Comparison between pipeline embolization device (PED) versus flow redirection endoluminal device (FRED) for intracranial aneurysms: a comprehensive systematic review and meta-analysis
Seyed Farzad Maroufi, Mohammad Sadegh Fallahi, Muhammad Waqas, Othman Bin-Alamer, Manisha Koneru, Joanna M Roy, Jane Khalife, Hamza A. Shaikh, Daniel A. Tonetti

TL;DR
This study compares two devices for treating brain aneurysms and finds they are similarly effective and safe.
Contribution
A comprehensive meta-analysis comparing the efficacy and safety of PED and FRED for intracranial aneurysms.
Findings
PED and FRED show comparable angiographic outcomes and complication rates.
FRED shows a trend toward lower retreatment rates but not statistically significant.
Adjunctive coiling is more frequently used with FRED.
Abstract
The performance of the Pipeline Embolization Device (PED) and relatively newer double-layered Flow Re-Direction Endoluminal Device (FRED) have been studied for the treatment of intracranial aneurysms, but direct comparisons between PED and FRED are limited. The current systematic review aims at comparing the efficacy and safety of PED and FRED. A systematic review of the literature was conducted according to the PRISMA guideline. PubMed, Embase, Scopus, Web of Science, and Cochrane Library were searched, and related records were identified. A meta-analysis of double-arm studies comparing PED and FRED was conducted on angiographic and clinical outcomes, retreatment rates, and complications following treatment. A total of 15 retrospective double-arm studies, published from 2017 to 2023, were included. Studies were predominantly from the US and Germany. A total of 2231 patients across…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
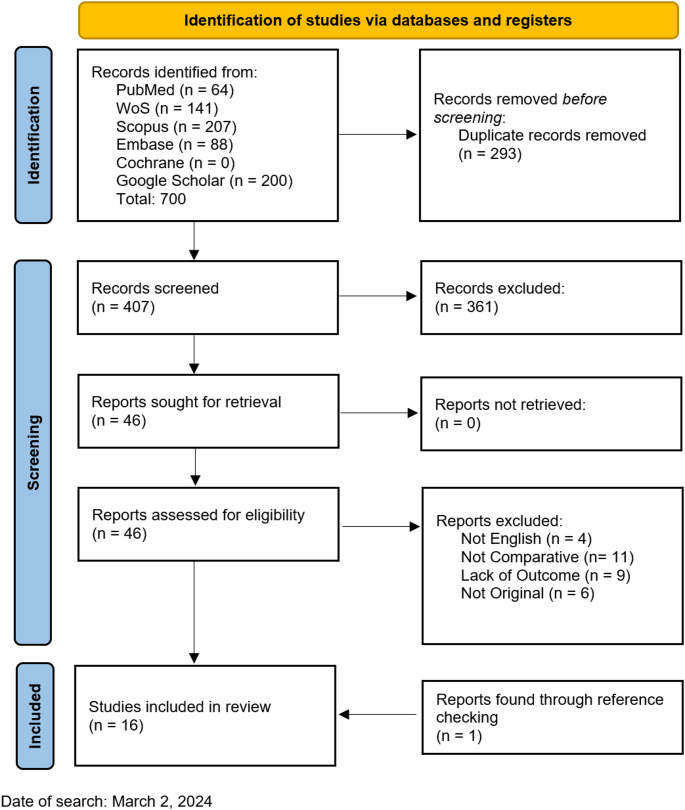 Figure 1
Figure 1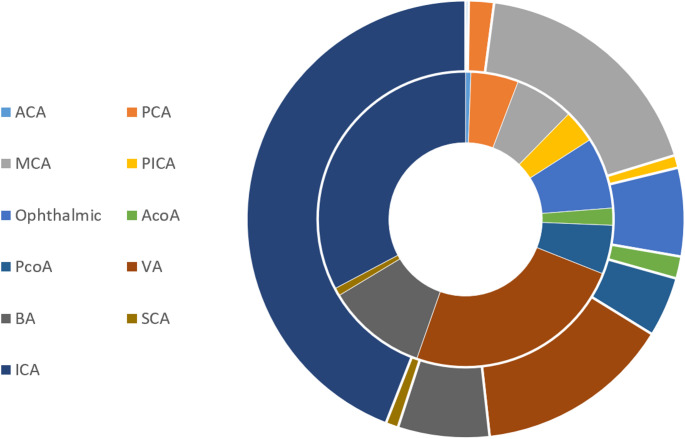 Figure 2
Figure 2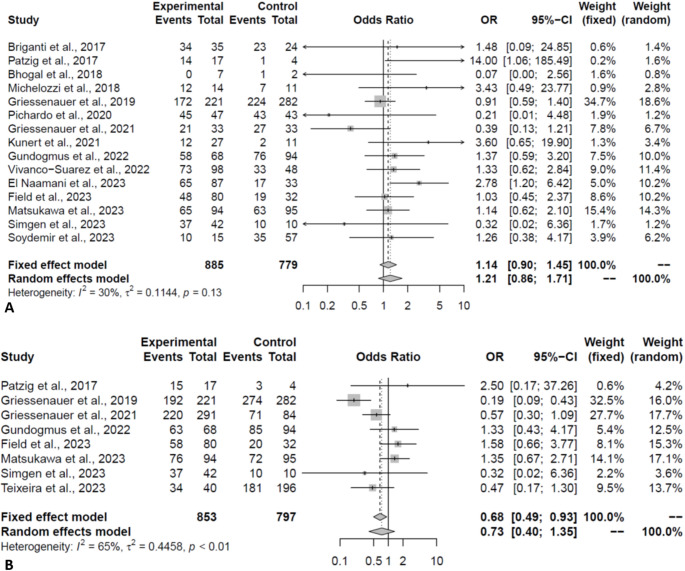 Figure 3
Figure 3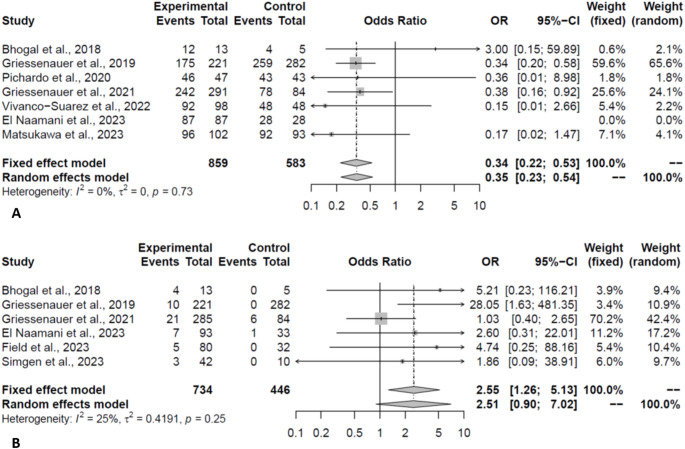 Figure 4
Figure 4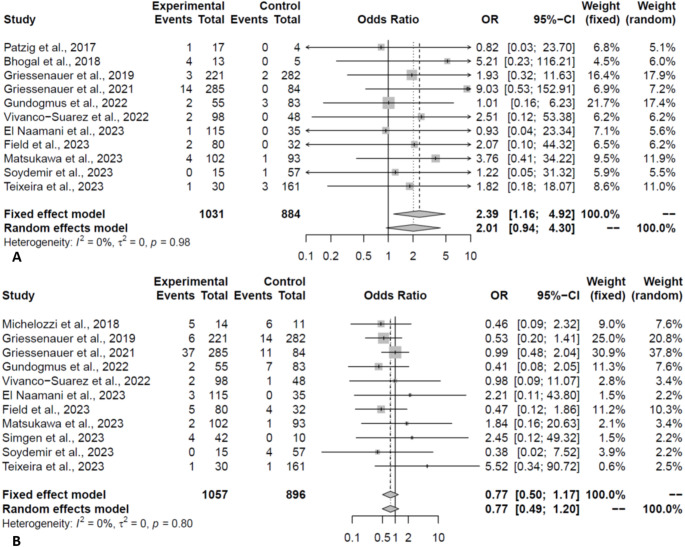 Figure 5
