Bladder Metastasis From Lung Adenocarcinoma: A Rare Case
Nicola Fazaa, Etan Eigner, Inbal Farkash, Gilad Amiel, Azik Hoffman

TL;DR
A rare case of lung cancer spreading to the bladder is reported, emphasizing the need for accurate diagnosis to avoid misidentification as bladder cancer.
Contribution
This paper presents a rare clinical case of bladder metastasis from lung adenocarcinoma and underscores diagnostic considerations.
Findings
Bladder metastasis from lung adenocarcinoma is rare and often misdiagnosed as primary bladder cancer.
Histopathology and immunohistochemistry confirmed metastasis with TTF-1+/CK7+/CK20-/GATA3- profile.
The case highlights the importance of considering metastasis in patients with advanced cancer and new urinary symptoms.
Abstract
Bladder metastasis from primary lung adenocarcinoma is an infrequent clinical entity. Due to its rarity and nonspecific presentation, it is often misdiagnosed as primary urothelial carcinoma. We report the case of a 65-year-old male with a history of metastatic lung adenocarcinoma presenting to the emergency room with sudden gross hematuria. Imaging revealed a new bladder lesion. Following transurethral resection, histopathological and immunohistochemical analysis confirmed metastatic lung adenocarcinoma (thyroid transcription factor-1-positive/cytokeratin 7-positive/cytokeratin 20 negative/GATA binding protein 3-negative or TTF-1+/CK7+/CK20-/GATA3-). The case was discussed at the Genitourinary Oncology Tumor Board, and given the prognosis of metastatic lung adenocarcinoma, the patient opted for palliative care. This case highlights the importance of considering metastatic spread to the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
