI, in comparison to other cause of tubular or interstitial origin, have been reported to reveal high frequency of leading to CKD and over time eventually ESRF.12,15 This cause further burden on health budget of individual as well as state. For present meta-analysis extensive literature search on multiple search engines and giving the time and age limit, after removing duplicates and extracting through eligibility criteria we only left with 21 original studies on topic of interest. Even among these 21 some were lacking bit information about details of outcome.
Current study first of its kind that is addressing in a meta-analysis the AKI of glomerular origin from Asian continent. This meta-analysis highlights the following points; firstly, with heterogeneity of 91-95% among outcomes we found that wide variety among stages of AKI has been reported in different studies included in current meta-analysis. So is evident for management as supported with heterogeneity of 98% for need of RRT. Secondly, up to 44% patients registering as AKI at base line developing ESRF12, this is of serious note for nephrologist as well as health care community as a whole and affects economic states in health care. As patients with ESRF will be requiring lifelong RRT in one or other form.
In many of Asian countries RRT is not supported by insurance program or by state thus contribute in invisible rise in number of deaths under nephrology care patients. Funnel plots in current analysis were meant more for generic means of examining small study effects, rather as a tool to detect specific types of bias. As every center implies own definition of AKI and people do not tend to report outcome on any universally described outline, thus biases among studies is expected in such kind of analysis. The studies included in present meta-analysis revealed variations in definitions of AKI,5-12,15-27 some considered abrupt rise in creatinine, some as doubling of serum creatinine from baseline, others mentioned serum creatinine of more than 2 mg/dl, some described abrupt fall in GFR, some considered histological pattern of acute cellular crescent formation with few using RIFLE or KDIGO guidelines. Duration of follow up has also revealed a variation from shortest of 32 weeks to longest 25 years (Table-I).
Variety of glomerular lesion seen in this meta-analysis. Some of studies addressing only one aspect of glomerular disease that is lupus nephritis,5,6,8,18,20,22,27 one study only addressed anti GBM disease,23 some addressing only acute glomerulonephritis,9,10 isolated AAV in two,7,21 Crescentic GN in two,16,26 PIGN in two19,25 and rest of studies had mixed causes for glomerular lesions including one or more one of above.7,11,12,15,24 The largest population study included in current meta-analysis15 was actually comprised of all biopsied cases over a median follow up of 90 months and addressed the outcome for those who developed ESRF or died during follow-up period but complete renal recovery and number of CKD is not mentioned in this large cohort.
Another large study from China reporting study population of 528 patients with biopsy proven crescentic glomerulonephritis (GN), has shown variation in causes of GN, including AAV and anti-GBM disease, 58% of their studied population developed AKI, while another 13% they categorized as acute kidney disease (AKD). In this study worse prognosis was observed in anti-GBM disease related AKI.16 Moreover, study published in past from our center has also shown worst prognosis towards renal recovery from same type of GN, that is, anti-GBM disease.7 Dual positivity of ANCA and anti-GBM at same time is reported as occurring at older age, causing more severe renal damage and resulting in high mortality.7,16 Another study published from China, with smaller study cohort, using same definitions of histologic pattern and crescentic GN, also had AAV and anti-GBM positive patients, this particular study has not mentioned number of renal recovery but mortality rate was 9% in their studied population.10
Only prospective study in this meta-analysis, comprising of 100 patients was addressing infection related GN, where most common source (41%) of infection was skin and soft tissues. Histological pattern in this study was 63% diffuse proliferative GN, 22% endo-capillary proliferative GN, 8% crescentic GN with >50% glomeruli with crescents and another 28% having crescents in <50% glomeruli. In their studied population 3% died during acute illness, 34% remained CKD and 9% dialysis dependent (ESRF), 26 % had persistent hypertension, the follow up was six months in this particular study.19 Heterogeneity among mortality highlights the differences in stages of AKI at time of presentation and possible impact of immunosuppression (effect of this factor not analyzed) used in these patients.
