Surgical Outcomes of the Boat-Form Vein Cuff Technique in Peripheral Artery Bypass Grafting
Shun-Ichiro Sakamoto, Anna Tsuji, Motohiro Maeda, Atsushi Hiromoto, Kenji Suzuki, Jiro Honda, Yosuke Ishii

TL;DR
This paper evaluates a new boat-form vein cuff technique in peripheral artery bypass grafting surgeries and reports positive outcomes.
Contribution
The boat-form vein cuff technique is introduced as a versatile and adjustable method for peripheral artery bypass grafting.
Findings
No operative deaths or serious complications were observed in 10 patients using the boat-form vein cuff.
The PTFE graft remained patent in 9 out of 10 patients during a follow-up period of about 3.7 years.
One patient experienced femoropopliteal bypass graft occlusion three months post-surgery.
Abstract
Objectives: The venous cuff technique has been used primarily for arterial bypass using artificial grafts to the lower extremities. The boat-form vein cuff was designed to allow adjustment of the size and angle of the anastomosis at any anatomic site. We report our experience and outcomes of the original vein cuff technique in various peripheral artery bypass grafting procedures. Methods: A total of 10 patients underwent arterial bypass grafting using a polytetrafluoroethylene (PTFE) graft with a boat-form venous cuff. The indications for the surgery consisted of peripheral artery disease (n = 4), acute limb ischemia (n = 4), chronic mesenteric ischemia (n = 1), and traumatic upper limb ischemia (n = 1). Five patients required emergency surgery. Surgical outcomes, such as mortality and morbidity, limb salvage rate, and graft patency, were examined using perioperative and postoperative…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
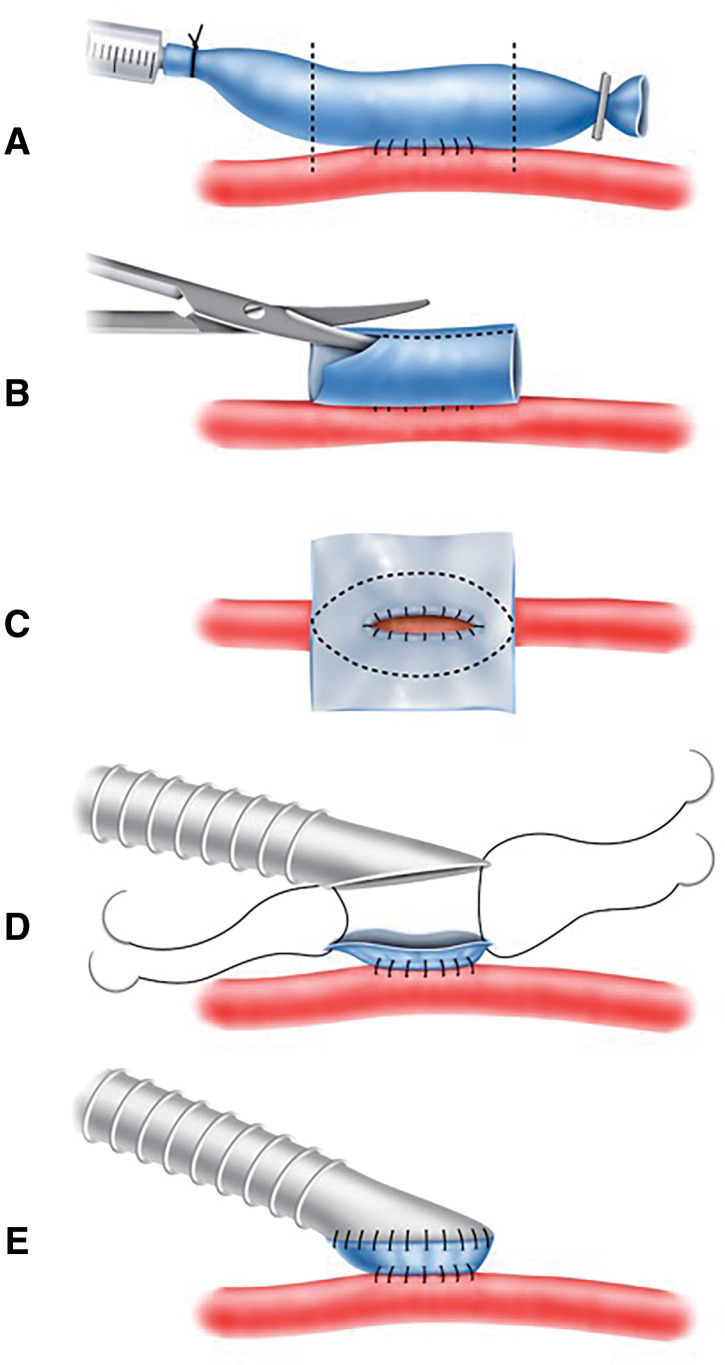 Figure 1
Figure 1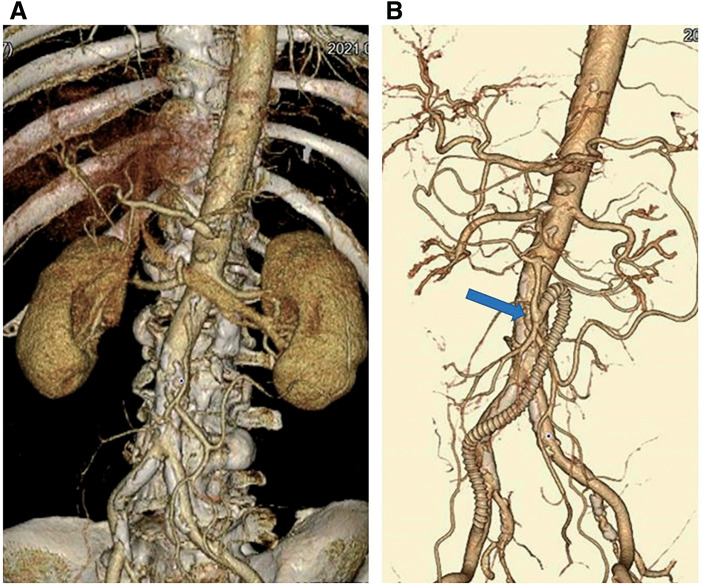 Figure 2
Figure 2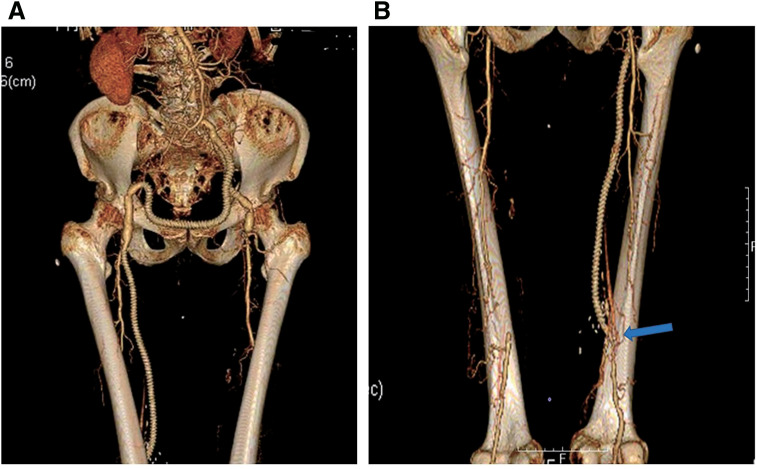 Figure 3
Figure 3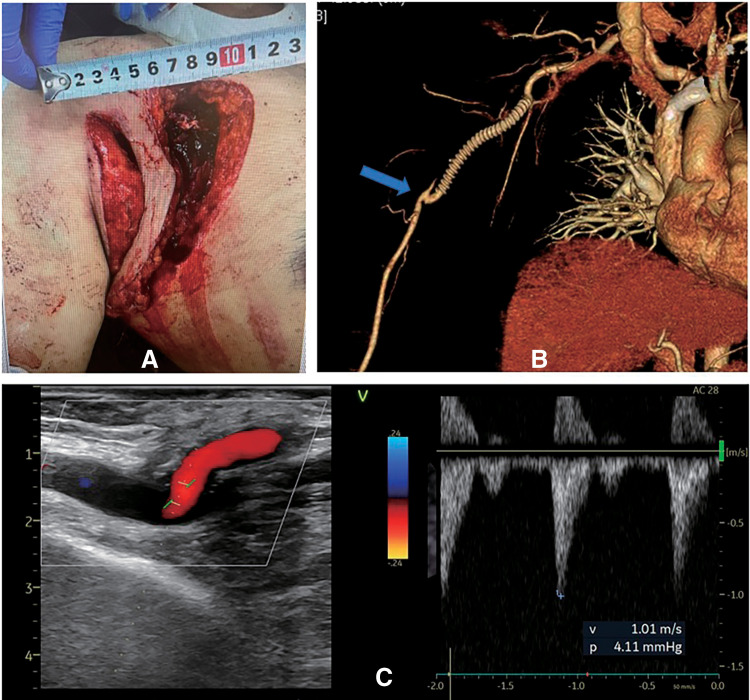 Figure 4
Figure 4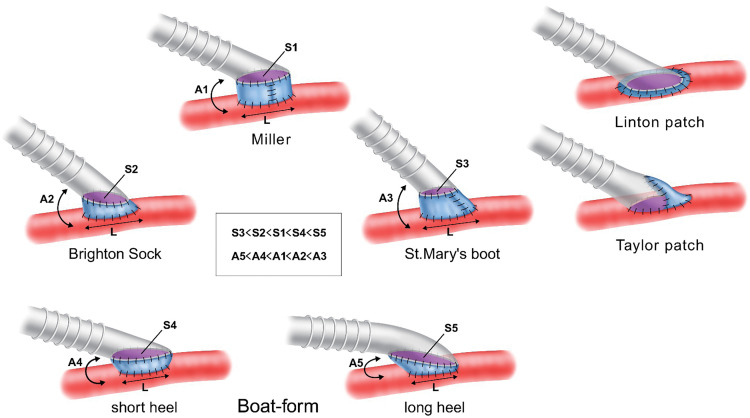 Figure 5
Figure 5| Case | Sex | Age | Diseases | Elective or emergency | Procedures |
|---|---|---|---|---|---|
| 1 | M | 70 | PAD | Elective | BK F-P bypass |
| 2 | M | 75 | PAD | Elective | BK F-P bypass |
| 3 | M | 66 | CMI | Elective | Division of MAL, CIA-SMA bypass |
| 4 | M | 66 | PAD | Elective | EA of Lt EIA and PA, Lt BK F-P bypass |
| 5 | M | 81 | ALI | Emergent | Lt CIA-EIA bypass, EA of Lt EIA, |
| 6 | F | 64 | ALI | Emergent | Rt EIA-Lt EIA bypass, EA of Lt CFA, Lt AK F-P bypass |
| 7 | F | 90 | ALI | Emergent | Lt EIA-Rt CFA bypass, Rt BK F-P bypass |
| 8 | F | 77 | ALI | Emergent | BK F-P bypass, thrombectomy |
| 9 | M | 73 | PAD | Elective | BK F-P bypass |
| 10 | M | 59 | Trauma | Emergent | Axillobrachial artery bypass |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Artery Disease Management · Vascular Procedures and Complications · Aortic aneurysm repair treatments
Introduction
