Predictive factors of stigma in stroke patients based on logistic regression and decision tree mode
Wenwen Ma, Kunjuan Jing, Ruotong Zhang, Xuefei Li, Zheng Li

TL;DR
This study identifies factors that predict stigma in stroke patients using logistic regression and decision tree models.
Contribution
The study compares logistic regression and decision tree models for predicting stigma in stroke patients.
Findings
Threat assessment is a risk factor for stigma, while social support and resilience are protective factors.
The decision tree model identified psychological resilience as the most important factor affecting stigma.
Logistic regression had slightly higher AUC and accuracy than the decision tree model.
Abstract
Logistic regression and decision tree model were used to analyze the predictive factors of stigma in stroke patients, and to explore the application value of the two models. This was a retrospective study. The data of 342 stroke patients were collected from Baoding No.1 Central Hospital from December 2023 to March 2024. Data were retrospectively retrieved from the hospital information and management system. The regression model and decision tree model of influencing factors of stroke patients’ sense of stigma were established, to analyze the influencing factors of the sense of stigma, and to compare the predictive effects, advantages and disadvantages of the two models. Logistic regression analysis showed that threat assessment (OR=2.7761) was a risk factor for stigma, while irrelevant cognitive appraisal (OR=0.321), social support (OR=0.098) and resilience (OR=0.438) were protective…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
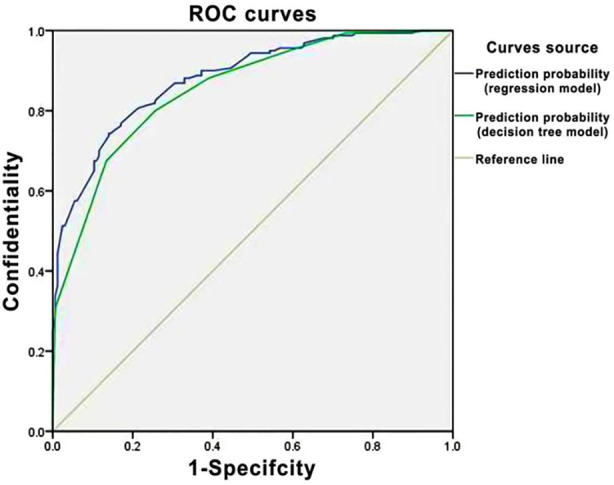 Fig.1
Fig.1| Item | Group | Low stigma risk group ( | High stigma risk group ( | 2 | P |
|---|---|---|---|---|---|
| Gender | Male | 95 (57.93) | 94 (58.75) | 0.023 | 0.881 |
| Female | 69 (42.07) | 66 (41.25) | |||
| Age (years) | <40 | 16 (9.76) | 9 (5.63) | 2.513 | 0.473 |
| 40~ | 59 (35.98) | 54 (33.75) | |||
| 60~ | 80 (48.78) | 88 (55.00) | |||
| ≥80 | 9 (5.49) | 9 (5.63) | |||
| Marital status | Married | 6 (3.66) | 2 (1.25) | 2.164 | 0.339 |
| Unmarried | 149 (90.85) | 147 (91.88) | |||
| Widowed | 9 (5.49) | 11 (6.88) | |||
| Educational level | Elementary school or below | 52 (31.71) | 54 (33.75) | 0.674 | 0.954 |
| Middle school | 54 (84.38) | 51 (31.88) | |||
| High school (Technical secondary school) | 38 (23.17) | 38 (23.75) | |||
| Junior college education or above | 31 (18.90) | 6 (3.75) | |||
| Work status | Unemployed | 20 (12.19) | 24 (15.00) | 3.647 | 0.456 |
| Employed | 27 (16.46) | 22 (13.75) | |||
| Retired | 43 (26.22) | 34 (21.25) | |||
| Engaged in agriculture | 74 (45.12) | 80 (50.00) | |||
| Family residence | Urban | 64 (39.02) | 68 (42.50) | 0.405 | 0.524 |
| Rural | 100 (60.98) | 92 (57.50) | |||
| Monthly family income per capita (Yuan) | <2000 | 76 (46.34) | 77 (48.13) | 10.350 | 0.016 |
| 2000~ | 65 (39.63) | 54 (33.75) | |||
| 4000~ | 16 (9.76) | 27 (16.88) | |||
| ≥6000 | 8 (4.88) | 1 (0.63) | |||
| Payment for medical expenses | Self-funded | 13 (7.93) | 6 (3.75) | 2.947 | 0.400 |
| Employee’s Medical Insurance | 56 (34.15) | 59 (36.88) | |||
| Urban Health Insurance (New Cooperative Medical Scheme) | 92 (56.09) | 95 (59.38) | |||
| Commercial insurance | 2 (1.22) | 1 (0.63) | |||
| Somatic dysfunction | Yes | 115 (70.12) | 74 (46.25) | 18.988 | 0.000 |
| No | 49 (29.88) | 86 (53.75) | |||
| Other chronic diseases | Yes | 116 (70.73) | 119 (74.38) | 0.540 | 0.463 |
| No | 48 (29.27) | 41 (25.63) | |||
