Penile Metastasis as the Presenting Symptom of Colorectal Carcinoma: A Rare Case Report
Mann Patel, Alain Kaldany, Farida Tanko, Andrew Parrott, Thomas L. Jang

TL;DR
A rare case of penile metastasis from colorectal cancer presented as the first symptom, with no known primary tumor and ongoing treatment.
Contribution
This case report highlights an isolated penile metastasis as the initial presentation of colorectal adenocarcinoma without a detectable primary tumor.
Findings
Penile metastasis was the first sign of colorectal cancer in a patient with no prior malignancy.
Diagnostic imaging and colonoscopy failed to identify a primary colorectal tumor.
The patient is undergoing chemotherapy with no adverse effects and possible improved prognosis.
Abstract
Background: Secondary penile cancer, despite the region's rich vascularization, is a rare phenomenon with only around 500 cases ever reported, typically of genitourinary origin and in even rarer cases, of colorectal adenocarcinoma. Unfortunately, the underlying mechanisms are not well elucidated, and prognosis remains poor with a late onset and median overall survival of 9 months for colon adenocarcinoma. Secondary penile cancer often presents alongside concurrent metastases months or years following successful treatment of the primary tumor. However, we report a case of an isolated penile metastasis as the presenting symptom of colon adenocarcinoma with no identifiable primary lesion or history of malignancy. Case Summary: A 67-year-old African-American male presented with a 1-month history of voiding symptoms, whereupon follow-up revealed a penile mass near the left base of the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
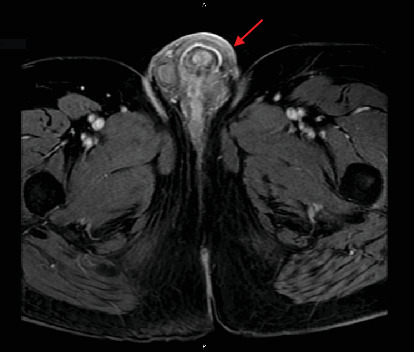 Figure 1
Figure 1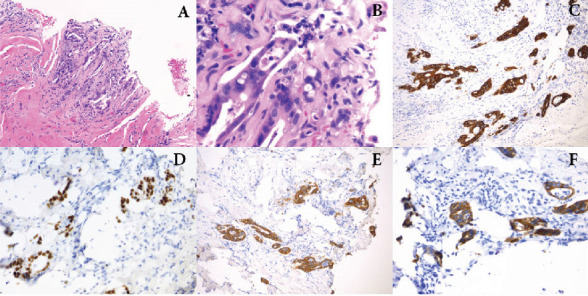 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenital Health and Disease · Cancer Diagnosis and Treatment · Urological Disorders and Treatments
1. Introduction
Penile metastasis, alternately referred to as secondary penile cancer, is a rare phenomenon, with only around 500 cases reported since 1870 [1]. The most common sites that metastasize to the penis include the bladder and prostate, with the lower gastrointestinal tract making up only around 80 cases in the literature [1, 2]. The typical age of onset of penile metastasis ranges from 60 to 80 years, mirroring the age of onset of the primary malignancy [1, 2]. Patients often present with obstructive symptoms including voiding difficulties, as well as penile or perineal pain [1–5].
Though it is rare, secondary penile cancer is often lethal, as it indicates worsened and disseminated primary disease [1, 2, 4]. In cases of rectal carcinoma metastatic to the penis, studies report an average overall survival of only 7 months, with patients presenting an average of 37 months following successful treatment of the initial disease [4]. Penile metastases from the colon are even fewer in number, despite colorectal cancer being the third most common cancer diagnosis and the second leading cause of cancer-related death in the United States (US) [3, 6]. While roughly one-half of patients with colorectal cancer will eventually develop disseminated disease, the typical sites of metastasis are the liver, thorax, and peritoneum [6, 7]. Interestingly, however, despite its relative proximity and extensive vascularity, penile metastasis of colorectal cancer remains a rare phenomenon [1, 2].
