Low anterior chamber volume as a risk factor in non-arteritic anterior ischemic optic neuropathy
Durgul Acan, Beyza Betul Cakar, Eyyup Karahan

TL;DR
The study found that a lower anterior chamber volume is linked to a higher risk of non-arteritic anterior ischemic optic neuropathy.
Contribution
The study identifies low anterior chamber volume as a novel potential risk factor for NAION.
Findings
Eyes with NAION had significantly lower anterior chamber volume compared to healthy eyes.
No significant differences were found in axial length, anterior chamber depth, or iridocorneal angle between NAION and control groups.
Decreased anterior chamber volume may contribute to NAION risk.
Abstract
This study aimed to compare the anterior chamber depth (ACD), anterior chamber volume (ACV), and iridocorneal angle (ICA) of the eyes of patients with non-arteritic anterior ischemic optic neuropathy (NAION) and normal eyes. In this cross-sectional study, 28 patients with NAION who were admitted to our institution were examined. Central corneal thickness (CCT), ACV, ACD, and ICA of all eyes were measured using corneal topography (Sirius, CSO, Italy). Axial lengths (ALs) were measured using an IOL-Master 500 (Carl Zeiss, Meditec). The eyes of these patients were compared with the eyes of 29 healthy individuals of similar age and gender. The mean ALs of the eyes with NAION and those in the control group were not statistically different, measuring 22.95 ± 0.68 mm and 23.13 ± 0.80mm, respectively (p=0.651). While the average ACV was 137.93 ± 41.01 mm3 in the control group, it was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
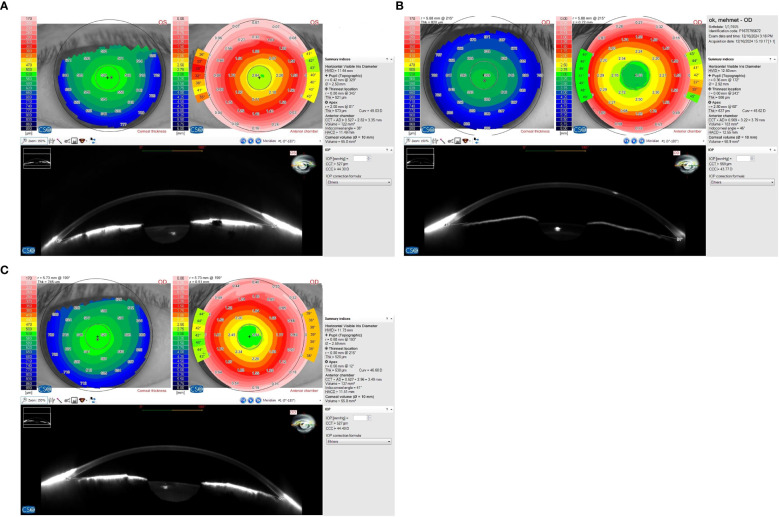 Figure 1
Figure 1| Variable | Study Group | Control Group | P value |
|---|---|---|---|
| Age, y, mean ± SD | 58.64 ± 7.86 | 57.86 ± 11.19 | 0.761 |
| Sex, n (%) | |||
| Male | 11(39.3) | 17(58.6) | 0.189 |
| Female | 17(60.7) | 12(41.4) | |
| Hypertension (%) | |||
| Yes | 9 (32.1) | 0 (0.0) | 0.001* |
| Diabetes mellitus (%) | |||
| Yes | 11 (39.3) | 0 (0.0) | 0.000* |
| Eye (right/left) | 16/12 | 29/0 | 0.000* |
| Parameter | NAION, N=28 | Fellow eyes, | Control, N=29 | P-value* | NAION Vs. control | Fellow eyes vs. control | NAION vs. fellow eyes |
|---|---|---|---|---|---|---|---|
| CCT, µm ± SD | 544.68 ± 31.26 | 547.03 ± 36.93 | 542.48 ± 19.39 | 0.849 | 0.959 | 0.835 | 0.953 |
| ICA, ° ± SD | 40.14 ± 7.04 | 39.75 ± 6.40 | 41.62 ± 6.99 | 0.552 | 0.693 | 0.557 | 0.975 |
| ACV, mm3 ± SD | 117.86 ± 22.23 | 118.07 ± 23.34 | 137.93 ± 41.01 | 0.019 | 0.038 | 0.040 | 1.000 |
| ACD, mm ± SD | 2.64 ± 0.31 | 2.66 ± 0.27 | 2.82 ± 0.57 | 0.203 | 0.236 | 0.323 | 0.988 |
| Axial length, mm ± SD | 22.95 ± 0.68 | 22.95 ± 0.81 | 23.13 ± 0.80 | 0.587 | 0.651 | 0.640 | 1.000 |
| IOP, mmHg ± SD | 15.46 ± 2.65 | 15.57 ± 2.75 | 14.79 ± 2.13 | 0.454 | 0.576 | 0.478 | 0.986 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntraoperative Neuromonitoring and Anesthetic Effects · Pain Management and Treatment · Anesthesia and Pain Management
Introduction
Non-arteritic ischemic optic neuropathy (NAION) is the most prevalent type of ischemic optic neuropathy in patients over 50 years of age (1, 2). The pathophysiology of NAION has not been fully elucidated yet. However, it is claimed that the crowding of the disc leads to a type of compartment syndrome, inhibiting axonal flow and causing vascular insufficiency related to existing systemic vascular diseases (3–6). The fellow eyes of these patients often also exhibit a small and crowded optic disc, commonly referred to as “disc at risk” in the literature. The presence of “disc at risk” indicates a high risk of developing NAION (7).