| Self-care ability | Severe | 15 (9.15) | 2 (1.25) | 20.674 | 0.000 |
| Moderate | 105 (64.02) | 92 (57.50) | |||
| Mild | 44 (26.83) | 58 (36.25) | |||
| Not required | 0 (0) | 8 (5.00) | |||
| Duration of disease | <1 | 128 (78.05) | 122 (76.25) | 0.737 | 0.864 |
| 1~ | 9 (5.49) | 12 (7.50) | |||
| 3~ | 12 (7.32) | 10 (6.25) | |||
| ≥5 | 15 (9.15) | 16 (10.00) | |||
| Frequency of strokes | <1 | 113 (68.90) | 98 (61.25) | 3.303 | 0.192 |
| 2~ | 51 (31.09) | 62 (38.75) |
| Variables | x±s | Challenge | Threat | Harm | Irrelevant | Secondary appraisal | Psychological resilience | Social support | Confrontation | Avoidance | Submission | Stigma |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Challenge | 19.72±4.47 | 1 | -.553 | -.627 | .579 | .110 | .690 | .563 | .540 | -.375 | -.661 | -.637 |
| Threat | 15.92±3.73 | -.553 | 1 | .671 | -.439 | .074 | -.534 | -.405 | -.323 | .359 | .506 | .580 |
| Harm | 27.22±6.84 | -.627 | .671 | 1 | -.604 | .149 | -.637 | -.406 | -.333 | .447 | .542 | .707 |
| Irrelevant | 9.49±3.94 | .579 | -.439 | -.604 | 1 | .065 | .561 | .406 | .313 | -.348 | -.447 | -.569 |
| Secondary appraisal | 17.05±2.09 | .110 | .074 | .149 | .065 | 1 | -.008 | .081 | .078 | .073 | -.049 | .065 |
| Psychological resilience | 21.91±8.81 | .690 | -.534 | -.637 | .561 | -.008 | 1 | .595 | .499 | -.476 | -.617 | -.667 |
| Social support | 58.09±12.98 | .563 | -.405 | -.406 | .406 | .081 | .595 | 1 | .504 | -.275 | -.406 | -.507 |
| Confrontation | 17.23±4.79 | .540 | -.323 | -.333 | .313 | .078 | .499 | .504 | 1 | -.364 | -.527 | -.389 |
| Avoidance | 16.61±3.64 | -.375 | .359 | .447 | -.348 | .073 | -.476 | -.275 | -.364 | 1 | .445 | .462 |
| Submission | 9.28±4.12 | -.661 | .506 | .542 | -.447 | -.049 | -.617 | -.406 | -.527 | .445 | 1 | .546 |
| Stigma | 45.36±11.76 | -.637 | .580 | .707 | -.569 | .065 | -.667 | -.507 | -.389 | .462 | .546 | 1 |
| B | S.E. | Wald | df | Significance | Exp (B) | 95% confidence interval of Exp (B) | ||
|---|---|---|---|---|---|---|---|---|
| Lower limit | Upper limit | |||||||
| Dysfunction | -.305 | .335 | .828 | 1 | .363 | .737 | .382 | 1.422 |
| Self-care ability 1 | -19.924 | 12237.898 | .000 | 1 | .999 | .000 | .000 | . |
| Self-care ability 2 | -19.849 | 12237.898 | .000 | 1 | .999 | .000 | .000 | . |
| Self-care ability 3 | -20.604 | 12237.898 | .000 | 1 | .999 | .000 | .000 | . |
| Threat | 1.021 | .392 | 6.790 | 1 | .009 | 2.776 | 1.288 | 5.982 |
| Challenge | -1.088 | .685 | 2.520 | 1 | .112 | .337 | .088 | 1.291 |
| Harm | .810 | .474 | 2.924 | 1 | .087 | 2.247 | .888 | 5.684 |
| Irrelevant | -1.137 | .314 | 13.089 | 1 | .000 | .321 | .173 | .594 |
| Social support | -2.319 | .726 | 10.199 | 1 | .001 | .098 | .024 | .408 |
| Avoidance | 1.075 | .787 | 1.865 | 1 | .172 | 2.929 | .627 | 13.697 |
| Submission | -19.345 | 10436.874 | .000 | 1 | .999 | .000 | .000 | . |
| Psychological resilience | -.825 | .317 | 6.776 | 1 | .009 | .438 | .236 | .816 |
| Constant | 40.832 | 16083.977 | .000 | 1 | .998 | 5406E+17 | ||
| Model | AUC | SD | P | 95%CI | Accuracy (%) |
|---|---|---|---|---|---|
| Logistic regression model | 0.880 | 0.018 | 0.000 | 0.844-0.916 | 79.6 |
| Decision tree model | 0.854 | 0.020 | 0.000 | 0.814-0.894 | 78.7 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStroke Rehabilitation and Recovery · Advanced Technologies in Various Fields · Acute Ischemic Stroke Management
INTRODUCTION