More than 40 years have passed since the venous cuff technique was introduced by Miller. Since then, several variations of the technique have been reported.^1–5)^ Bypass grafting to peripheral arteries with a prosthetic graft using a vein cuff is often used in cases where autologous vein grafts cannot be used, the diameter of the anastomotic vessel is small, or the wall properties of the anastomotic vessel are poor. Advantages of the venous cuff technique include avoiding direct anastomosis between a prosthetic graft and a vessel with an atherosclerotic lesion, forming a large anastomotic opening, and preventing turbulent flow and intimal hyperplasia by increasing the shear stress on the toe and heel of the anastomotic site through the cuff-induced central vortex.^6,7)^ On the other hand, conventional venous cuffs use collar sutures or partial patch formation to create a defined anastomotic opening, making it difficult to adjust the shape and length of the anastomotic opening when suturing an artificial blood vessel. We have previously reported on the boat-form vein cuff technique, in which a vein anastomosed to an artery using the side-to-side technique is trimmed into a boat shape.^8)^ The boat-form technique is easy to perform, has the advantage that the anastomotic opening and angle of the graft and vein can be adjusted as needed, and is expected to be suitable for peripheral vascular surgery at all anatomic sites. Herein, we aimed to report a single center’s experience with the boat-form vein cuff and the surgical outcomes.