Differences in the anterior segment, such as corneal thickness and corneal biomechanics, have been previously determined in some diseases, such as normotensive glaucoma (8, 9). In a previous study conducted at our clinic, it was demonstrated that patients with central retinal vein occlusion (CRVO) exhibit anterior segment crowding, characterized by a reduced anterior chamber volume (ACV), resembling the anatomical configuration observed in a crowded optic nerve head (10). Only corneal thickness and hysteresis were evaluated in some studies on the relationship between NAION and anterior segment morphology (11, 12). The aim of this study was to compare anterior chamber morphology in NAION with normal eyes.
Materials and methods
In this cross-sectional study, 28 eyes of 28 patients who were followed up and treated with the diagnosis of NAION between May 2019 and January 2023 were included. Furthermore, 29 healthy eyes from 29 age- and gender-matched individuals with comparable axial lengths (ALs) were enrolled as the control group. The ethics committee of the university evaluated and approved this study in compliance with the guidelines outlined in the Declaration of Helsinki. All the patients in this study were informed about the purposes of the study, and written consent was obtained from all participants.
The diagnosis of NAION was described as an acute loss of visual acuity without pain, visual field abnormalities, an ipsilateral relative afferent pupillary deficiency, impairment in color vision, and optic disc edema with splinter hemorrhage. Only patients with normal C-reactive protein levels and erythrocyte sedimentation rates were included. Eyes suspected to have arteritic anterior ischemic optic neuropathy (AAION) based on clinical and laboratory results were excluded from the study. Eyes with intraocular pressure (IOP) greater than 21mmHg, glaucomatous optic nerve damage, glaucomatous visual field defects, a history of ocular surgery (including cataract surgery), ocular trauma, corneal scars, corneal or lens abnormalities (dense cataract) that could affect corneal and anterior segment biomechanical measurements, and refractive errors exceeding ±3 diopters spherical equivalent were excluded.
A complete ophthalmological and neuro-ophthalmological examination was applied to all participants, including best-corrected visual acuity (BCVA) with Snellen charts, pupillary light reaction, evaluation for the presence of relative afferent pupillary defect, color vision test with Ishihara plates, slit-lamp examination, IOP measurement with a Goldmann applanation tonometer, and funduscopy. Anterior chamber depth (ACD), ACV, central corneal thickness (CCT), and iridocorneal angle (ICA) values were automatically created by the Scheimpflug/Placido photography-based topography system and a Sirius topographer (Costruzione Strumenti Oftalmici, Florence, Italy) using Phoenix v2.6 software. A single clinician (B.B.C.) took three measurements for each eye and the measurements with best alignment and fixation were included. Due to the inability to obtain reliable refraction measurements in some eyes with NAION, AL was assessed as an alternative. The ALs were measured with an IOL-Master 500 (Carl Zeiss, Meditec). Affected and fellow eyes of the patients in the study group and the right eyes of the control group were evaluated. Figure 1 presents topographic data from the patients with NAION and from the control subjects.
Anterior chamber topographic data of the affected (A) and fellow (B) eyes of a patient with non-arteritic anterior ischemic optic neuropathy (NAION) and an eye in the control group (C).