Stroke with a disability rate as high as 75%.1 While the disease puts them in a certain degree of stigma. A study reveal that stigma is prevalent in stroke patients.2 Cognitive appraisal refers to the cognitive process by which an individual realizes the impact of a stressful event on his or her health.3 Social support is a key factor in determining the relationship between psychological stress and health.4 Social support works with internal factors such as coping styles to influence the individual’s mental health.5 A study revealed that stroke patients with greater access to social support had lower levels of stigma6, some studies have shown a strong correlation between coping styles and stigma.7 Psychological resilience refers to the process of positive adjustment by an individual to achieve physical and mental balance in the face of unfavorable or potentially traumatic events.8 Psychological resilience has been found to be associated negatively with stigma. This study used the stress and coped model as a framework, we explored the influencing factors of stigma in stroke patients from a psycho-cognitive perspective based on Logistic regression and decision tree model.
METHODS
This was a retrospective study. Data from 342 hospitalized stroke patients collected in Baoding No.1 Central Hospital from December 2023 to March 2024 were used. Data were retrospectively retrieved from the hospital information and management system. Collected their various information of all patients, including age, gender, marital status, education level, work status, family residence, monthly family income per capita, payment for medical expenses, frequency of strokes, duration of disease, presence of somatic dysfunction, etc.
Ethics approval:
The study was approved by the Institutional Ethics Committee of Baoding No.1 Central Hospital (No.: 2023095; date: October 23, 2023), and written informed consent was obtained from all participants.
The Cognitive Appraisal of Health Scale:
A self-assessment scale to measure stroke patients’ cognitive appraisal of stroke events.9 In this study, Cronbach’s α coefficients were 0.75 for threat, 0.82 for challenge, 0.83 for beneficial/irrelevant, and 0.85 for harm/loss. The higher the score, the more inclined the individual is to appraise the event of having a stroke by this appraisal scale.
Connor-Davidson Resilience Scale (CD-RISC-10):
A simplified version of the 10 items psychological resilience scale (CD-RISC-10).10,11 The higher the score, the better the individual’s psychological resilience.12 The Cronbach’s α coefficient was 0.94.
Perceived Social Support Scale (PSSS):
To measure the perceived social support and level of family, friends and other people in stroke patients.13,14 The higher the score, the more social support is subjectively perceived by the individual. The total Cronbach’s α coefficient was 0.94.
Medical Coping Modes Questionnaire:
To mainly assess the coping styles adopted by stroke patients when facing the disease.15 The Chinese version includes 20 items in three dimensions.16 With higher scores suggesting greater use of the corresponding coping style. The Cronbach’s α coefficients of this study were 0.793 for confrontation, 0.52 for avoidance, and 0.844 for submission.
Stroke Stigma Scale:
To measure the level of stroke patients’ stigma.17 The higher the score, the greater the degree of stigma. The total Cronbach’s α coefficient was 0.880.
Statistical analysis:
All data analyzed using the SPSS 25.0 software. The confidence interval was 95%. General data were expressed as the number of cases and percentages, and the chi-square test was used for comparison between groups. P-value<0.05 indicated a statistically significant difference. Pearson’s correlation analysis was taken for the correlation of influencing factors.