This study was performed in accordance with the guidelines of the Declaration of Helsinki and was approved by the Ethics Committee of Nippon Medical School Musashikosugi Hospital in Kanagawa, Japan (No. 734-5-45, 2023).^9)^
Materials and Methods
A total of 10 patients have undergone peripheral vascular surgery using a polytetrafluoroethylene (PTFE) graft with a boat-form vein cuff in the 9 years since the boat-form vein cuff technique was first used for a femoropopliteal (F-P) artery bypass in 2014.^1)^ The mean age was 71 ± 10.1 years, and 7 (70%) were male. All patients had hyperlipidemia as a risk factor for atherosclerosis, and 3 were current smokers. Eight patients had Trans-Atlantic Inter-Society Consensus Class D aortoiliac or F-P occlusive disease,^10)^ and 4 of them required emergency surgery for the development of acute limb ischemia.
It is the institutional policy to use autologous veins, primarily the great saphenous vein, as the first choice for arterial bypass surgery, but PTFE grafts were used in patients for whom appropriate autologous veins could not be obtained, such as those with varicose veins in the lower extremities or when the great saphenous vein had already been used in coronary artery bypass surgery. PTFE grafts were also used in patients in whom an autologous vein could be obtained, but who had anatomic obstruction factors such as anastomotic compression or graft flexion, or who required emergency revascularization due to acute limb ischemia. The venous cuff technique was used only when the diameter of the peripheral artery was significantly smaller than the PTFE graft and an atherosclerotic lesion was observed grossly at the anastomotic opening.
In the first 5 patients in our study, a 7-cm vein was harvested and the dilated vein was marked in a boat form with a pen and then trimmed.^1)^ However, more recently, the vein was separated at both ends, followed by a longitudinal incision to expose the intimal surface. Thereafter, the vein was trimmed to match the anastomotic design of the PTFE graft (Fig. 1). In this case group, a 6-mm PTFE graft was used for all patients, with the length of the arteriotomy incision set at 12 mm and the length of the PTFE anastomosis adjusted to 15–20 mm on the heel side. The vein cuff was created using the great saphenous vein in 3 patients and the collateral saphenous vein in 7 patients. Emergency surgery was performed for acute lower limb ischemia in 4 patients and for traumatic upper limb ischemia due to an axillary laceration in 1 patient. The vein cuff was also used in a superior mesenteric artery bypass for the treatment of mesenteric ischemia in 1 patient.^11)^ Although multiple procedures were performed during the surgeries of 6 patients, the vein cuff was created for a distal anastomosis and a 6-mm PTFE graft was used for the peripheral arterial bypass in all patients.
Fig. 1 Illustration of the creation of a boat-form vein cuff. (A) Side-to-side anastomosis between the vein and artery. The dotted line indicates the resection line of the vein. (B) Longitudinal incision of the vein. (C) Trimming of the vein in accordance with the anastomosis diameter and angle of the PTFE graft. (D) Sutures are applied to both ends of the PTFE graft and vein cuff. (E) Completed boat-form vein cuff anastomosis. PTFE: polytetrafluoroethylene
All patients were administered an antiplatelet agent, and warfarin was used only for the 1st year after the operation with a target prothrombin time-international normalized ratio of 1.5–2. The patients were followed up regularly in the outpatient clinic after surgery. The first contrast-enhanced computed tomography (CT) was obtained 6 and 12 months after surgery. Thereafter, if the patient did not exhibit any ischemic symptoms, the ankle–brachial index and/or CT was obtained once a year to confirm graft patency.