Figure 5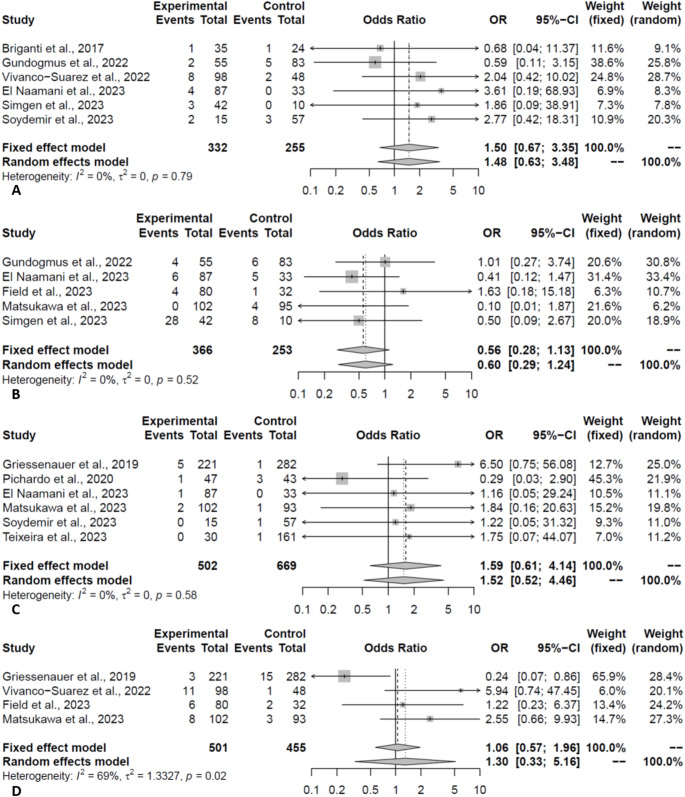 Figure 6
Figure 6 Figure 7
Figure 7- —Rowan University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntracranial Aneurysms: Treatment and Complications · Vascular Malformations Diagnosis and Treatment · Traumatic Brain Injury and Neurovascular Disturbances
Introduction
The Pipeline Embolization Device (PED) and the Flow Re-Direction Endoluminal Device (FRED) are both flow-diverting stents used in the endovascular treatment of intracranial aneurysms. By rerouting blood flow from the aneurysm sac, these devices promote thrombosis within aneurysm and reconstruction of the parent artery [1]. A number of sizable trials evaluating the safety and efficacy of PEDs have reported high occlusion rates and comparatively low complication rates [2, 3, 4]. The FRED is a newer-generation flow diverter (FD) with a dual-layer stent, consisting of an outer layer designed to divert blood flow and an inner layer to support the construct. Several multicenter experiences have reported acceptable occlusion rates and complication profiles for the FRED device [5, 6, 7]. While both devices aim to achieve similar outcomes, direct comparative studies between PED and FRED are limited. With the increasing number of available FDs, a pooled comparative report is paramount. This systematic review aims to provide a detailed, direct comparison of the performance and safety between these two FDs.
Materials and methods
The protocol of this review was not previously registered.
Search strategy
Embase, PubMed, Web of Science, Scopus, and Cochrane Library were searched on February 2024 according to PRISMA guideline, utilizing the following keywords and their equivalents “Pipeline Embolization Device” and “Flow Redirection Endoluminal Device”. A search was also performed on Google Scholar, and the top 200 most relevant results were reviewed. Additionally, a manual search of the bibliographies of the studies included was performed to discover any other pertinent studies.