Analysis of influencing factors:
The Logistic regression model and CART decision tree model were established to analyze the influencing factors of stigma, with stigma as the dependent variable and statistically significant general data, cognitive evaluation, coping style, psychological resilience and social support in the univariate analysis as the independent variables. The prediction efficiency of the two models was compared.
RESULTS
The average age of the included 324 patients was 60.22±12.95 years old, of which 189 were male and 135 were female. The stigma score of stroke patients was (44.92±11.68) with a median of 46. The median stigma score was used to categorize the patients into two groups: high stigma risk group (≤46, assigned a value of 0) (160 cases, 49.4%) and low stigma risk group (>46, assigned a value of one) (164 cases, 50.6%). The results showed that the monthly family income per capita, dysfunction and self-care ability were statistically significant (P<0.05), Table-I.
Pearson’s correlation analysis showed that there was a statistically significant relationship between stigma and the influencing factors, Table-II. Logistic regression analysis results showed that patients with threat cognitive appraisal was risk factors for irrelevant cognitive appraisal, social support and psychological resilience, Table-III. Hosmer-lemeshow goodness-of-fit test X2=1.917, df=3, P=0.590, demonstrating good model fit.
The decision tree model results showed that 160 were at risk of high stigma, with an incidence of 49.4%. The most important independent variable affecting the decision tree target variable (stigma) was psychological resilience. When the score was ≤22, the incidence of high stigma risk was 73.3%. When the psychological resilience score was ≤22 and social support ≤61, the incidence of high stigma risk was 98%; When the psychological resilience score was ≤22, along with social support >61 and irrelevant cognitive appraisal ≤9, the incidence of high stigma risk was 73.8%. When the psychological resilience score was >22, along with threat cognitive appraisal >16 and irrelevant cognitive appraisal ≤9, the risk of high stigma was 50.0%.
The ROC curves of the two models were plotted. Fig.1 and the AUC was calculated, as shown in Table-IV. The results showed that the AUC of the decision tree model and the Logistic regression model were 0.854 and 0.880, and the accuracy respectively was 78.7% and 79.6%.
ROC curve.
DISCUSSION
Logistic regression analysis reveals a positive correlation between stigma and threat cognitive appraisal and a negative correlation with irrelevant cognitive appraisal in stroke patients. It indicates that threat cognitive appraisal is a risk factor for stigma in stroke patients and irrelevant cognitive appraisal is a protective factor. This is similar to the findings of national and international studies.18 Cognitive appraisal including primary appraisal, secondary appraisal and reappraisal. The primary appraisal is an appraisal of the event or situation itself, Secondary appraisal is mainly an appraisal of coping styles, coping resources, and so on. Reappraisal is an appraisal of the effectiveness and adaptability of one’s emotional and behavioral responses.3
The decision tree model shows that threat cognitive appraisal mediates the relationship between psychological resilience and stigma, through which patients’ stigma is reduced instead, suggesting a protective effect. This is in contrast to the results of the logistic regression analysis. The irrelevant cognitive appraisal is a diminished effect on stigmas compared to threat cognitive appraisal. It indicates that irrelevant cognitive appraisal mediates the relationship between social support and stigma, and that higher scores on irrelevant cognitive appraisal are associated with a lower incidence of stigma. Irrelevant cognitive appraisal is a protective factor for stigma.
The Logistic regression model and decision tree model illustrated that threat and irrelevant cognitive appraisals are predictors of stigma in stroke patients. It has been found that stigma is positively correlated with negative emotions, which exacerbates patients’ stigma by preventing them from fully understanding their illness and fearing the prognosis.19 Accordingly, patients’ health cognition should be understood in nursing care, and their positive cognition should be mobilized while their negative cognition should be minimized; at the same time, patients should be educated to accept the reality of suffering from a stroke event frankly, to enhance their confidence in overcoming the disease, and to alleviate their sense of stigma.