Results
Table 1 shows the patients' characteristics and vascular surgeries in which the boat-form vein cuff technique was used. The mean operative time was 289 ± 102 minutes. The treatment of chronic mesenteric ischemia (Patient 3) required multiple procedures, including ilio-superior mesenteric artery bypass with a venous cuff, division of the median arcuate ligament, and angioplasty of the celiac artery, which were performed in collaboration with physicians from other departments (Fig. 2). The most time-consuming surgery was performed in Patient 5, in whom 3 bypasses were created from the inflow site to the peripheral anastomosis, in addition to an endarterectomy of the external iliac and common femoral arteries. The operative time was 555 minutes (Fig. 3). Among the emergency surgeries for acute ischemia of the lower extremity, 2-compartment fasciotomy was performed in 3 patients (Patients 5, 6, and 7) for acute compartment syndrome that developed due to postoperative revascularization. In Patient 6, a postoperative CT revealed local necrosis of the gastrocnemius muscle, and the mean blood creatine phosphokinase (CPK) level was 3216 ± 4387.8. The CPK level was the highest in Patient 7, with a maximum CPK value of 9000 U/L immediately after surgery. Thus, continuous hemodialysis was performed for 4 days. Skin grafting was performed to the relaxed skin tension lines on postoperative day 15 in Patient 7. In the patient with a traumatic brachial artery injury (Patient 10), the artery was initially reconstructed in the emergency room using an autologous vein. However, after closure of the wound, the graft became bent and occluded. Thus, the patient was immediately transferred to the operating room for bypass using a PTFE graft (Fig. 4).
**:
Fig. 2 Superior mesenteric artery bypass for the treatment of chronic mesenteric ischemia (Patient 3). (A) 3D reconstruction of preoperatively obtained CT. (B) 3D reconstruction of postoperatively obtained CT showing an intact graft and SMA. The blue arrow indicates the site of the vein cuff. 3D: three-dimensional; CT: computed tomography; SMA: superior mesenteric artery
Fig. 3 An emergency case of above knee F-P bypass and multiple inflow procedures for the treatment of acute limb ischemia (Patient 5). (A) 3D reconstruction of postoperatively obtained CT showing a patent PTFE graft for a left EIA-CFA bypass and left CFA-right CFA bypass. (B) 3D reconstructed posterior view of a PTFE graft above the right knee for an F-P bypass. The blue arrow indicates the site of the vein cuff. 3D: three-dimensional; CFA: common femoral artery; CT: computed tomography; EIA: external iliac artery; F-P: femoropopliteal; PTFE: polytetrafluoroethylene
Fig. 4 A case of axillobrachial artery bypass for traumatic obstruction of the brachial artery (Patient 10). (A) A 59-year-old man fell from a height, resulting in an axillary laceration and an arteriovenous injury. Axillobrachial artery bypass was performed using a 6-mm PTFE graft. (B) 3D reconstruction of postoperatively obtained computed tomography image showing the site of the vein cuff (blue arrow). (C) Color Doppler of the vein cuff showing a patent graft, absence of significant stenosis, and high-speed turbulent flow. PTFE: polytetrafluoroethylene
There were no operative deaths or serious complications, such as amputation of the upper or lower extremities, in our study. Postoperative contrast-enhanced CT showed that the graft was patent in all patients. All upper and lower limbs were preserved, and 5 patients were transferred to postoperative rehabilitation facilities. During the postoperative follow-up period (44 ± 36.9 months), the PTFE graft remained patent in 9 patients (90%). One patient (Patient 3) developed occlusion of the F-P bypass graft at 3 months postoperatively.