Study selection
The inclusion criteria were as follows: (1) various types of clinical studies; (2) double-arm studies comparing the PED and FRED for intracranial aneurysms; (3) providing relevant outcomes such as occlusion, retreatment, complications, and neurological outcomes; and (4) written in English. The criteria for exclusion were: (1) case reports, reviews, letters, and editorials; and (2) studies that did not provide data on outcomes.
Data extraction
Information was extracted related to different variables, including patient characteristics, procedural specifics, angiographic and clinical outcomes, complications, and retreatment rates. When studies provided matched cohorts, they were categorized into distinct entries for additional analysis based on matching status. The primary outcomes included complete occlusion rates (defined as Raymond-Roy Occlusion Classification [RROC] grade 1, O’Kelly-Marotta [OKM] grade D, or Kamran et al. [8] grade 4), adequate occlusion rates (defined as RROC grade 2, OKM grade C, or Kamran et al. grade 3), and procedure-related complications. Complications analyzed included hemorrhagic events (spontaneous/delayed rupture, intracranial hemorrhage, hemorrhagic stroke, and systemic hemorrhage), thromboembolic events (ischemic stroke, transient ischemic attack, and intraoperative thrombus formation), procedural-related complication (deployment failure or microwire rupture), neurological complications, and in-stent stenosis.
Risk of bias assessment
The Risk of Bias in Non-Randomized Studies-of Interventions (ROBINS-I) was utilized by two impartial reviewers to assess the bias risk. Any discrepancies were resolved through involvement of a third reviewer.
Statistical analysis
All analyses were performed using the “meta” package in R (version 4.1.2). Due to the clinical and methodological variations among the studies, random-effect meta-analysis models were used. Median and range data were converted into mean and standard deviation, following Hozo et al. [9]. The functions “metabin” and “metacont” were used to derive effect estimates with the Mantel-Haenszel and DerSimonian-Laird methods [10]. Continuous data was presented using the mean difference, and categorical data was reported using the odds ratio (OR). Leave-one-out analysis was performed to gauge the influence of each study on the final effect. To assess heterogeneity and publication bias, meta-regressions and Egger regression were performed, respectively. A P-value < 0.05 was considered statistically significant.
Results
Study selection
A total of 700 articles were identified on initial search. 407 distinct records were left for abstract screening after duplicate removal, and 46 full-texts were selected for evaluation. Fifteen studies were deemed eligible and were included for analysis. One additional record was identified through reference checking (Fig. 1) [11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26].
Fig. 1. Flow diagram of the screening process
The included studies were retrospective cohorts published from 2017 to 2023 (Table 1). The most common countries of publications were the US and Germany, respectively. Three studies reported data on matched patients in addition to their main sample. Angiographic outcomes were evaluated using various scales across the included studies, with the OKM being the most commonly used scale (6 studies), followed by the RROC (5 studies) and Kamran et al. (2 studies).
Table 1. Characteristics of the included studiesAuthor/YearCountryStudy DurationFD TypeImaging TypeOcclusion CriteriaNo PatientsAgeFemaleFollow-UpLocationSaccularDevice TypeBhogal et al., 2018 [10]Argentina2009–2018PEDDSARROC1356.6161.5418.09ACA (3), PCA (3), PeriC (1), PICA (1), MCA (5)8PEDFRED555.210012ACA (1), PICA (1), MCA (3)5FREDJBriganti et al., 2017 [11]Italy2008–2015PEDDSA, MRA, CTAOKM315794.1250Paraophthalmic ICA (36), PcoA (14), Cavernous ICA (7), ACA (1), MCA (6), BA (2), PICA (1), SCA (2)67PEDFRED20FREDEl Naamani et al., 2023 [12]USA2018–2021PEDNRRROC11553.885.228.8Anterior Circulation (87)103PEDFRED3560.985.718.4Anterior Circulation (27)27FRED/FRED JrField et al., 2023 [13]USA2018–2022PEDNROKM8659.384.8820.6Anterior Circulation (74), Ophthalmic ICA (33.7%), MCA (11,6%), PcoA (25.6%), AcoA (9%)81PED/PED Flex/PED ShieldFRED3359.266.6712.4Anterior Circulation (27), Ophthalmic ICA (18.2%), MCA (11.6%), PcoA (18.2%), AcoA (9%)31FRED/FREDXGriessenauer et al., 2021 [14]USA, Canada, Austria, China, Germany, Turkey, Iran, Denmark2012–2019PEDDSA, CTANR2915750.5212VA (136), VBJ (19), BA (76), SCA (6), PICA (24), PCA (30)96PED FlexFRED84545024VA (46), VBJ (2), BA (22), SCA (4), PICA (3), PCA (7)34FREDGriessenauer et al., 2019 [15]USA, Austria, Turkey, Germany, Denmark,2013–2017PEDDSA, CTANR2216086.438.3Cavernous ICA (78), Paraophthalmic ICA (352), Other ICA (73)215PED/PED FlexFRED28254.578.0110.8257FREDGundogmus et al., 2022 [16]Turkey2012–2019PEDDSAOKM555085.4534Supraclinoid ICA (40), Cavernous ICA (15)55PEDFRED835286.7533Supraclinoid ICA (59), Cavernous ICA (24)52FREDKunert et al., 2021 [17]Poland2009–2016PEDDSAOKM27NRNRNROphthalmic ICA (27)NRPEDFRED11Ophthalmic ICA (11)FREDMatsukawa et al., 2023 [18]Japan2015–2022PEDDSA, MRA, CTARROC1036493.212.63ICA (102), PCA (2)96PEDFRED936175.2711.77ICA (71), PCA (1), MCA (2), VA (14), BA (7)74FREDMichelozzi et al., 2018 [19]France2010–2017PEDDSANR1518.57MCA (10), AcoA (5)NRPEDFRED1216.91MCA (8), AcoA (4)FRED/FREDJPatzig et al., 2017 [20]Germany2011–2013PEDDSAModified Kamran1756.2447.0629.67ICA (12), VA (5)NRNRFRED449.7510020.23ICA (4)Simgen et al., 2023 [21]Germany2010–2019PEDDSAKamran4251.880.9534.3ICA (39), VA (3)40NRFRED1051.16031.3ICA (10)10Soydemir et al., 2023 [22]Turkey2013–2019PEDDSAOKM1957.866.6724.7MCA73PEDFRED59MCAFRED/FREDJTeixeira et al., 2023 [23]Brazil2018–2022PEDDSAOKM40NRNRNRNRNRNRFRED196Vivanco-Suarez et al., 2022 [24]USA2015–2021PEDDSA, MRA, CTARROC926282.6114Anterior Circulation (99), Posterior Circulation (20)93PED/PED FlexFRED475085.1112Anterior Circulation (57), Posterior Circulation (5)42FREDPichardo et al., 2020 [25]Mexico2016–2019PEDDSARROC476155.3212PCOM (15), Ophthalmic ICA (7), Cavernous ICA (6), Anterior Choroidal (5), Hypophyseal ICA (3), Petrous ICA (4), VA (5), PCA (1), MCA (1)NRPEDFRED436155.8112PcoA (13), Ophthalmic ICA (11), Cavernous (9), Anterior Choroidal (4), Hypophyseal ICA (5), Petrous ICA (2)FREDNR: Not Reported; FD: Flow Diverter; PED: Pipeline Embolization Device; FRED: Flow Redirection Endoluminal Device; RROC: Raymond Roy Occlusion Classification; OKM: The O’Kelly-Marotta; DSA: Digital Subtraction Angiography; MRA: Magnetic Resonance Angiography, CTA: Computed Tomography Angiography; ACA: Anterior Cerebral Artery, PCA: Posterior Cerebral Artery, PeriC: Pericallosal Artery, PICA: Posterior Inferior Cerebellar Artery, MCA: Middle Cerebral Artery, PcoA: Posterior Communicating Artery, BA: Basilar Artery, SCA: Superior Cerebellar Artery, AcoA: Anterior Communicating Artery, VA: Vertebral Artery, VBJ: Vertebrobasilar Junction
Patients characteristics
A total of 2231 patients were identified across the included studies. 1214 patients (1276 aneurysms) were treated using PED and 1017 patients (1068 aneurysms) were treated with FRED. Patients in the PED group were slightly older than patients in the FRED group (57.42 vs. 55.54 years, P = 0.03). The majority of the patients were female in both groups (PED:77.75% vs. FRED:75.59%, P = 0.13). Only 2.05% and 0.27% of patients presented with ruptured aneurysms in the PED and FRED groups, respectively (P = 0.74). While the majority of aneurysms were saccular, the proportion was slightly higher in the PED group (86.25% vs. 80.52%, P = 0.03). More than 90% of the aneurysms were in the anterior circulation (PED:92.02% vs. FRED:96.12%, P = 0.96). In studies providing detailed data regarding aneurysm location, there were no significant differences between the two groups in the proportion of posterior cerebral (P = 0.33), middle cerebral (P = 0.27), ophthalmic (P = 0.73), vertebral (P = 0.96), and internal carotid artery (P = 0.56) locations (Fig. 2). Neck and aneurysm sizes were comparable between the two groups (P = 0.66, 0.18, respectively). 14.84% and 9.08% of patients received prior treatment in the PED and FRED groups, respectively (P = 0.20). Details of patients’ characteristics are reported in Table 2.
Fig. 2. Distribution of various aneurysm location for PED treated (inner circle) and FRED treated (outer circle) patients
Table 2. Meta-analytic details of baseline characteristics, outcomes, and adverse eventsVariableStPEDFREDEffect OR/MD P I^2HEager’s PAge, years1057.42 [55.56; 59.28]55.54 [54.00; 57.08]2.36 [0.28; 4.44]0.0389.13.03-Female, %1177.75 [67.64; 85.38]75.59 [66.21; 83.03]1.37 [0.91; 2.05]0.1350.51.42-Follow-Up, months1016.62 [14.41; 18.82]17.44 [12.76; 22.11]0.66 [-3.37; 4.68]0.7598.17.19-Rupture Presentation, %52.05 [0.39; 10.08]0.27 [0.01; 7.99]1.18 [0.44; 3.18]0.7456.71.52-Saccular Shape, %986.25 [72.30; 93.78]80.52 [64.28; 90.48]1.82 [1.07; 3.11]0.0362,71.64-Anterior Circulation, %892.02 [57.29; 99.00]96.12 [66.75; 99.67]1.02 [0.45; 2.33]0.9663.21.65-Neck Size, mm64.64 [3.46; 5.82]4.82 [3.89; 5.75]-0.14 [-0.75; 0.48]0.6688.82.99-Aneurysm Diameter, mm (SMD)127.91 [6.92; 8.90]7.01 [6.21; 7.81]0.28 [-0.13; 0.68]0.1893.03.77-Prior Treatment, %714.84 [7.67; 26.76]9.08 [6.93; 11.81]1.59 [0.78; 3.23]0.2071.01.86-Complete Occlusion, %1576.02 [64.31; 84.79]73.95 [58.41; 85.16]1.21 [0.86; 1.71]0.2730.51.200.79Matched Complete Occlusion, %471.78 [61.91; 79.92]78.36 [65.88; 87.17]0.79 [0.48; 1.29]0.350.001.00LSAdequate Occlusion, %883.46 [77.91; 87.84]88.46 [78.67; 94.09]0.73 [0.40; 1.35]0.3265.11.69LSMatched Adequate Occlusion, %381.61 [73.02; 87.92]92.71 [75.47; 98.13]0.49 [0.16; 1.47]0.2042.21.32LSResidual, %427.84 [3.54; 80.23]14.06 [7.48; 24.87]1.00 [0.28; 3.52]1.0023.11.14LSAdjunctive Coiling, %77.17 [3.58; 13.85]17.12 [10.20; 27.31]0.42 [0.18; 0.99]0.0471.81.88LSmRS < = 2, %793.96 [85.55; 97.61]97.70 [91.23; 99.43]0.35 [0.23; 0.54]< 0.010.001.00LSMatched mRS < = 2, %491.39 [77.31; 97.07]99.59 [57.29; 100]0.31 [0.12; 0.80]0.010.001.00LSComplications, %512.52 [7.22; 20.85]13.25 [5.44; 28.85]0.94 [0.44; 1.99]0.8641.31.31LSHemorrhage^#^, %113.12 [1.73; 5.57]1.13 [0.61; 2.09]2.01 [0.94; 4.30]0.070.001.000.68Thromboembolic Complication, %114.74 [2.54; 8.67]450 [1.74; 11.14]0.77 [0.49; 1.20]0.250.001.000.40In-Stent Stenosis, %56.52 [0.97; 33.11]12.11 [2.89; 39.01]0.60 [0.29; 1.24]0.170.001.00LSNeurological Complication, %61.79 [0.94; 3.41]1.02 [0.35; 2.95]1.52 [0.52; 4.46]0.450.001.00LSProcedural-Related Complication, %66.02 [3.92; 9.15]4.31 [2.40; 7.62]1.48 [0.63; 3.48]0.360.001.00LSRetreatment^^, %66.81 [5.20; 8.88]0.58 [0.04; 8.87]2.51 [0.90; 7.02]0.0825.01.16LSAdditional Treatment, %45.63 [2.63; 11.65]4.62 [3.03; 6.97]1.30 [0.33; 5.16]0.7168.51.78LSMortality, %31.48 [0.62; 3.50]0.79 [0.10; 6.02]1.21 [0.29; 5.02]0.800.001.00LS Significant on leave-one-out omitting Griessenauer et al., 2021 (P = 0.01); # Significant on leave-one-out omitting Gundogmus et al., 2022 (P = 0.04); mRS: Modified Rankin Scale; St: Number of studies; OR: Odds Ratio; MD: Mean Difference; SMD: Standardized Mean Diffrernece; LS: Limited number of studies
Clinical & angiographic outcomes
Outcomes are reported in Table 2. The complete occlusion rate was comparable between the two FDs (PED:76.02% vs. FRED:73.95%, OR:1.21, P = 0.27, Fig. 3A). The complete occlusion rates were still comparable when only pooling the matched studies (OR:0.79, P = 0.35). Similarly, the rate of adequate occlusion (occlusion with small neck/remnant) was comparable in pooling of all (PED:83.46% vs. FRED: 88.46%, OR:0.73, P = 0.32, Fig. 3B) and only matched studies (OR:0.49, P = 0.20). The residual aneurysm rate (> 50% filling) was comparable between the two groups (OR:1.00, P = 1.00). Based on the occlusion scales, the observed effect did not change on subgroup analysis. Moreover, the leave-one-out analysis demonstrated the robustness of the meta-analysis for these outcomes.
Fig. 3. Forest plot depicting the odds of complete (A) and adequate (B) occlusion in PED vs. FRED groups (Experimental: PED; Control: FRED)
While meta-regression demonstrated that female gender, saccular shape, and prior treatment as the main sources of heterogeneity for complete occlusion, only prior treatment was associated with the calculated effect. Regarding adequate occlusion, publication year and follow-up duration were identified as sources of heterogeneity (Table 3). Meta-regression was not performed for residual aneurysm rate due to the limited number of studies.
Table 3. Meta-regression details for outcomes with significant heterogeneity on primary analysisKEstimate10SE**P-ValR^2Complete OcclusionYear15-0.488.200.950.00Age13-2.835.920.630.00Female %132.521.640.1332.96Follow-Up140.622.080.770.00Rupture Rate %13-2.922.580.263.01Saccular Shape %111.461.020.1534.23Prior Treatment %83.701.750.03100.00Additional Coiling %91.271.510.400.00Aneurysm Size11-0.189.260.980.00Adequate OcclusionYear88.1212.590.525.67Age74.1310.250.690.00Female %70.503.030.870.00Follow-Up74.134.080.318.86Rupture Rate %70.404.290.930.00Saccular Shape %60.121.960.950.00Prior Treatment %47.538.100.350.00Additional Coiling %51.354.390.760.00Aneurysm Size419.7527.230.470.00Need for Adjunctive CoilingYear727.1218.890.1523.79Age68.9312.520.480.00Female %610.3316.210.520.00Follow-Up71.405.400.800.00Rupture Rate %6-7.6010.720.480.00Saccular Shape %6-4.407.260.540.00Prior Treatment %5-2.695.180.600.00Aneurysm Size52.8620.780.890.00RetreatmentYear64.2624.200.860.00Age615.2930.000.610.00Female %64.872.580.05100.00Follow-Up6-3.497.930.660.00Rupture Rate %6-7.414.150.07100.00Saccular Shape %62.761.430.05100.00Prior Treatment %4-0.1111.850.990.00Additional Coiling %43.2516.190.840.00Aneurysm Size416.6231.270.600.00
Good functional outcome (mRS ≤ 2) at the last follow-up (1447patients) was more common in the FRED group compared to the PED group (17.12% vs. 7.17%, OR:0.35, P < 0.01, Fig. 4A). Analysis of matched studies revealed a similar effect (OR:0.31, P = 0.01). The observed effect did not change on leave-one-out analysis.
Fig. 4. Forest plot depicting the odds of good functional outcome (A) and retreatment (B) in PED vs. FRED groups (Experimental: PED; Control: FRED)
Adjunctive coiling was more frequently required in patients treated with FRED (17.12% vs. 7.17%, OR:0.42, P = 0.04). Moreover, while there was a trend toward lower retreatment rates in the FRED group, retreatment rates were not significantly different (PED:6.81% vs. FRED:0.58%, OR:2.51, P = 0.08, Fig. 4B). However, the difference in retreatment rates was significant on leave-one-out analysis, after omitting Griessenauer et al. (OR:4.71, P = 0.01). The main source of heterogeneity was the year of study for adjunctive coiling. Regarding retreatment, the heterogeneity was sourced from the female gender, rupture rate, and saccular shape (Table 3).