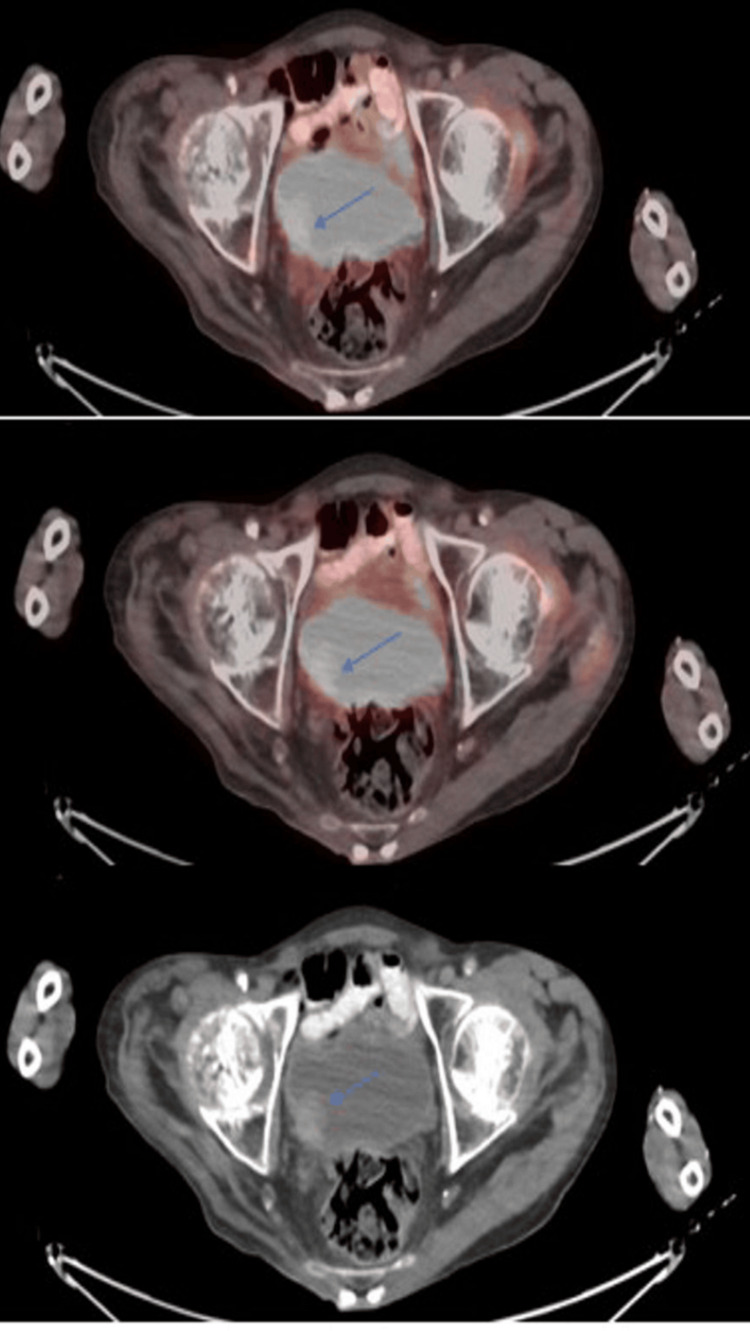 Figure 1
Figure 1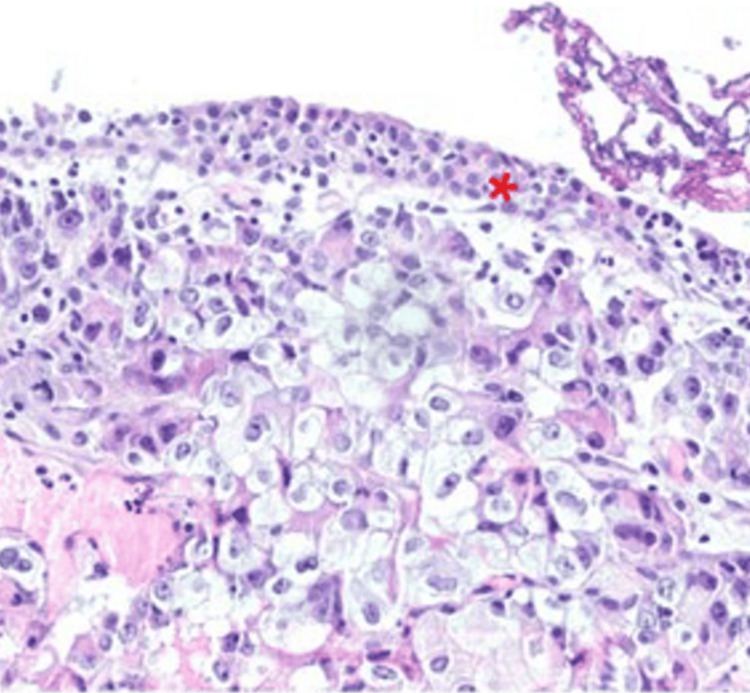 Figure 2
Figure 2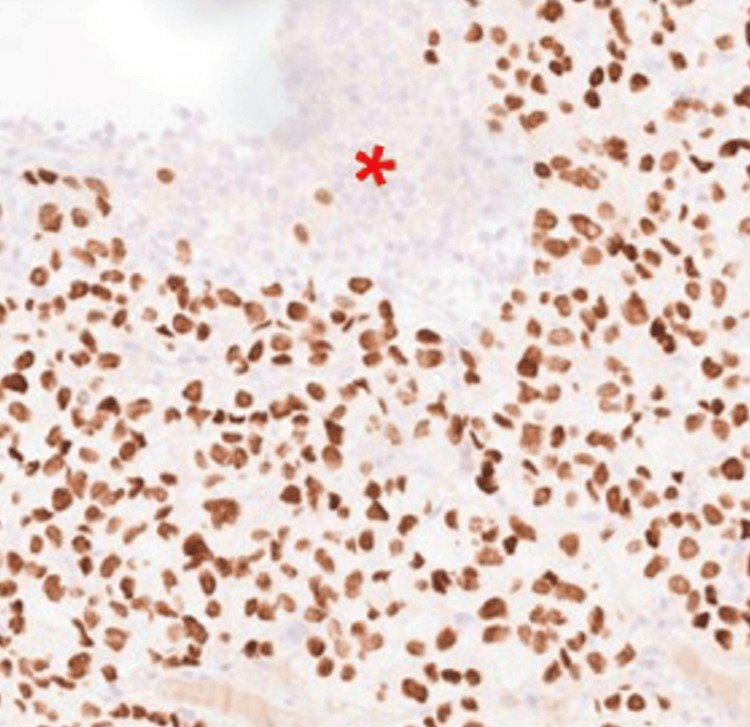 Figure 3
Figure 3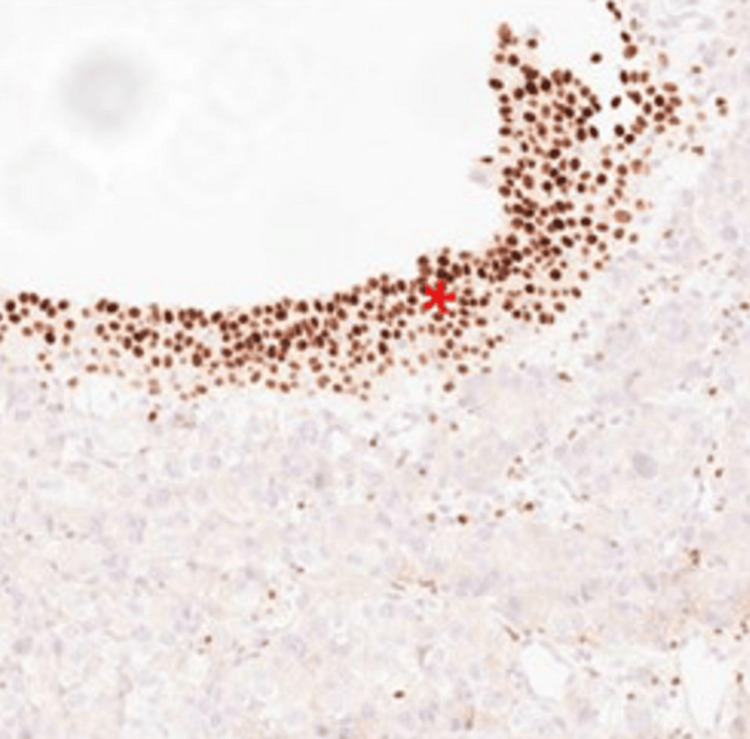 Figure 4
Figure 4| Age | Sex | Clinical presentation | Findings from cystoscopy | Immunohistochemistry and genetic marker results | Reference |
| 52 | M | Microscopic hematuria, dysuria | Tumor located at the apex of the bladder | CK-7(+), TTF-1(+), CK-20(-) | [ |
| 61 | M | Hydronephrosis | Thickened bladder wall | EGFR19(+), T790M(-) | [ |
| 63 | F | Arthralgia | Solid lesion measuring 3cm on the left side of the bladder wall | CK7(+), S100P(+), CK20(-), GATA3(+), CDX-2(-), TTF-1(-), NapsinA(-) | [ |
| 81 | F | Abdominal pain | Normal mucosal appearance with external compression | TTF-1(-), CK7(+), NapsinA(+) | [ |
| 83 | M | Gross hematuria | Bladder diverticulum observed in the right posterior wall | CK20(-), CK7(+), TTF-1(+), PSA(-), AR(-) | [ |
| 55 | M | Lower urinary tract symptoms (LUTS) | Involvement of the trigone and right lateral bladder wall | CK7(+), TTF1(+), CK20(-), PSA(-) | [ |
| 78 | M | Gross hematuria | 3mm papillary tumor, right lateral wall | TTF-1(+), CK-7(+), CK-20(-) | [ |
| 65 | F | Gross hematuria | Numerous solid lesions within the bladder | TTF-1(+), CK7(+), CK20(-), CD15(-) | [ |
| 53 | M | Hematuria | Normal mucosal lining with invasion of the detrusor muscle | TTF-1(+), CK-7(+), CK-20(-) | [ |