In most cases, secondary penile cancer presents alongside systemic metastases, which often appear months or years following successful treatment of the primary tumor [1–5, 8]. However, here, we report an unusual case of isolated penile metastasis as the initial presenting symptom of colon adenocarcinoma in the absence of a known primary colorectal lesion [3, 9, 10].
2. Case Presentation
A 67-year-old African-American male with a past medical history of HIV managed with highly active antiretroviral therapy, benign prostatic hyperplasia, erectile dysfunction, and recurrent urethral stricture disease presented with a 1-month history of voiding symptoms associated with minimal pain. The examination was notable for a firm, nontender nodularity near the left base of the penis without associated skin changes. Cystoscopy revealed dense bulbar and proximal penile urethral stricture near the palpable penile mass. Magnetic resonance imaging (MRI) of the pelvis revealed a heterogeneously enhancing lesion measuring 3.7 by 3.6 cm near the left penile base (Figure 1). The patient was then taken to the operating room for excisional biopsy of the penile mass, which grossly measured 0.7 × 0.6 × 0.3 cm.
Histopathological analysis of the lesion revealed characteristics of invasive adenocarcinoma, and immunohistochemical testing was compatible with metastatic colorectal adenocarcinoma. Specifically, the tissue was positive for pancytokeratin, CK20, CDX-2, and CK7, and negative for GATA-3, p63, CMV, GMS, and HSV2 virus (Figure 2).
Further diagnostic testing was notable for elevations in serum tumor markers CA 19-9 (127.6 U/mL, normal 0.6–55.0 U/mL) and carcinoembryonic antigen (33.05 ng/mL, normal 0–3 ng/mL) and whole body PET/CT scan revealed multiple subcentimeter pulmonary nodules, but no colonic abnormalities. Hypermetabolic activity was noted near the base of the penis and in several subcentimeter inguinal lymph nodes bilaterally. A colonoscopy was performed, showing several areas of ulceration and focally congested mucosa within the cecum and rectum, respectively; however, the biopsy of these sites was negative for malignancy. No apparent polyps or other lesions were identified. Genomic analysis with Guardant360 (Guardant Health, Redwood City, CA) and FoundationOne (Foundation Medicine, Cambridge, MA) revealed mutations in KRAS, SMAD4, and TP53, with equivocal microsatellite instability and indeterminate tumor mutational burden.
Despite the absence of a primary colorectal lesion, the patient was started on chemotherapy with a modified FOLFOX-6 regimen (mFOLFOX-6; oxaliplatin with 5-fluorouracil and folinic acid) and has since completed treatment in full. Of note, the patient experienced refractory upper extremity neuropathy, and oxaliplatin dose was adjusted accordingly.
Follow-up CT imaging prior to the 12th cycle revealed the persistence of previously noted hypermetabolic activity in several subcentimeter inguinal lymph nodes bilaterally, as well as prominent bilateral axillary lymph nodes with FDG avidity and two foci of FDG avidity within the penis likely corresponding to metastatic disease. Given this concern for residual disease, the patient is planned to initiate radiation therapy to the pelvis.
3. Discussion
Secondary penile cancer of any origin is a rare phenomenon. Most cases of colorectal adenocarcinoma are accompanied by metastases to the lungs, liver, and/or pelvis and appear years after a successful initial treatment [1–3]. The prognosis for metastatic colorectal adenocarcinoma is generally poor, with a median overall survival ranging from 11 to 30 months depending on the tumor's profile [11, 12]. However, due to the rarity of secondary penile cancers, particularly those originating from colorectal cancer, survival outcomes are less well-defined. For metastatic cancer to the penis, the average overall survival is shorter, ranging from 9 to 14 months [5, 13, 14]. Further, most penile metastases from colorectal magnicides stem specifically from rectal carcinoma, while metastasis from colonic masses is less frequent, with only 10 reported cases since 1952 [3, 8, 15].