The Logistic regression analysis reveals a negative correlation between psychological resilience and stigma. The decision tree model shows that the influence of psychological resilience on stigma is located at the first tier of the decision tree, which indicates that psychological resilience is an important protective factor for stigma. A study found that psychological resilience in stroke patients was negatively correlated with negative emotions such as anxiety and depression.20 These studies have affirmed the important role played by patients’ psychological resilience during disease regression. Therefore, caregivers should analyze the psychological resilience level and characteristics of stroke patients, improve their psychological resilience level and promote their adaptation to stroke events, so as to promote their recovery. Logistic regression analysis reveals a negative correlation between social support and stigma, this is consistent with the findings of Ge C.2
The Logistic regression model and decision tree model have shown that social support is a major protective factor for stigma in stroke patients. Therefore, patients should be encouraged to actively seek social support networks in nursing care, while nursing workers should actively mobilize patients’ family members, friends and other people to care for, support and encourage patients, so as to improve their confidence in overcoming the disease and reduce their negative emotions of stigma. The decision tree model shows that dysfunction also has an effect on stigma, but it is not included in the Logistic regression analysis, suggesting that dysfunction has a weaker effect on stigma.
In the comparison of the two models, it is found that the Logistic regression model emphasizes more on the dependence between different influencing factors and stigma, it has higher accuracy and stability. But the decision tree model capable of visualizing and categorizing the influencing factors, providing a more reliable basis for targeted interventions.
Limitations:
However, regression models and decision tree models are not included in the coping styles in this study, which may be related to the sample size or a single source of the sample. For this reason, the sample size needs to be enlarged and multicenter sampling should be adopted in future studies to make the results more reliable.
CONCLUSIONS
The two models have their own advantages, combination of the advantages of the two models may be used while considering one of the higher accuracies of the two, in order to provide a new idea for the screening of predictors of stigma in stroke patients.
Authors’ Contributions:
WM and KJ carried out the studies, data collection, drafted the manuscript, and are responsible and accountable for the accuracy or integrity of the work.
RZ and XL: Literature search, performed the statistical analysis and participated in its design.
ZL performed the statistical analysis, participated in its design. Critical Review.
All authors have read and approved the final manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wang HL Li YL Li XF Wang ZZ The value of serum procalcitonin in the anti-infection therapy of acute stroke patients Pak J Med Sci 202137411551160 doi:10.12669/pjms.37.4.39323429080010.12669/pjms.37.4.3932 PMC 8281182 · doi ↗ · pubmed ↗
- 2Ge C Zhang H Zhu G Cao A Zhang J Intervention study of Snyder's hope theory on the stigma of stroke in young and middle-aged patients:a randomised trial Ann Palliat Med 202110557215728 doi:10.21037/apm-21-4413397774310.21037/apm-21-441 · doi ↗ · pubmed ↗
- 3Nott M Wiseman L Seymour T Pike S Cuming T Wall G Stroke self-management and the role of self-efficacy Disabil Rehabil 2021431014101419 doi:10.1080/09638288.2019.16664313156023010.1080/09638288.2019.1666431 · doi ↗ · pubmed ↗
- 4Pollock A Campbell P Cheyne J Cowie J Davis B Mc Callum J Interventions to support the resilience and mental health of frontline health and social care professionals during and after a disease outbreak, epidemic or pandemic:a mixed methods systematic review Cochrane Database Syst Rev 20201111 CD 013779 doi:10.1002/14651858.CD 0137793315097010.1002/14651858.CD 013779 PMC 8226433 · doi ↗ · pubmed ↗
- 5Salve J Pate S Debnath K Langade D Adaptogenic and Anxiolytic Effects of Ashwagandha Root Extract in Healthy Adults:A Double-blind, Randomized, Placebo-controlled Clinical Study Cureus 20191112 e 6466 doi:10.7759/cureus.64663202173510.7759/cureus.6466 PMC 6979308 · doi ↗ · pubmed ↗
- 6Lin FH Yih DN Shih FM Chu CM Effect of social support and health education on depression scale scores of chronic stroke patients Medicine (Baltimore)20199844 e 17667 doi:10.1097/MD.00000000000176673168978010.1097/MD.0000000000017667 PMC 6946326 · doi ↗ · pubmed ↗
- 7Mantzoukas S Kotrotsiou S Mentis M Paschou A Diamantopoulos E Kotrotsiou E Exploring the Impact of Shame on Health-Related Quality of Life in Older Individuals J Nurs Scholarsh 2021534439448 doi:10.1111/jnu.126633387060210.1111/jnu.12663 · doi ↗ · pubmed ↗
- 8ZábóV Csiszar A Ungvari Z Purebl G Psychological resilience and competence:key promoters of successful aging and flourishing in late life Geroscience 202345530453058 doi:10.1007/s 11357-023-00856-93741809810.1007/s 11357-023-00856-9PMC 10643728 · doi ↗ · pubmed ↗