| 71 | M | Hematuria | Involvement along the urinary tract without muscle invasion | CK-7(+), TTF-1(+), NapsinA(+), CK20(-), PSA(-), P504S(-) | [ |
| 86 | F | LUTS | Nodular lesion with calcified areas in the left bladder wall | TTF-1(+), CK7(+), CK20(-), napsinA(-), p53(+), GATA3(+), Uroplakin III(-) | [ |
| 40 | M | Hematuria | Not specified | TTF-1(+), CK7(+), CK20(+) | [ |
| 72 | F | Gross hematuria | Space-occupying lesions | CK7(+), TTF-1(+), NapsinA(+), CK20(+), GATA3(-), CR(-), CD163(-), PAX-8(-). | [ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary and Genital Oncology Studies · Urological Disorders and Treatments · Bladder and Urothelial Cancer Treatments
Introduction
Lung adenocarcinoma is the most common histological subtype of lung cancer and is known for its ability to metastasize to various organs, including the liver, bones, adrenal glands, and brain [1]. Bladder metastasis from lung adenocarcinoma is exceptionally rare, with fewer than 15 cases reported over the past two decades [2]. The mechanism of metastasis to the bladder is not well understood, but hematogenous and lymphatic dissemination have been proposed as possible pathways [3]. Most bladder metastases from lung cancer present with hematuria, which is often initially mistaken for primary urothelial carcinoma, leading to diagnostic challenges [2]. In this report, we present a case of bladder metastasis from lung adenocarcinoma and discuss its clinical, histopathological, and immunohistochemical features in the context of the available literature.
