Comparison of Clinical Characteristics Between Bullous and Non-bullous Rheumatoid Neutrophilic Dermatosis: A Case Report, Literature Review, and Proposed Diagnostic Criteria
Masakazu Kakurai, Kazuma Iwamoto, Yoshihiro Moriyama

TL;DR
This case report describes a rare bullous form of rheumatoid neutrophilic dermatosis and proposes new diagnostic criteria to distinguish it from similar conditions.
Contribution
The paper introduces five proposed diagnostic criteria for bullous rheumatoid neutrophilic dermatosis, previously undocumented.
Findings
Bullous RND presented with painful bullae, pustules, and erythematous lesions on lower extremities.
Treatment with dapsone improved skin lesions and arthralgia within one week.
Diagnostic criteria emphasize rheumatoid arthritis activity and neutrophilic infiltration without vasculitis.
Abstract
Rheumatoid neutrophilic dermatosis (RND) is associated with rheumatoid arthritis and typically presents as papules, nodules, and/or plaques bilaterally on the extremities. Rarely, vesiculobullous lesions (bullous RND) may occur. We herein present a case of bullous RND diagnosed in our department. A 70-year-old Japanese woman presented with multiple painful, tense bullae, accompanied by pustules, erythematous papules, and erosions on the lower extremities, and a few hemorrhagic bullae were observed on the soles. Her medical history included seropositive rheumatoid arthritis for 14 years, which was successfully treated with oral prednisolone and tacrolimus hydrate, but joint pain and swelling developed one month before her visit to our department. A skin biopsy of the blister on the lower leg revealed an intraepidermal and subepidermal blister, containing numerous neutrophils. Marked…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
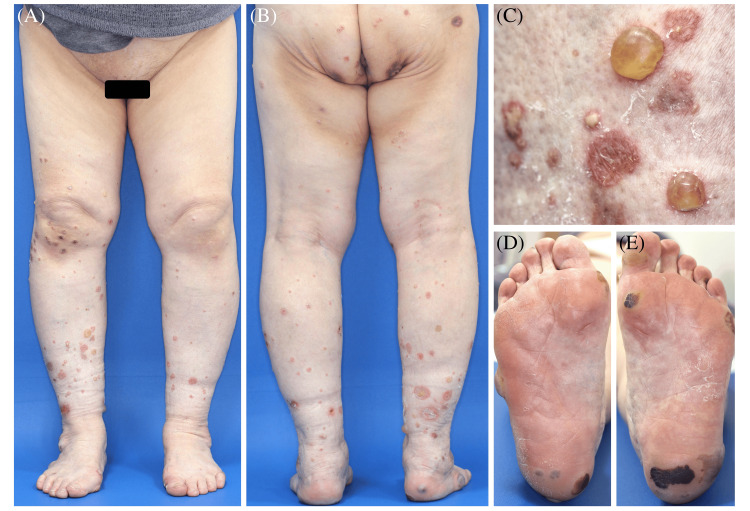 Figure 1
Figure 1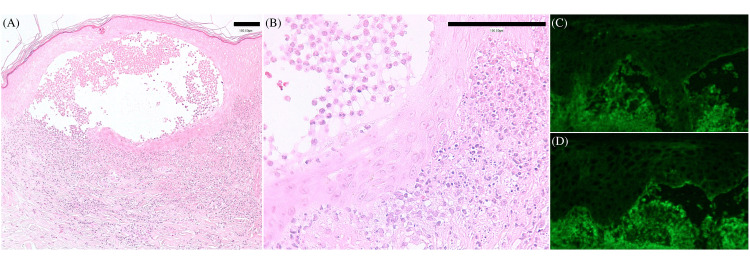 Figure 2
Figure 2| Parameter | Reference value (female) | On arrival |
| Aspartate aminotransferase (U/L) | 8-35 | 24 |
| Alanine aminotransferase (U/L) | 4-40 | 18 |
| Sodium (mEq/L) | 135–150 | 138 |
| Potassium (mEq/L) | 3.5–5.0 | 4.9 |
| Urea nitrogen (mg/dL) | 7–20 | 52 |
| Creatinine (mg/dL) | 0.40–1.20 | 1.43 |
| Creatine kinase (U/L) | 57–160 | 96 |
| C-reactive protein (mg/dL) | 0–0.30 | 2.13 |
| White blood cell (/μL) | 4,000–9,000 | 10,460 |
| Neutrophils (%) | 45.0-70.0 | 65.7 |
| Hemoglobin (g/dL) | 12.0–15.0 | 12.5 |
| Platelet (×104 /μL) | 15.0–35.0 | 19.8 |
| Rheumatoid factor (IU/mL) | 0-15 | 1712 |
| Erythrocyte sedimentation rate (mm/h) | 0-15 | 73 |
| Anti-desmoglein 1 antibodies (U/mL) | 0-19 | <20 |
| Anti-desmoglein 3 antibodies (U/mL) | 0-19 | <20 |
| Anti-BP180 NC16A antibody (U/mL) | 0-8 | <9 |
| Author/Year | Age/ Sex | RA duration (years) | Lesion sites | Erythema surrounding the blisters | Effective treatment |
| Lowe et al., 1992 [ | 56/F | 10 | Extremities | NA | Naturally healed |
| Lu et al., 2004 [ | 35/M | 18 | Extremities | − | Dapsone |
| Kreuter et al., 2005 [ | 78/F | 15 | Lower extremities | − | Etanercept |
| Yamamoto et al., 2010 [ | 65/F | >20 | Lower extremities | − | Topical steroid |
| Fujio et al., 2014 [ | 78/F | 2 | Extremities and back | − | Etanercept |
| Soza et al., 2015 [ | 56/F | >10 | Extremities | − | Topical steroid |
| Shin et al., 2015 [ | 64/F | 10 | Extremities | − | Dapsone |
| Kosumi et al., 2017 [ | 78/F | 2 | Lower extremities | Mild | NA |