Limitations:
Scarcity of studies published from region and discrepancies in way of defining and addressing the outcomes, as well as almost nonexistence of well-designed prospective cohorts were main limitations during this analysis. Heterogeneity with I2 of up to 98% is also a limitation towards setting down any hard core recommendation. However, heterogeneity was inevitable because these studies were reported from different centers of countries in Asia with varying type of set up of nephrology services and available facilities.
CONCLUSIONS
In conclusion; our analysis included more than 4,000 patients from 21 studies, reflecting major causes of AKI related to glomerular diseases in the region. All studies were observational with wide heterogeneity. This study provides a wide spectrum of glomerular diseases causing AKI, highlighting important disparities related to availability of nephrology care in different Asian countries which include both lower income and lower middle income countries. Future work in this field, in this region, should focus on designing prospective or randomized multicenter studies targeting standard definitions of AKI and proper documentation of events during management as well as follow up.
Authors contributions:
SA: Intern, Department of Nephrology, SIUT, did search independently through different search engines, entered and analyzed the results.
AAB and AAZ: Intern, Department of Nephrology, SIUT, did search independently through different search engines, entered the data, written introduction and results.
RN: Professor, Department of Nephrology, SIUT, given concept, guided through selection of articles, reviewed articles included in final analysis, written discussion and responsible for accuracy of study.
All authors have read and approved the final manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kellum JA Romagnani P Ashuntantang G Ronco C Zarbock A Anders HJ Acute kidney injury Nat Rev Dis Primers 20217117 doi:10.1038/s 41572-021-00284-z 3426722310.1038/s 41572-021-00284-z · doi ↗ · pubmed ↗
- 2Beaufils M Morel-Maroger L Sraer JD Kanfer A Kourilsky O Richet G Acute renal failure of glomerular origin during visceral abscesses New England J Med 19762954185189 doi:10.1056/NEJM 197607222950402127234710.1056/NEJM 197607222950402 · doi ↗ · pubmed ↗
- 3Naqvi R Epidemiological trends in community acquired acute Kidney Injury in Pakistan:25 years'Experience from a Tertiary Care Renal Unit Pak J Med Sci 2021372312319 doi:10.12669/pjms.37.2.38763367990510.12669/pjms.37.2.3876 PMC 7931297 · doi ↗ · pubmed ↗
- 4Yoo JJ Lee JH Yoon JH Lee M Lee DH Cho Y Hepatitis B Virus-Related Glomerulonephritis:Not a Predominant Cause of Proteinuria in Korean Patients with Chronic Hepatitis B Gastroenterol Res Pract 201520151126532 doi:10.1155/2015/1265322578894010.1155/2015/126532 PMC 4348579 · doi ↗ · pubmed ↗
- 5Koubar SH Kort J Kawtharani S Chaaya M Makki M Uthman I Characteristics of lupus and lupus nephritis at a tertiary care center in Lebanon Lupus 2019281315981603 doi:10.1177/0961203319≆593155445810.1177/0961203319877459 · doi ↗ · pubmed ↗
- 6Hari P Bagga A Mahajan P Dinda A Outcome of lupus nephritis in Indian children Lupus 2009184348354 doi:10.1177/09612033080975701927630310.1177/0961203308097570 · doi ↗ · pubmed ↗
- 7Naqvi R Mubarak M Ahmed E Akhtar F Bhatti S Naqvi A Spectrum of glomerular diseases causing acute kidney injury;25 years'experience from a single center J Renal Inj Prev 201544113116 doi:10.12861/jrip.2015.242669349710.12861/jrip.2015.24PMC 4685980 · doi ↗ · pubmed ↗
- 8Chan PC Wong WS Wong KL Cheng IK Chan MK Lupus nephritis patients on maintenance dialysis in Hong Kong Int J Artif Org 19891212782787 doi:10.1177/0391398889012012092613359 · pubmed ↗