Case presentation
A 65-year-old male, with a significant smoking history (60 pack-years), was diagnosed with lung adenocarcinoma with metastases to the adrenal glands, bones, and lymph nodes. The patient underwent palliative radiation therapy to the right knee, followed by a right above-knee amputation. He was subsequently treated by systemic immunotherapy with pembrolizumab. Three months later, during a revision surgery for his amputation, the patient developed gross hematuria. A three-way catheter was placed to facilitate continuous bladder irrigation.
A repeat PET-CT scan one month later identified a 2-cm space-occupying lesion located on the right bladder wall (Figure 1), which had not been seen on a prior CT scan a few months ago. Four weeks later, the patient underwent transurethral resection of the bladder tumor (TURBT), during which a 3 cm solid mass was resected from the right bladder wall. Concurrently, a transurethral resection of the prostate (TURP) was performed to facilitate a trial without a catheter, which was successful.
Focal hypermetabolic mass in the urinary bladder on PET-CT.
The histopathological examination demonstrated infiltration of the urothelium, lamina propria, and muscularis propria by malignant cells. Hematoxylin and eosin (H&E) staining (Figure 2) revealed an atypical cellular infiltrate beneath the urothelial surface.
Carcinoma infiltrates the lamina propria beneath the benign urothelium.
Immunohistochemical analysis showed strong nuclear uptake for thyroid transcription factor-1 (TTF-1) (Figure 3) and positivity for cytokeratin 7 (CK7), while cytokeratin 20 (CK20) and GATA3 staining (Figure 4) were negative. This immunophenotypic profile (TTF-1+/CK7+/CK20-/GATA3-) is inconsistent with primary urothelial carcinoma and instead strongly supports a diagnosis of metastatic lung adenocarcinoma involving the bladder wall.
TTF-1 positive carcinoma cells in contrast with the negative benign urothelium.
GATA3 positive in the benign urothelium. The carcinoma cells are negative for GATA3.
Following the confirmation of metastatic lung adenocarcinoma involving the bladder based on histopathological and immunohistochemical findings, the case was presented to the multidisciplinary Genitourinary Oncology Tumor Board. Given the patient's overall disease burden, as seen in whole-body imaging, and the prognosis associated with metastatic lung adenocarcinoma, he was referred back to his primary oncologist to discuss potential treatment options. After a comprehensive review of therapeutic strategies, including systemic therapy, the patient opted for palliative care, prioritizing symptom management and quality of life.
Discussion
Bladder metastases from lung adenocarcinoma are exceptionally rare, with fewer than 15 cases documented over the past two decades [2]. Patients typically present with hematuria, which can easily be misinterpreted as indicative of primary urothelial carcinoma [4], especially since smoking is a common risk factor for both bladder and lung carcinomas. This underscores the imperative for meticulous histopathological and immunohistochemical evaluations to achieve accurate diagnosis.
Metastases from distant primary tumors represent less than 2% of bladder cancers. Primary tumor locations with bladder metastases described in the literature are stomach, melanoma, breast, and lung [5,6]. The appearance of these tumors on cystoscopy could be variable and sometimes nonspecific and may look similar to other primary and secondary bladder tumors [3]. Table 1 provides a comprehensive overview of reported cases of lung adenocarcinoma presenting as a metastatic lesion in the bladder.