| Ha et al., 2021 [ | 45/F | 3 | Extremities | NA | NA |
| Our case | 70/F | 14 | Lower extremities | Mild | Dapsone |
| RND types | Bullous RND; N=10 | Non-bullous RND; N=29 | p-value a |
| Age, mean (range) years | 62.5 (35-78) | 49.8 (21-74) | 0.031 |
| Sex | 0.4 | ||
| Male | 1 (10) | 8 (28) | |
| Female | 9 (90) | 21 (72) | |
| RA duration, mean (range) years b | 9.3 (2-18) | 6.2 (0-20) | 0.247 |
| <10 years c | 3 (30) | 19 (73) | 0.026 |
| ≥10 years c | 7 (70) | 7(27) | |
| RA severity | |||
| High severity | 7 (70) | 12 (41) | |
| Low severity or remission | 0 (0) | 0 (0) | |
| Not described | 3 (30) | 17 (59) | |
| RA characteristics | |||
| Seropositive RA | 10 (100) | 22 (76) | |
| Seronegative RA | 0 (0) | 7 (24) | |
| Medical history other than RA | |||
| Monoclonal IgA gammopathy | 1 (10) | 0 (0) | |
| Dysglobulinemia | 0 (0) | 1 (3) | |
| Interstitial pneumonia | 1 (10) | 0 (0) | |
| Sjögren’s syndrome | 0 (0) | 2 (7) | |
| Others | 3 (30) | 1 (3) | |
| None/Not described | 5 (50) | 25 (86) |
| RND types | Bullous RND; N (%), N=10 | Non-bullous RND; N (%), N=29 |
| Lesion sites | ||
| Head (neck/face/scalp) | 0 (0) | 1 (3) |
| Head+trunk+extremities | 0 (0) | 3 (10) |
| Trunk+extremities | 1 (10) | 10 (34) |
| Trunk | 0 (0) | 1 (3) |
| Extremities | 5 (50) | 7 (24) |
| Upper extremities | 0 (0) | 5 (17) |
| Lower extremities | 4 (40) | 2 (7) |
| Painful rash | ||
| Yes | 2 (20) | 8 (28) |
| No (pruritic rash) | 1 (10) | 6 (21) |
| No (asymptomatic) | 2 (20) | 7 (24) |
| Not described | 5 (50) | 8 (28) |
| Papillary dermal edema | ||
| Yes | 0 (0) | 4 (14) |
| No | 7 (70) | 14 (48) |
| Not described | 3 (30) | 11 (38) |
| Leukocytoclasis | ||
| Yes | 6 (60) | 19 (66) |
| No | 0 (0) | 3 (10) |
| Not described | 4 (40) | 7 (24) |
| RND treatment | Bullous RND; N (%), N=10 | Non-bullous RND; N (%), N=29 |
| Topical steroids | 2 (20) | 2 (7) |
| PSL | 0 (0) | 4 (14) |
| Dapsone | 3 (30) | 4 (14) |
| Etanercept | 2 (20) | 0 (0) |
| Cyclosporine | 0 (0) | 1 (3) |
| HCQ | 0 (0) | 1 (3) |
| Cyclophosphamide | 0 (0) | 1 (3) |
| PSL+MTX | 0 (0) | 1 (3) |
| PSL+colchicine+AZM | 0 (0) | 2 (7) |
| PSL+MTX+HCQ | 0 (0) | 1 (3) |
| Spontaneous remission | 1 (10) | 0 (0) |
| Not described | 2 (20) | 12 (41) |
| RND types | Bullous RND | Non-bullous RND |
| RA duration until onset of RND | ≥10 years | <10 years |
| Clinical features | Tense vesiculobullous lesions without prominent surrounding erythema, predominantly on the lower extremities | Multiple erythematous papules, nodules, and plaques on the trunk and extremities |
| Histological features | Intraepidermal or subepidermal blister, without acantholysis, and marked neutrophilic infiltration in the dermis without leukocytoclastic vasculitis | Dense neutrophilic dermal infiltrate without leukocytoclastic vasculitis |
| Diagnostic criteria for RND a | (1) A definitive diagnosis of RA; (2) high RA disease activity; (3) multiple erythematous papules, nodules, plaques, and/or tense vesiculobullous lesions; (4) predominantly neutrophilic dermal infiltrate without leukocytoclastic vasculitis; (5) microbial sterility | |
| Differential diagnosis | Sweet’s syndrome, rheumatoid vasculitis, pyoderma gangrenosum, erythema elevatum diutinum | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutoimmune and Inflammatory Disorders · Autoimmune Bullous Skin Diseases · Skin Diseases and Diabetes
Introduction