Complications & mortality
The two FDs had comparable total complication rates (PED:12.52% vs. FRED:13.25%, OR:0.94, P = 0.86). Meta-regression of total complication was not conducted due to the limited number of studies. The hemorrhage rate was 3.12% and 1.13% in the PED and FRED groups, respectively (OR:2.01, P = 0.07, Fig. 5A). In the leave-one-out analysis, the hemorrhage rate was significantly higher in the PED group, when omitting Gundogmus et al. (OR:2.35, P = 0.04). Rates of thromboembolic complication were comparable between the two groups (PED:4.74% vs. FRED:4.50%, OR:0.77, P = 0.25, Fig. 5B). Procedural-related complication rates were comparable between the two groups (PED:6.02% vs. FRED:4.31%, OR:1.48, P = 0.36, Fig. 6A). In-stent stenosis was observed in 6.52% and 12.11% of patients in the PED and FRED groups, respectively (P = 0.17, Fig. 6B).
Fig. 5. Forest plot depicting the odds of hemorrhage (A) and thromboembolic (B) events in PED vs. FRED groups (Experimental: PED; Control: FRED)
Fig. 6. Forest plot depicting the odds of procedural-related complications (A), in-stent stenosis (B), neurological complications (C), and need for additional treatments (D) in PED vs. FRED groups (Experimental: PED; Control: FRED)
Neurological complication rates were comparable between the two groups (PED:1.79% vs. FRED:1.02%, OR:1.52, P = 0.45, Fig. 6C). The need for additional treatment (e.g. balloon angioplasty, etc.) was comparable between the two groups (PED:5.63% vs. FRED:4.62%, OR:1.30, P = 0.71, Fig. 6D). Lastly, mortality rates were comparable between the two groups (PED:1.48% vs. FRED:0.79%, OR:1.21, P = 0.80).
Risk of bias
The majority of studies had low to moderate risk of bias (81.25%) with confounding factors being the main source of bias (Fig. 7). None of the analyzed outcomes revealed publication bias on Egger’s regression and visual inspection of funnel plots.
Fig. 7. Details of risk of bias according to ROBINS-I
Discussion
Overview
FDs, placed in the parent artery, induce stasis within the aneurysm sac by diverting blood flow. Over time, endothelialization around the neck results in complete exclusion of the aneurysm from the vasculature [27]. Two FDA-approved FDs, PED and FRED, offer solutions for complex aneurysms that are often difficult to treat with traditional methods [7]. PED utilizes a cylindrical mesh design, featuring platinum and cobalt-chromium braided strands, available in various single or multi-layered configurations. In contrast, FRED is a braided double-stent device made from nitinol wires, with expansions of the outer stent at both ends.
Although both PED and FRED have shown promising effectiveness and safety, there are controversies regarding the comparison between the two devices. While a recent meta-analysis compared these two approaches, it suffered from incomplete inclusion and severe statistical shortcomings [28]. Accordingly, this is the most comprehensive review comparing PED and FRED and factors associated with various outcomes while considering the baseline characteristics and matching status of the included studies. The results reveal comparable occlusion rates and safety profiles for the two devices. Interestingly, FRED was associated with both an increased need for adjunctive coiling and better functional outcomes following treatment, which potentially suggests the baseline functional status was better in the FRED group. Given the extensive meta-analysis and minimal heterogeneity of calculated effects, these findings provide strong evidence of the non-inferiority of the FRED device compared to the more commonly utilized PED.
Angiographic and clinical outcome
PED was approved by FDA for treating large/giant, wide-necked aneurysms in the internal carotid artery, specifically from the petrous to the superior hypophyseal segments in 2011. This approval was based on the results of the PUFS trial which demonstrated a high rate (73.6%) of complete occlusion without major narrowing of the parent artery or need for additional embolic material at 180-day follow-up [29]. Further follow-up data from the PUFS trial showed increasing complete occlusion rates, reaching 95.2% at 5 years for this challenging cohort of aneurysms. Importantly, the rates of new serious adverse events were low, at 1%, 3.5%, and 0% at 1, 3, and 5-years, respectively [30, 31]. Consistently, the PREMIER study reported a complete occlusion rate of 76.8% at 1-year and 83.3% at 3-year evaluation [32, 33]. Due to the high efficacy and favorable safety profile of PEDs, further technological advancements have been made to improve ease of use and reduce complications. These advancements include the introduction of PED Flex with reheating technology and PED Flex with Shield technology [34, 35, 36]. Both iterations have shown comparable occlusion rates to the original PED while potentially reducing complication rates [37, 38].
The first large study of the FRED device, involving 15 European neurovascular centers, found that complete occlusion rates increased over time: 20% at 90 days, 82.5% at 180 days, 91.3% at 1 year, and 95.3% for follow-ups exceeding 1 year. Additionally, temporary and permanent complications occurred in 3.2% and 0.8% of procedures, respectively, with an overall mortality rate of 1.5% [39]. Further evidence came from a US pivotal trial focusing on FRED for intracranial aneurysms considered unsuitable for traditional endovascular treatments. This trial showed a technical success rate of 57.6% at 1 year. Additionally, 6.2% of patients experienced death or major stroke within 30 days, or any major stroke or neurological death affecting the same side of the body within 12 months of the procedure [40]. A post-market evaluation of FRED showed similar findings: 74.2% complete occlusion, 11.3% near-complete occlusion, 2.8% retreatment rate, and 2.8% permanent ischemic complications [6]. The present study found consistent angiographic occlusion rates with no significant differences between the PED (complete:76.02%, adequate:83.46%) and FRED (complete:73.95%, adequate:88.46%). Several studies reviewed here report comparable occlusion rates between FRED and PED. However, Matsukawa et al. found a significantly higher rate of complete and adequate occlusions with FRED compared to PED. They suggested this could be due to the space between FRED’s layers, which disrupts blood flow, increases stagnation, traps platelets, and promotes further clot formation [41]. It should be noted that PED received FDA approval approximately eight years before FRED and surgeons are more experienced in using PED [37]. However, as demonstrated in the present analysis, both methods demonstrate similar effectiveness, even after matched analysis, suggesting that the lessons learned from operators experienced with PED deployment may be relevant to the use of the FRED. Theoretical technical advantages to FRED might include a self-expanding structure, easier opening in landing zones (smoother deployment in both the distal and proximal ends of the device), and a smaller size of delivery catheter required for FRED Jr in treating aneurysms in smaller and distal arteries, potentially offering greater versatility [27].