Although rare, prior case reports of colorectal metastases to the penis have been documented [4]. The majority of these cases involve patients with a known history of previously diagnosed and/or treated colorectal carcinoma with now metachronous penile metastases, often with multiple other sites of metastases [4, 8, 16–20]. However, in fewer instances, penile metastasis has been reported as the initial presenting symptom of metastatic colorectal cancer, often occurring alongside other systemic metastases and with an identifiable primary malignancy on workup [4, 9, 10, 21].
Here, we present a unique case of an isolated penile metastasis as the initial symptom of colon adenocarcinoma without a history of previous malignancy. Not only is an isolated penile metastasis as the initial presenting symptom of colorectal cancer an extremely rare manifestation, but to our knowledge, this is also the first such reported case in the literature without an identifiable primary colonic mass.
4. Proposed Theories of Dissemination
Given its rarity, the mechanism of penile metastasis has yet to be elucidated. In 1956, Paquin and Roland posited numerous theories including retrograde venous, lymphatic, or arterial spread, and, less likely, direct growth of tumor into adjacent organs or implantation [22]. Among these, retrograde venous flow is thought to represent the most likely mechanism [1, 2, 22].
Specifically, blood from the cavernous spaces of the penis drains through vessels that converge into the deep dorsal vein or pass through the base of the penis to join the prostatic plexus [1, 2, 18]. These venous networks communicate with the pudendal, vesical, vertebral, and hemorrhoidal plexuses, allowing for a connection between the dorsal venous system of the penis and venous plexuses of the pelvic organs. Consequently, a reversal of blood flow, possibly by tumor obstruction, could lead to tumor spread to the penis [1, 2, 18]. In fact, such retrograde flow may explain why most secondary penile lesions affect the corpora cavernosa and glans [1]. Conversely, metastasis to the penis via arterial spread is likely uncommon, possibly occurring through the internal pudendal and iliac arteries, either by direct tumor extension into the arterial pathways or from metastatic tumor emboli [1–4, 22].
Another commonly proposed theory involves retrograde lymphatic spread, which occurs similarly to retrograde venous flow [1, 22]. The superficial inguinal nodes drain the skin of the penis, while lymphatics from the glans and corpora cavernosa drain into either superficial or deep nodes. In the pelvic region, the lower rectum drains through the perineum into the inguinal and iliac nodes [1, 2, 18]. The proximity of these lymphatic networks allows for a potential connection between the penile and pelvic regions and may explain resulting secondary lesions to the penile skin [2].
5. Detection and Treatment
Secondary penile cancer varies in presentation, but 60% report symptoms related to the presence of nodules which often involve both corpora cavernosa [1, 2]. These nodular symptoms include lower urinary tract symptoms, priapism, skin lesions, and penile and/or perineal pain in advanced cases [1–5]. In our case, the tumor presented as a unilateral mass and urethral stricture with urinary symptoms. As these symptoms are somewhat nonspecific, the etiology must be clarified in order to differentiate malignancy from benign penile lesions, infectious causes, and other benign conditions such as Peyronie's disease [1–3].
Biopsy or corporal aspiration is the standard of diagnosis to differentiate between metastasis and primary penile cancer [1, 2]. In the case of penile metastasis, a pathological assessment with immunohistochemistry is integral to determining the primary site, particularly in cases with no prior history of malignancy or an identifiable primary lesion [3, 8]. Supplementary imaging includes ultrasonography, CT, and/or MRI for staging and detection of other metastatic sites, and adjunctive genomic testing can be performed to identify mutational profiles for precision medicine [1, 2, 23].