Neutrophilic dermatosis (ND) is an inflammatory skin disorder with unique clinical features characterized by a sterile, predominantly neutrophilic infiltrate on histology, and includes Sweet’s syndrome (SS), pyoderma gangrenosum (PG), bowel-associated dermatosis-arthritis syndrome, and rheumatoid neutrophilic dermatosis (RND) [1]. RND, first described by Ackerman in 1978, is associated with severe rheumatoid arthritis (RA) [2]. The condition typically presents as asymptomatic multiple erythematous papules, nodules, and/or plaques bilaterally on the extremities, with a sterile dense neutrophilic dermal infiltrate and no vasculitis on histological examination [3]. Rarely, vesiculobullous lesions may also occur [3]. RND presenting with vesiculobullous lesions (bullous RND) was initially reported by Lowe et al. in 1992 [4].
RA is a systemic inflammatory disorder with both articular and extra-articular involvement, occurring mainly after middle age [5,6]. Female patients with RA outnumber male patients by a ratio of approximately 2.5 to 1 [5]. Extra-articular involvement is common, affecting almost every organ system [5]. Among the extra-articular involvements, specific skin manifestations are diverse and include classic rheumatoid nodules, accelerated rheumatoid nodulosis, granulomatous dermatitis, rheumatoid vasculitis (RV), PG, and RND [5].
Therefore, the diagnosis of RND can be challenging owing to the wide range of clinical manifestations and the variety of skin disorders associated with RA. Although the clinical characteristics of RND have been reported [3], the clinical differences between bullous and non-bullous RND remain unclear. In addition, RND is clinicopathologically similar to SS, and the distinction between the two is still debated, with no diagnostic criteria currently available for RND. Therefore, we aimed to identify the differences in the clinical characteristics of bullous and non-bullous RND and to propose a clinical practice guide for RND. Additionally, this literature reports the clinical and histological features of a patient with bullous RND diagnosed in our department.
Case presentation
A 70-year-old Japanese woman presented with a two-week history of a painful rash on her lower extremities. Her medical history included seropositive RA for 14 years, which was successfully treated with a combination of oral prednisolone (PSL) 5 mg daily and tacrolimus hydrate 2 mg daily. However, joint pain and swelling occurred one month before her visit to our department, and she was diagnosed with severe RA. Physical examination revealed multiple painful, tense bullae up to 1.5 cm in diameter, accompanied by pustules, erythematous papules, and erosions on the lower extremities (Figure 1A-1C). A few hemorrhagic bullae were observed on the soles (Figure 1D, 1E).
Clinical images of bullous RND experienced in our department(A-C) Multiple painful, tense bullae and blisters, accompanied by pustules, erythematous papules, and erosions on the lower extremities. Mild erythema around the bullae, blisters, and pustules are observed. (D, E) Hemorrhagic bullae on the soles.RND: rheumatoid neutrophilic dermatosis
A skin biopsy of the blister on the lower leg revealed an intraepidermal and subepidermal blister, containing numerous neutrophils. Marked neutrophilic infiltration, showing prominent leukocytoclasis, was observed in the dermis without vasculitis (Figure 2A, 2B). Direct immunofluorescence (DIF) yielded negative results (Figure 2C, 2D).