Furthermore, regarding neurological outcomes after treatment, our study found that patients who received FRED had significantly higher rates of favorable outcomes compared to those who received PED in the published comparative studies. This finding remained significant even when we restricted the analysis to matched studies only. Although the significant difference may have been attributed to the lower rates of hemorrhagic complications, the reason for this observed difference is not yet fully understood. It is possible that selection bias and other factors not accounted for in the matching process may have influenced the results, and it is possible that the FRED was used in patients with better baseline functional status, or in easier-to-treat aneurysms [15]. Further comparative studies are needed to elucidate these findings.
Procedural details
The use of adjunctive coiling alongside FDs for treating intracranial aneurysms is a topic of debate. Some studies suggest that adjunctive coiling can promote progressive intra-aneurysmal thrombosis, leading to improved aneurysm occlusion, and potentially preventing delayed rupture [42]. Additionally, it might be more effective in inducing early complete occlusion and may be more suitable for cases with high rupture risk [43, 44, 45]. However, a meta-analysis revealed comparable occlusion rates between patients receiving FDs with or without adjunctive coiling [46]. Our study revealed significantly higher rates of adjunctive coiling in the FRED group compared to the PED group. This could be due to specialists favoring FRED for patients deemed to have a higher risk of rupture, a profile often requiring adjunctive coiling. Interestingly, the meta-regression analysis showed no significant association between adjunctive coiling rates and either occlusion or complication rates. These findings align with the aforementioned meta-analysis, suggesting that adjunctive coiling might not significantly impact outcomes in either FRED or PED treatment.
Complications
Our study identified a trend toward increased hemorrhagic complications in patients treated with the PED, which became statistically significant after excluding the study by Gündoğmuş et al. Their study reported higher hemorrhage rates in the FRED group compared to other included publications. This discrepancy may be attributable to the higher proportion of ruptured aneurysms (8% vs. 4%) and significantly greater use of adjunctive coiling (37% vs. 22%) in their FRED cohort relative to the PED group in the same study, both of which suggest a higher risk of re-rupture and have known associations with hemorrhagic complications following flow diversion therapy [47, 48]. The difference in hemorrhagic complication between PED and FRED may not be solely due to the devices themselves. Existing research supports this notion. For instance, Gündoğmuş et al. reported various causes of hemorrhage unrelated to device type, including rupture of a previously treated aneurysm, bleeding caused by medication, spontaneous rupture despite coiling, inadequate coiling technique, and device migration [17]. Furthermore, the dual-layer architecture of FRED may offer advantages in directing blood flow away from the aneurysm while maintaining circulation in nearby perforating vessels. This design has the potential to mitigate ischemic events and hemorrhages. Additionally, the extent of flow diversion could be influenced by the surface area coverage of the aneurysm neck by the device’s struts. With FRED’s inner layer potentially providing greater metal coverage, there could be a more rapid occlusion of the aneurysm, potentially resulting in reduced hemorrhage rates.
Thromboembolic events are among the most serious complications of FDs, occurring in approximately 6% of patients [49, 50]. In our study, the pooled rates of thromboembolic events were 4.7% in the PED group and 4.5% in the FRED group. These rates vary across studies, likely due to differences in methodology and patient populations. Previous single-arm studies reported thromboembolic complication risks ranging from 2 to 7% following PED placement, aligning with our findings [33, 51, 52]. However, a recent study observed a thromboembolic event rate of 10.71% in patients treated with first-generation PED or PED Flex, compared to 3.57% for the PED Shield [53]. Similarly, thromboembolic event rates for FRED vary significantly between studies, [54] with one reporting a 6.9% incidence [5]. The higher thrombogenicity of FRED compared to other FDs has been corroborated by in vitro studies, potentially attributable to its dual-layer design. This structure increases metal surface area and creates localized turbulent blood flow, promoting platelet activation, fibrin deposition, and thrombus formation [55]. Notably, FRED X—a newer surface-coated device—demonstrated a markedly lower ischemic event rate compared to its predecessor (0.6% vs. 5.1%, respectively) [56]. Discrepancies between studies may arise from variations in patient selection criteria, antiplatelet regimens, medication adherence, clopidogrel resistance, procedural learning curves, and follow-up duration. Additional randomized controlled trials are warranted to validate and expand upon these findings.
Previous research suggests a link between the double-layer structure of FRED and a higher incidence of in-stent stenosis compared to PED. This association is hypothesized to be due to potential blood flow disruption and stasis within the dual layers, triggering platelet activation, fibrin buildup, and ultimately, clot formation [13, 55, 57]. However, in-stent stenosis rates were comparable between the two devices in our study. Additionally, we found nearly significantly higher retreatment in PED, which reached statistical significance after excluding the study by Griessenauer et al. [15]. This discrepancy arose because their study reported elevated retreatment rates following the FRED, contrasting with four other studies where no patients in the FRED group required retreatment [14, 16, 22, 58]. The Griessenauer et al. [15]. study included patients with posterior circulation aneurysms treated with PED or FRED as off-label interventions. The higher retreatment rates for FRED in their cohort may reflect the clinical teams’ heightened vigilance in detecting and managing incomplete occlusion or recurrence. This could stem from the inherent challenges of using FDs in posterior circulation aneurysms, compounded by limited institutional experience with FRED at the time of the study. Several factors may influence the difference in retreatment rates including a higher prevalence of incomplete occlusion with PED and a lower bar for retreatment decisions by the physicians managing those cases [16]. Overall, our findings suggest similar safety profiles for the two FDs when considering adverse events. However, future randomized controlled trials could provide more definitive insights.