Discussion
Artificial grafts are inferior to autologous veins in terms of patency of the bypass to the popliteal artery.^12)^ To overcome this challenge, Miller developed the venous cuff technique, in which a vein is inserted between the graft and the artery. Randomized studies have demonstrated that the venous cuff technique may improve graft patency.^13,14)^ However, the creation of collared venous cuffs, such as the Miller cuff and Saint Mary’s boot, is not technically easy and can result in cross sutures between the longitudinal suture of the cuff and the arterial wall or PTFE graft.^1,2)^ The venous cuff using the Brighton method and the venous patch using the Linton method do not include the longitudinal suture, which is a drawback of the collared cuff. However, the size of the anastomosis is determined by the length of the arteriotomy incision, so the size cannot be adjusted according to the suture angle of the PTFE graft.^3,4)^ The Taylor method requires direct suturing of the graft to the artery, reducing the benefits of the cuff.^5)^ The boat-form vein cuff has the largest anastomosis size per length of arteriotomy when compared with the other vein cuff methods. Furthermore, the graft can be freely trimmed, and the anastomotic angle can be adjusted by changing the cuff’s shape (Fig. 5). The hemostatic state of the cuff can be easily checked without crossing sutures during cuff creation. Thus, the cuff can be created according to the surgical field, and peripheral vascular surgery can be easily performed at any anatomical site.
Fig. 5 Vein cuff and venous patch techniques. The anastomotic size of the vein cuff at the arterial incision length is the largest in the boat-form vein cuff and the smallest in the St. Mary’s boot vein. However, the anastomotic angle of a prosthetic graft with vein cuff decreases as the anastomosis size increases. The boat-form vein cuff has the largest angle among the 4 vein cuffs. The boat-form vein cuff differs from other vein cuffs in that the anastomosis size and angle can be adjusted by changing the length of the heel portion of the cuff. A: anastomotic angle between prosthetic graft and target artery; L: length of arteriotomy; S: anastomotic size of prosthetic graft
In our study, PTFE grafts were used in 4 emergency operations despite the availability of vein grafts. These grafts may have been used to reduce the time spent harvesting autologous veins and because the interposition of a vein cuff produces better results than PTFE alone when bypassing the popliteal artery below the knee.^15)^ Furthermore, the boat-form vein cuff is easy to create, especially in patients in whom the inflow procedure requires time. For example, in Patients 5 and 6, it was possible to simultaneously create the vein cuff and perform inflow procedures by securing a separate operative field. All emergency surgeries, including those performed in Patients 5 and 6, were performed for Rutherford Class IIB acute limb ischemia that developed due to native artery occlusion and critical limb ischemia.^16)^ Although postoperative reperfusion injury developed in 3 of these patients (75%), limb salvage was achieved in all 4 patients. Guntani et al. reported a high limb salvage rate despite a low long-term patency rate in their study.^17)^ They speculated that the high limb salvage rate may be due to an adequate supply of direct blood flow. In our study as well, the boat-form cuff technique may have been useful in terms of time-to-reperfusion and ensuring blood flow.
In the present study, PTFE bypass with a boat-form vein cuff was performed to the brachial artery and superior mesenteric artery (SMA) in addition to revascularization of the lower extremity. Direct anastomosis of the prosthetic graft to these arteries was avoided only because of a caliber mismatch with the PTFE. PTFE graft bypass to the brachial artery has been reported in several cases, primarily for the treatment of brachial artery aneurysms.^18)^ In a review of 49 patients with this condition, the PTFE graft was used in 9 patients (18%), and all peripheral anastomoses were direct anastomoses without a venous cuff. In the upper arm, where subcutaneous fat is limited, autologous veins are usually used to avoid infection. In Patient 10 in our study, venous grafting would have been preferred due to the trauma and contamination. However, due to the long graft length and the compression caused by the residual subcutaneous hematoma, we had to use a PTFE graft. The PTFE graft is frequently used for SMA bypass in chronic mesenteric ischemia because a 4-mm or longer autologous vein is required, which may kink depending on the bypass length.^19)^ Furthermore, the incidence of graft failure in the early postoperative period is reported to be less than half that of autologous venous bypass.^20)^ In Patient 3 in our study, we performed a C-loop retrograde PTFE graft bypass with iliac artery inflow. Although several similar revascularization procedures have been reported, none have used a venous cuff for mesenteric artery bypass.^21)^ Because of the good clinical course and graft blood flow after revascularization of both brachial and mesenteric arteries, PTFE bypass using a boat-form vein cuff may be used for all peripheral arterial revascularization procedures, not only for arterial diseases of the lower extremities.