The management of penile metastasis is dependent on the site of the primary lesion, the degree of additional metastatic burden, and the severity of symptoms [2]. As the presence of a penile metastasis typically underlies advanced or end-stage primary disease with a poor prognosis, treatment is often palliative. Treatment modalities include chemotherapy, radiotherapy, palliative care, and surgical excision including penectomy [4]. In this case, the patient underwent therapeutic systemic chemotherapy with mFOLFOX-6, with successful resolution of his urinary symptoms, though the patient did experience persistent neuropathy of the hands, a common side effect of oxaliplatin [24].
Unlike most previously reported cases, our patient had no symptoms of colorectal disease, no identifiable primary colorectal lesion, and no other identifiable metastatic lesions. Our patient also lacked significant penile or cutaneous involvement that would warrant aggressive surgical treatment and was instead managed with excisional biopsy followed by systemic chemotherapy and pelvic radiotherapy. Still, such an initial presentation may suggest a more favorable prognosis than has previously been described. Close surveillance via serum tumor markers (CEA and CA 19-9), cross-sectional imaging, and colonoscopy will be imperative as treatment continues.
6. Conclusion
Although rare, secondary penile cancer should be considered in patients with relevant genitourinary symptoms, particularly in cases with a history of underlying malignancy. Here, we describe a rare case of isolated penile metastasis as the initial manifestation of colorectal adenocarcinoma with no identifiable primary mass. While current literature suggests poor prognosis and palliative management for penile metastasis, the unique and relatively indolent presentation of this patient may portend a more favorable outcome, although optimal treatment and accurate prognosis remain unclear.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mearini L. Colella R. Zucchi A. Nunzi E. Porrozzi C. Porena M. A Review of Penile Metastasis Oncology Reviews 201261 e 1010.4081/oncol.2012.e 102-s 2.0-8487865194525992200 PMC 4419641 · doi ↗ · pubmed ↗
- 2Cherian J. Rajan S. Thwaini A. Elmasry Y. Shah T. Puri R. Secondary Penile Tumours Revisited International Seminars in Surgical Oncology 200631 p. 3310.1186/1477-7800-3-332-s 2.0-3375041170817032461 PMC 1618838 · doi ↗ · pubmed ↗
- 3Yin G. L. Zhu J. B. Fu C. L. Ding R. L. Zhang J. M. Lin Q. Metachronous Isolated Penile Metastasis From Sigmoid Colon Adenocarcinoma: A Case Report World Journal of Clinical Cases 20221031116581166410.12998/wjcc.v 10.i 31.1165836387791 PMC 9649525 · doi ↗ · pubmed ↗
- 4Kuliavas J. Dulskas A. Drachneris J. Miseikyte-Kaubriene E. Samalavicius N. E. Penile Metastasis From Rectal Carcinoma: Case Report and Review of the Literature Visceral Medicine 201834538939210.1159/0004915942-s 2.0-8505270923130498707 PMC 6257096 · doi ↗ · pubmed ↗
- 5Dong Z. Qin C. Zhang Q. Penile Metastasis of Sigmoid Colon Carcinoma: A Rare Case Report BMC Urology 2015151 p. 2010.1186/s 12894-015-0014-92-s 2.0-84925452564 PMC 437162125887957 · doi ↗ · pubmed ↗
- 6Lotfollahzadeh S. Recio-Boiles A. Cagir B. Colon Cancer 2023 Stat Pearls
- 7Riihimaki M. Hemminki A. Sundquist J. Hemminki K. Patterns of Metastasis in Colon and Rectal Cancer Scientific Reports 2016612976510.1038/srep 297652-s 2.0-8497865350027416752 PMC 4945942 · doi ↗ · pubmed ↗
- 8Triki W. Kacem A. Itami A. Baraket O. Rebai M. H. Bouchoucha S. Penile Metastasis of Colon Carcinoma: A Rare Case Report Urology Case Reports 20192410087510.1016/j.eucr.2019.1008752-s 2.0-8506312697031211084 PMC 6562570 · doi ↗ · pubmed ↗