In our present study, we found that the rates of additional treatment were comparable between the two groups. This observation aligns with the similarity of adverse events, including in-stent restenosis, hemorrhage, and thromboembolic events. However, a study by Matsukawa et al. revealed significantly higher rates of additional treatment in the PED treated patients [41]. This discrepancy may be ascribed to technical differences in performing additional treatment using stents and balloon angioplasty. For example, while previous research has demonstrated the safety and effectiveness of balloon angioplasty for foreshortening and improving apposition of PED, [59] in the case of FRED, passing a balloon through the stent is challenging due to its double-stent structure. The inner mesh of FRED may hinder the navigation of the balloon through the entire length of the stent [60].
Limitations
This study has several limitations to consider. While both PED and FRED are FDA-approved for treating large, wide-necked intracranial aneurysms, the comparative studies primarily focused on saccular aneurysms. This limits the applicability of our findings to the officially intended uses of PED and FRED. A limited number of studies provided details on the specific scales used to assess aneurysm occlusion. This prevented us from conducting analyses on specific occlusion levels. Two studies had slight overlap in their cohorts but were included to prevent patient loss. There was also significant heterogeneity across the studies in terms of patient selection criteria, device types, and follow-up durations, all of which could potentially influence the outcomes of our analysis. Furthermore, our review may not fully capture instances where thromboembolic events are significantly elevated (for example, in FRED-only cohorts), as studies solely comparing PED and FRED might inherently underrepresent these higher-risk populations. Additionally, we were unable to perform subgroup analyses based on specific device variations (PED Flex, PED Shield, and FRED X) because none of the studies reported outcomes for each device subtype separately. Considering that surface-modified FDs are considered to be safer iterations affecting the future of aneurysm treatment, comparative studies focusing on these devices are of utmost importance.
Conclusion
The current systematic review revealed that FRED is a suitable alternative to the commonly utilized PED. Despite slight demographic differences, both devices demonstrated comparable angiographic outcomes, with similar rates of complete and adequate occlusion. In this analysis of double-arm comparative studies, complication rates and mortality were similar between the two groups except for the slightly higher hemorrhage rates observed in PED. While both PED and FRED are effective treatment options, considerations regarding adjunctive interventions and retreatment rates should be weighed when selecting the appropriate device for individual patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cappuzzo JM, Monteiro A, Taylor MN et al (2022) First U.S. Experience Using the Pipeline Flex Embolization Device with Shield Technology for Treatment of Intracranial Aneurysms. World Neurosurg. 159:e 184-e 191. 10.1016/j.wneu.2021.12.03110.1016/j.wneu.2021.12.03134920157 · doi ↗ · pubmed ↗
- 2Rashidi F, Habibi MA, Reyhani M et al Pipeline Embolization Device and Flow Re-Direction Endoluminal Device for Intracranial Aneurysms: A Comparative Systematic Review and Meta-Analysis Study. World Neurosurg. 2024/06/24/ 2024;10.1016/j.wneu.2024.06.10010.1016/j.wneu.2024.06.10038925243 · doi ↗ · pubmed ↗
- 3Ramirez-Velandia F, Enriquez-Marulanda A, Filo J et al (2024) Comparison of thromboembolic events between pipeline embolization device (PED) shield and PED/PED flex: A propensity Score-Matched analysis. Neurosurgery Feb 23. 10.1227/neu.000000000000288310.1227/neu.000000000000288338391195 · doi ↗ · pubmed ↗
- 4Killer-Oberpfalzer M, Kocer N, Griessenauer CJ et al (May 2018) European multicenter study for the evaluation of a Dual-Layer Flow-Diverting stent for treatment of Wide-Neck intracranial aneurysms: the European Flow-Redirection intraluminal device study. AJNR Am J Neuroradiol 39(5):841–847. 10.3174/ajnr.A 559210.3174/ajnr.A 5592 PMC 741067529545252 · doi ↗ · pubmed ↗
- 5Feng W, Tian X, Kang J, Han Z, Chen E (2023) Flow diverter Device-Assisted coiling treatment for cerebral blister aneurysm: A Single-Center study. Brain Sci Mar 3(3). 10.3390/brainsci 1303043510.3390/brainsci 13030435 PMC 1004618636979245 · doi ↗ · pubmed ↗
- 6Cagnazzo F, Mantilla D, Rouchaud A et al (May 2018) Endovascular treatment of very large and giant intracranial aneurysms: comparison between reconstructive and deconstructive Techniques-A Meta-Analysis. AJNR Am J Neuroradiol 39(5):852–858. 10.3174/ajnr.A 559110.3174/ajnr.A 5591 PMC 741065729545248 · doi ↗ · pubmed ↗
- 7Kallmes DF, Hanel R, Lopes D et al (Jan 2015) International retrospective study of the pipeline embolization device: a multicenter aneurysm treatment study. AJNR Am J Neuroradiol 36(1):108–115. 10.3174/ajnr.A 411110.3174/ajnr.A 4111 PMC 796592025355814 · doi ↗ · pubmed ↗
- 8Goertz L, Hohenstatt S, Vollherbst DF et al (2024) Lower-Ischemic-Risk profile of coated flow Redirection endoluminal device X compared with uncoated flow Redirection endoluminal device flow diverter in the treatment of unruptured intracranial aneurysms. Neurosurgery Oct 8. 10.1227/neu.000000000000318810.1227/neu.000000000000318839471102 · doi ↗ · pubmed ↗