Histological and immunofluorescence findings of bullous RND experienced in our department(A, B) Intraepidermal and subepidermal blister containing numerous neutrophils without acantholytic cells. Marked neutrophilic dermal infiltration showing prominent leukocytoclasis without vasculitis. Bars indicate 100 μm. (C, D) DIF yields negative results for C3 (C), IgG (D), IgA, and IgM.RND: rheumatoid neutrophilic dermatosis; DIF: direct immunofluorescence
Blood tests revealed leukocytosis of 10,460 /μL (normal; 4,000-9,000 /μL) with 65.7% neutrophils and were significant for C-reactive protein (CRP): 2.13 mg/dL (normal; <0.30 mg/dL), rheumatoid factor (RF): 1712 IU/mL (normal; <15 IU/mL), and erythrocyte sedimentation rate: 73 mm/h (normal; <15 mm/h) (Table 1). Neither anti-desmoglein 1, 3 antibodies nor anti-BP180 NC16A antibody was detected.
Bacterial cultures from the blisters were sterile. Therefore, the diagnosis of bullous RND was made. Despite treatment with oral minocycline at 100 mg daily for one week, new skin lesions developed. Treatment was switched to dapsone at 75 mg daily, resulting in the improvement of skin lesions and arthralgia within one week, leaving mild hyperpigmentation. Dapsone was discontinued after three months, and the patient was followed up for one month after cessation, during which no recurrences were observed.
Discussion
We reviewed English-language articles on bullous and non-bullous RND published between January 1, 1989, and September 1, 2024. A structured literature search of PubMed was performed, using the keywords “(bullous) rheumatoid neutrophilic dermatosis” or “(bullous) rheumatoid neutrophilic dermatitis.” Relevant articles were screened for key terms and included if appropriate. Bullous RND was defined as RND with vesiculobullous lesions, while non-bullous RND was defined as RND without vesiculobullous lesions.
We identified 40 articles (48 patients) on RND and excluded patients whose iatrogenic RND developed during treatment with interleukin (IL)-6-receptor antagonists [7,8], as drug-induced cases may have distinct clinical or histological features that differ from classic RND. Articles on patients with atypical RND presenting with a solitary skin lesion [9], confined to the same site after trauma [10], and with symmetrically localized erythematous plaques were excluded [11-13]. We also excluded patients with RND who had histological vasculitis [14] and positive DIF results [15], whose diagnoses could not be definitively distinguished from differential diagnoses of RND, including RV.
Ultimately, our study included 10 patients with bullous RND [4,16-23], including an additional patient diagnosed in our department, and 29 patients with non-bullous RND [4,24-46] (Table 2).
Tables 3-5 summarize the comparison of RA characteristics (Table 3), clinicopathological features (Table 4), and treatment data (Table 5) between patients with bullous and non-bullous RND.
Table 3: Comparison of the RA characteristics of the patients with bullous and non-bullous RNDRND: rheumatoid neutrophilic dermatosis; RA: rheumatoid arthritis. Data are presented as N (%) unless otherwise specified.The mean age at diagnosis of bullous RND was 62.5 years, higher than that of non-bullous RND. Bullous and non-bullous RND were predominantly observed in females. The mean time from RA to bullous RND diagnosis was longer than that of non-bullous RND. The proportion of patients with more than 10 years between the RA and RND diagnoses was 70% in the bullous RND group, which was higher than that in the non-bullous RND group (27%). All patients with RND, except those not described, had severe RA disease activity prior to the development of skin lesions or before consultation. Seropositive RA was noted in all patients with bullous RND, whereas seven patients (24%) with non-bullous RND were seronegative for RA. RND was not complicated by infectious diseases, malignancies, or inflammatory bowel disease and was associated with monoclonal IgA gammopathy and dysglobulinemia, but no hematological malignancies were reported.a Disease characteristics were compared between subgroups using the Mann-Whitney or Fisher’s exact test as appropriate. Statistical tests were two-sided, and p-values less than 0.05 were considered statistically significant. We used Microsoft® Excel for Mac ver. 16.95.4 (Microsoft Corp., Redmond, WA).b The number of patients in the bullous and non-bullous RND groups for whom the exact RA duration was known was 8 and 26, respectively.c The number of patients in the bullous and non-bullous RND groups for whom RA duration could be categorized as either <10 years or ≥10 years was 10 and 26, respectively.