This study had some limitations. Because autologous veins or PTFE grafts are always used alone as grafts in peripheral artery bypass surgery, venous cuffs are used in very few cases. Furthermore, the study was conducted at a single institution. To overcome these limitations, further multicenter studies are required to compare the outcomes of treatment with and without the use of the boat-form vein cuff.
The boat-form vein cuff has a large anastomotic opening due to the outwardly warped cuff edge, which facilitates anastomosis with the PTFE graft. Thus, it may be useful in cases where the operative field is deep and narrow. On the other hand, the results of the present study do not indicate that the boat-form vein cuff is superior to other vein cuffs. Previous studies have used computer models to analyze the anastomotic blood flow patterns and wall shear stress distribution in end-to-end anastomosis using venous cuffs.^22,23)^ In the future, similar analyses will be required to compare the blood flow pattern in a boat-form vein cuff, a Miller cuff, other vein cuffs, and precuffed PTFE grafts.^24,25)^
Conclusion
The simple design and creation of the boat-form vein cuff are useful at any anatomical site in peripheral artery bypass grafting with a PTFE graft.
Declarations
Acknowledgments
We acknowledge the excellent assistance of Masako Izumi in preparing the manuscript.
Disclosure statement
The authors do not have any conflicts of interest to declare.
Author contributions
Study conception: SS, JH
Data collection: SS, MM, AT, AH
Analysis: SS
Investigation: MM, SS, KS, JH
Funding acquisition: none
Manuscript preparation: SS, MM, YI
Critical review and revision: all authors
Final approval of the article: all authors
Accountability for all aspects of the work: all authors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Miller JH, Foreman RK, Ferguson L, et al. Interposition vein cuff for anastomosis of prostheses to small arteries. Aust N Z J Surg 1984; 54: 283–5.6380479 10.1111/j.1445-2197.1984.tb 05318.x · doi ↗ · pubmed ↗
- 2Tyrrell MR, Wolfe JHN. New prosthetic venous collar anastomotic technique: combining the best of other procedures. Br J Surg 1991; 78: 1016–7.1913097 10.1002/bjs.1800780840 · doi ↗ · pubmed ↗
- 3Nash TM, Elahwal M, Edwards M. Adaptation of the vein cuff in distal arterial anastomosis (Brighton Sock). Ann R Coll Surg Engl 2021; 103: 537–8.34192499 10.1308/rcsann.2021.0010 PMC 10334982 · doi ↗ · pubmed ↗
- 4Batson RC, Sottiurai VS, Craighead CC. Linton patch angioplasty. An adjunct to distal bypass with polytetrafluoroethylene grafts. Ann Surg 1984; 199: 684–93.6375593 10.1097/00000658-198406000-00006 PMC 1353446 · doi ↗ · pubmed ↗
- 5Taylor RS, Loh A, Mc Farland RJ, et al. Improved technique for polytetrafluoroethylene bypass grafting: long-term results using anastomotic vein patches. Br J Surg 1992; 79: 348–54.1576506 10.1002/bjs.1800790424 · doi ↗ · pubmed ↗
- 6Kissin M, Kansal N, Pappas PJ, et al. Vein interposition cuffs decrease the intimal hyperplastic response of polytetrafluoroethylene bypass grafts. J Vasc Surg 2000; 31: 69–83.10642710 10.1016/s 0741-5214(00)70069-3 · doi ↗ · pubmed ↗
- 7How TV, Rowe CS, Gilling-Smith GL, et al. Interposition vein cuff anastomosis alters wall shear stress distribution in the recipient artery. J Vasc Surg 2000; 31: 1008–17.10805893 10.1067/mva.2000.105961 · doi ↗ · pubmed ↗
- 8Sakamoto SI, Shibata M, Takahashi KI, et al. A novel method of vein cuff creation for below-knee femoropopliteal bypass with a prosthetic graft. J Vasc Surg Cases Innov Tech 2020; 6: 165–7.32322767 10.1016/j.jvscit.2020.02.002PMC 7160380 · doi ↗ · pubmed ↗