All data were analyzed using SPSS v25.0 for Windows (SPSS Inc., Chicago, IL). The distribution of continuous variables was evaluated using the Shapiro–Wilks test and visual graphs (histogram, etc.). Continuous variables are presented as mean ± standard deviation. Differences between the affected eyes, fellow eyes in the study group, and the eyes in the control group were analyzed using ANOVA with Tukey’s post hoc tests. Statistical significance was accepted at p< 0.05.
Results
There was no difference between the two groups in terms of age and gender (p_1_ = 0.761 and p_2_ = 0.189, respectively). Table 1 presents the demographic characteristics of the patients in the study and control groups. When comparing the eyes with NAION, fellow eyes, and the eyes in the control group, no statistically significant differences were found in the mean values of the IOP (p=0.454). The mean AL was 22.95 ± 0.68 mm in the eyes with NAION, 22.95 ± 0.81 mm in the fellow eyes, and 23.13 ± 0.80 mm in the eyes of the control group, with no statistically significant difference among the groups (p=0.587). Since the eyes that underwent cataract surgery were excluded, all the eyes were phakic. Of the eyes with NAION, 16 were right eyes.
There was no difference in the mean CCT between the eyes with NAION, fellow eyes, and the eyes in the control group (p=0.849). The mean ACD in the aforementioned groups was 2.64 ± 0.31mm, 2.66 ± 0.27 mm, and 2.82 ± 0.57 mm, respectively (p=0.203). The assessment of mean ACV showed that the values were 117.86 ± 22.23 mm^3^, 118.07 ± 23.34 mm^3^, and 137.93 ± 41.01mm^3^ in the eyes with NAION, fellow eyes, and eyes in the control group, respectively, demonstrating a statistically significant difference among the groups (p=0.019). Post hoc analyses revealed that ACV was significantly lower in the eyes with NAION and fellow eyes compared to the healthy eyes in the control group (p_1_ = 0.038, p_2_ = 0.040). There was no significant difference between the mean ICA values of the eyes with NAION, fellow eyes, and the eyes in the control group (p=0.552) (Table 2).
Discussion
The anterior segment morphology of the eyes with NAION was evaluated in this study. ACV was found to be significantly lower in the eyes with NAION and the fellow eyes compared to the healthy eyes in the control group. However, with respect to CCT, ACD, and ICA, there were no significant differences between the three groups. The findings of this study provide important insights into the anterior segment structures of eyes with NAION and their fellow eyes.
Considering that the sclera, cornea, peripapillary ring, and lamina cribrosa are composed of similar extracellular matrix components, it is plausible that their biomechanical and anatomical features may also share similarities (11). Corneal thickness and corneal hysteresis have previously been investigated in patients with NAION. Jabaly-Habib et al. hypothesized that the cornea may be thinner in patients with NAION, and that, in parallel, their crowded optic discs may also be more susceptible to damage; however, they did not find a statistically significant difference (11). In another study, CCT was found to be thinner in the affected and fellow eyes of NAION patients compared to the control eyes, although the difference did not reach statistical significance (12). In a comparative analysis of 33 NAION patients and 33 healthy individuals, Uysal et al. reported that corneal hysteresis, which represents the dynamic deformation response of the cornea, and corneal resistance factor, which reflects corneal elasticity and structural resistance, were both lower in the affected and fellow eyes of NAION patients than in control eyes (12). The authors concluded that this corneal biomechanical weakness may indirectly reflect the structural fragility of the lamina cribrosa.
To the best of our knowledge, no prior study has specifically investigated the anterior chamber characteristics of eyes with NAION. However, Cankaya et al. examined 200 healthy eyes and reported an association between anterior segment morphology and the optic nerve head (13). They also emphasized a negative correlation between rim volume and both ACD and ACV, thereby supporting the potential role of anterior segment changes accompanying a crowded optic disc in the etiopathogenesis of NAION. The development of NAION after intravitreal injection and cataract surgery has been reported, suggesting the hypothesis that anatomical variations in the anterior chamber may lead to transient IOP spikes in susceptible eyes, which may result in impaired perfusion of the optic nerve head (14, 15).