We discovered that the mean age at diagnosis of bullous RND was higher than that of non-bullous RND. This may be due to the longer duration of RA in patients with bullous RND, as 70% of these patients had RA for more than 10 years. Interestingly, we also identified that vesiculobullous lesions were absent in all patients with seronegative RA who developed RND [24-30]. RA can be divided into two types (seropositive and seronegative) based on the presence or absence of RF and anti-citrullinated protein antibodies. Seronegative patients have been reported to demonstrate higher disease activity than seropositive ones [6]. Patients with seronegative RA who developed RND had severe RA before the onset of RND [24-30], and their skin lesions improved with joint involvement [27,28], suggesting a parallel disease course between RND and RA. Therefore, high disease activity in RA may be involved in the onset and exacerbation of RND, even in seronegative patients.
Although the pathophysiology of RND remains unclear, evidence suggests chemokine-mediated neutrophil recruitment (e.g., IL-8 from synovial tissue) plays a key role [37], distinguishing it from SS, where systemic cytokine dysregulation (e.g., G-CSF) is more prominent. Yamamoto et al. reported that serum levels of IL-6 and IL-8 were elevated in a patient with non-bullous RND, but IL-1, IL-2, and tumour necrosis factor-alpha levels were within normal limits [37]. They speculated that IL-8 from synovial tissue, which can attract neutrophils, may contribute to leukocyte accumulation and inflammatory processes in the skin. Kubota et al. reported that immunohistochemistry of specimens from a patient with RND that developed while using an IL-6-receptor antagonist expressed high levels of IL-6 and IL-8, suggesting that the paradoxical drug effect may have been caused by a cytokine imbalance that increased IL-6 [7].
According to a recent literature review of 54 patients, RND presented most frequently as erythematous papules (31%), nodules (15.1%), and/or plaques (13.5%), often distributed in the extremities, and vesiculobullous lesions accounted for 12.7% of patients [3]. In this study, vesiculobullous lesions were found in 25.6% of RND patients. Bullous RND was characterized by tense vesiculobullous lesions without prominent surrounding erythema. Vesiculobullous lesions developed on the extremities, especially on the lower extremities, and no lesions were observed in the chest, abdomen, face, head, and neck. In contrast, skin lesions of non-bullous RND often appeared on the extremities, sometimes on the trunk, and rarely on the head and neck region.
The main differential diagnoses for RND include RV, PG, erythema elevatum diutinum (EED), and SS [3]. RV is a complication of RA that can lead to both systemic symptoms, including fever and peripheral neuropathy, and skin lesions such as ulcers, purpura, hemorrhagic blisters, nodular erythema, and livedo reticularis [5]. The histological findings of RV are leukocytoclastic vasculitis and/or necrotizing granulomatous vasculitis, which can be distinguished from RND. However, one patient with progression from RND to RV has been reported [13]. Since these two conditions can occur simultaneously in an individual, performing skin biopsies, when necessary, and depending on the clinical course, is important. PG is classified as ND and has four clinical variants: ulcerative, pustular, vegetative, and bullous [5,47]. Bullous PG, a rare variant of PG, must be distinguished from bullous RND. Bullous PG is characterized by painful hemorrhagic bullae that develop into rapidly progressive superficial ulcers [47]. Histologically, leukocytoclasis is often absent; however, secondary vasculitis may occur [5]. Bullous RND can be distinguished from bullous PG by a comprehensive assessment, including the lack of rapid progression of tense vesiculobullous lesions to ulcers, and histologically, the presence of leukocytoclasis without vasculitis. Although vesiculobullous formation is rare, EED can present with clinical findings similar to those of RND [4,5,21,38]. However, EED can be distinguished from RND by the presence of vasculitis [4,21,38].
SS is the most challenging differential diagnosis because of its similar clinicopathological presentation to RND. The diagnostic criteria for SS, consisting of two major and four minor criteria, were first proposed by Su and Liu in 1986 [1, 48]. In 1994, von den Driesch published a modification of these diagnostic criteria, requiring both major and two minor criteria for the diagnosis of SS [48]. The major criteria are as follows: (1) abrupt onset of tender or painful erythematous plaques or nodules, occasionally with pustules or blisters, and (2) predominantly neutrophilic dermal infiltrate without leukocytoclastic vasculitis. Minor criteria include the following: (1) preceded by a nonspecific respiratory or gastrointestinal tract infection or vaccination or associated with inflammatory diseases, malignancies, or pregnancy; (2) fever; (3) abnormal laboratory values, including leukocytosis; and (4) excellent response to treatment with PSL or potassium iodide. More recently, Nofal et al. revised the diagnostic criteria for SS and concluded that the abrupt onset of painful erythematous plaques and nodules associated with dense dermal neutrophilic infiltrate was sufficient to confirm the diagnosis of SS [48].