Immunohistochemistry plays a pivotal role in differentiating primary bladder tumors from metastatic lesions. Markers such as TTF-1 and CK7 are commonly expressed in lung adenocarcinomas, whereas CK20 and GATA3 are typically negative [5,7]. This immune profile aids in distinguishing metastatic lung adenocarcinoma from primary bladder adenocarcinoma and other malignancies [8].
The prognosis for patients with bladder metastasis from lung adenocarcinoma is generally poor, reflecting the aggressive nature of the primary disease and most often the presence of widespread metastases. Treatment strategies are primarily palliative, focusing on systemic chemotherapy tailored to the primary lung cancer. Localized treatments, such as transurethral resection or radiation therapy, may be offered to alleviate symptoms such as hematuria, but do not significantly improve overall survival [2,5].
A comprehensive review of the literature reveals that bladder metastases from lung adenocarcinoma often occur in the context of disseminated disease. For instance, Liu et al. described a 55-year-old patient with lung adenocarcinoma who developed bladder metastasis, highlighting the aggressive progression of the disease [2]. Similarly, other studies have documented cases in which bladder metastasis was detected as part of a widespread metastatic spread, further emphasizing the need for systemic therapeutic approaches [4,5,7].
This case contributes to the limited body of literature on this rare phenomenon, emphasizing the necessity to highlight this possible spread pattern, improve clinical awareness, and prevent misdiagnosis. Given that lung cancer remains a leading cause of cancer-related mortality, the possibility of atypical metastatic patterns should always be considered in patients with unusual presentations.
Conclusions
This case highlights the importance of considering metastatic disease in patients with a known primary malignancy who develop new urinary symptoms, such as hematuria. Accurate diagnosis through histopathological and immunohistochemical analysis is essential to guide proper management and avoid unnecessary interventions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Metastatic sites and survival in lung cancer Lung Cancer Riihimäki M Hemminki A Fallah M Thomsen H Sundquist K Sundquist J Hemminki K 78848620142513008310.1016/j.lungcan.2014.07.020 · doi ↗ · pubmed ↗
- 2Lung adenocarcinoma with bladder metastasis: a case report and literature review Front Oncol Liu Y Dong X Li T Xing Y Liu N 12028851320233747638310.3389/fonc.2023.1202885 PMC 10354362 · doi ↗ · pubmed ↗
- 3Bladder metastasis from lung adenocarcinoma: a difficult differential diagnosis with primary bladder adenocarcinoma World J Surg Oncol Cormio L Sanguedolce F Di Fino G Massenio P Liuzzi G Bufo P Carrieri G 901220142471673210.1186/1477-7819-12-90PMC 3984282 · doi ↗ · pubmed ↗
- 4Bladder metastases from lung cancer: clinical and pathological implications: a systematic review Oncology Sanguedolce F Loizzi D Sollitto F 1251349220172805645610.1159/000454731 · doi ↗ · pubmed ↗
- 5Isolated bladder metastasis from lung adenocarcinoma: a case report J Surg Case Rep Zaghbib S Chakroun M Saadi A 02021202110.1093/jscr/rjab 195PMC 815919434055288 · doi ↗ · pubmed ↗
- 6[A case of secondary bladder tumor the origin (gastric cancer) of which could not be identified before autopsy]Hinyokika Kiyo Mizutani Y Hashimura T Kitayama T Toshimitsu T Nonomura M 605608361990 https://pubmed.ncbi.nlm.nih.gov/2169186/2169186 · pubmed ↗
- 7A case of metastatic lung adenocarcinoma of the bladder in a patient with no documented history of lung cancer Urol Case Rep Azaiza M Yallapragada S Siegert J Andros G 1024414920233728831810.1016/j.eucr.2023.102441 PMC 10242483 · doi ↗ · pubmed ↗
- 8The use of placental S 100 (S 100P), GATA 3 and napsin A in the differential diagnosis of primary adenocarcinoma of the bladder and bladder metastasis from adenocarcinoma of the lung Pathologica Raspollini MR Comin CE Crisci A Chilosi M 33351022010 https://pubmed.ncbi.nlm.nih.gov/20731252/20731252 · pubmed ↗