In this study, in addition to a reduced ACV, ACD was also found to be shorter in the eyes with NAION and the fellow eyes compared to the healthy controls; however, the difference did not reach the level of statistical significance. Another important finding was that the ICA did not differ significantly between the eyes with NAION and the control eyes. Although some studies reported the coexistence of NAION and angle-closure glaucoma, no comparative study has been published on the relationship between angle-closure glaucoma and NAION (16–21). In accordance with these reports, an abrupt rise in IOP with acute angle closure can trigger hypoperfusion and ischemia of the optic nerve head and the development of NAION. As far as we know, anterior chamber findings were evaluated for the first time in this study and ACV was found to be lower in both eyes of the patients with NAION, while ICA, although narrower, did not reach statistical significance.
In the present study, the prevalence of hypertension and diabetes was significantly higher in the patients with NAION compared to the control group, as expected, given that both diseases are considered risk factors for NAION (2). To our knowledge, there is no existing data in the literature demonstrating a relationship between systemic hypertension and anterior chamber parameters. However, in diabetes, lens abnormalities and reduced corneal sensitivity are frequently observed and they may indirectly influence the anterior segment (22). Accordingly, future research should be designed to include only non-diabetic NAION patients in order to eliminate the potential confounding effects of diabetes.
In light of current knowledge, the presence of a “disc at risk” appearance in the fellow eye of a patient presenting with signs of ischemic optic neuropathy is one of the most important clinical clues directing the clinician toward a non-arteritic etiology (23, 24). In this study, a reduced ACV was also identified as a potential risk factor for NAION. However, larger studies including a greater number of patients, particularly those involving eyes with AAION, which plays a critical role in the differential diagnosis of NAION, are needed to validate our findings.
The small sample size is one of the major limitations of this study, and future studies involving a larger number of patients are warranted. In addition, the absence of certain parameters, such as corneal hysteresis and lens thickness, further weakens the strength of the findings. Considering that diabetes may indirectly affect anterior chamber measurements, the inclusion of diabetic patients represents another limitation of the present study. Therefore, evaluating only non-diabetic patients with NAION in future research may provide more accurate and generalizable results.
Conclusion
Differences in anterior segment morphology were identified in both NAION eyes and fellow eyes compared to healthy eyes. Reduced ACV may be a potential risk factor for NAION; however, larger comparative studies are needed to confirm this finding.
The authors have no funding and conflicts of interest to disclose.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hattenhauer MG Leavitt JA Hodge DO Grill R Gray DT. Incidence of nonarteritic anterior ischemic optic neuropathy. Am J Ophthalmol. (1997) 123:103–7. doi: 10.1016/s 0002-9394(14)70999-7 9186104 · doi ↗ · pubmed ↗
- 2Salvetat ML Pellegrini F Spadea L Salati C Zeppieri M. Non-arteritic anterior ischemic optic neuropathy (NA-AION): A comprehensive overview. Vision (Basel). (2023) 7:72. doi: 10.3390/vision 7040072 37987292 PMC 10661278 · doi ↗ · pubmed ↗
- 3Hayreh SS. Ischemic optic neuropathy. Prog Retin Eye Res. (2009) 28:34–62. doi: 10.1016/j.preteyeres.2008.11.002 19063989 · doi ↗ · pubmed ↗
- 4Burde RM. Optic disk risk factors for nonarteritic anterior ischemic optic neuropathy. Am J Ophthalmol. (1993) 116:759–64. doi: 10.1016/s 0002-9394(14)73478-6 8250081 · doi ↗ · pubmed ↗
- 5Pahor D Gracner B. Hyperopia as a risk factor in patients with non-arteritic anterior ischaemic optic neuropathy. Klin Monbl Augenheilkd. (2008) 225:1070–4. doi: 10.1055/s-2008-1028000 19085788 · doi ↗ · pubmed ↗
- 6Bernstein SL Miller NR. Ischemic optic neuropathies and their models: disease comparisons, model strengths and weaknesses. Jpn J Ophthalmol. (2015) 59:135–47. doi: 10.1007/s 10384-015-0373-5 PMC 455637025690987 · doi ↗ · pubmed ↗
- 7Beck RW Servais GE Hayreh SS. Anterior ischemic optic neuropathy. IX. Cup-to-disc ratio and its role in pathogenesis. Ophthalmology. (1987) 94:1503–8. doi: 10.1016/S 0161-6420(87)33263-4 3684223 · doi ↗ · pubmed ↗
- 8Xu Y Ye Y Chen Z Xu J Yang Y Fan Y. Corneal stiffness and modulus of normal-tension glaucoma in Chinese. Am J Ophthalmol. (2022) 242:131–8. doi: 10.1016/j.ajo.2022.06.014 35764102 · doi ↗ · pubmed ↗