SS and RND share overlapping clinicopathological features, and patients with RND may fulfill the diagnosis of SS. Therefore, based on the characteristics of RND in this study and the differential diagnoses, we propose five diagnostic criteria for RND (Table 6): (1) a definitive diagnosis of RA; (2) high RA disease activity; (3) multiple erythematous papules, nodules, plaques, and/or tense vesiculobullous lesions; (4) predominantly neutrophilic dermal infiltrate without leukocytoclastic vasculitis; and (5) microbial sterility. Since all five of these criteria apply in the reported cases of bullous and non-bullous RND, the possibility of other diseases should be considered if one or more of these criteria are not met. Additionally, treatment response is not included among these criteria, as it varies between individuals, and effective treatments for RND remain poorly understood. We believe that further diagnosis and accumulation of RND cases will lead to a better understanding of treatment and help elucidate its pathophysiological mechanisms.
The limitations of this study include the restrictive inclusion criteria for English-language publications, a limited number of cases, and missing data in several studies. The lack of long-term follow-up data highlights the need for prospective studies to assess treatment durability and relapse rates in RND.
Conclusions
The duration of RA before the onset of bullous RND was often more than 10 years, which was longer than that of non-bullous RND. The clinical characteristics of bullous RND typically include tense vesiculobullous lesions without prominent surrounding erythema, most commonly on the lower extremities. In contrast, even though non-bullous RND lesions were common in the extremities, the trunk was more affected. Since bullous and non-bullous RND have different clinical characteristics, it is important to diagnose and document each subtype of RND to better clarify their clinicopathological differences and guide future treatment strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Neutrophilic dermatoses: Pathogenesis, Sweet syndrome, neutrophilic eccrine hidradenitis, and Behçet disease J Am Acad Dermatol Nelson CA Stephen S Ashchyan HJ James WD Micheletti RG Rosenbach M 98710067920182965321010.1016/j.jaad.2017.11.064 · doi ↗ · pubmed ↗
- 2Histologic Diagnosis of Inflammatory Skin Diseases: A Method of Pattern Analysis Ackerman AB 51Philadelphia, PA Lea and Febiger 4491978 https://search.worldcat.org/title/Histologic-diagnosis-of-inflammatory-skin-diseases-:-a-method-of-pattern-analysis/oclc/612298750
- 3Rheumatoid neutrophilic dermatitis: a case report and review of the literature J Eur Acad Dermatol Venereol Clin Pract Scotti B Misciali C Merli Y Bardazzi F Abbenante D Dika E Piraccini BM 1364138042024
- 4Rheumatoid neutrophilic dermatitis J Cutan Pathol Lowe L Kornfeld B Clayman J Golitz LE 4853191992155626610.1111/j.1600-0560.1992.tb 01558.x · doi ↗ · pubmed ↗
- 5Rheumatoid arthritis: a review of the cutaneous manifestations J Am Acad Dermatol Sayah A English JC 3rd 19125320051602111110.1016/j.jaad.2004.07.023 · doi ↗ · pubmed ↗
- 6Patients with seronegative RA have more inflammatory activity compared with patients with seropositive RA in an inception cohort of DMARD-naïve patients classified according to the 2010 ACR/EULAR criteria Ann Rheum Dis Nordberg LB Lillegraven S Lie E 3413457620172709444410.1136/annrheumdis-2015-208873 · doi ↗ · pubmed ↗
- 7Rheumatoid neutrophilic dermatitis in a patient taking tocilizumab for treatment of rheumatoid arthritis J Dermatol Kubota N Ito M Sakauchi M Kobayashi K 0144201710.1111/1346-8138.1382428342172 · doi ↗ · pubmed ↗
- 8Rheumatoid neutrophilic dermatosis under treatment with the interleukin-6-receptor-antagonist sarilumab in a patient with seropositive rheumatoid arthritis J Cutan Pathol Jost M Schwarz T Wehkamp U Bohne AS Drerup K 7347385020233697515810.1111/cup.14425 · doi ↗ · pubmed ↗