The Application Value of Early Amplitude-Integrated Electroencephalogram in a Newborn with Nonketotic Hyperglycinemia: A Rare Case Report
Enting Ma, Wei Li, Hong Gao, Shifeng Ma, Qianwen Chai, Li Wei, Jing Wang

TL;DR
This case report explores how amplitude-integrated electroencephalogram (aEEG) can help diagnose and monitor brain activity in a newborn with nonketotic hyperglycinemia.
Contribution
This is the first reported use of aEEG in a newborn with NKH due to AMT gene mutations in the Chinese mainland.
Findings
aEEG detected seizures and a burst–suppression pattern in the newborn with NKH.
The aEEG showed no sleep–wake cycle, indicating severe brain damage.
aEEG provided objective insights despite the absence of observable clinical symptoms.
Abstract
This study aimed to evaluate the application value of amplitude-integrated electroencephalogram (aEEG) findings in a newborn with nonketotic hyperglycinemia (NKH). The clinical data of a neonatal patient with NKH were retrospectively analyzed. In this study, aEEG was first used to assess brain function in NKH due to AMT gene mutations in the Chinese mainland so far. The aEEG assessment was stratified according to its background pattern, sleep–wake cycle (SWC), and seizure activity, which gave more objective and systemic results. Seizures and burst–suppression pattern were detected on the aEEG. The background belonged to discontinuous voltage, and showed discontinuity of cerebral activity in the form of the burst–suppression pattern. The classification of SWC in this record belonged to the “No SWC” category, which meant the child had severe brain damage. A typical neonatal single…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
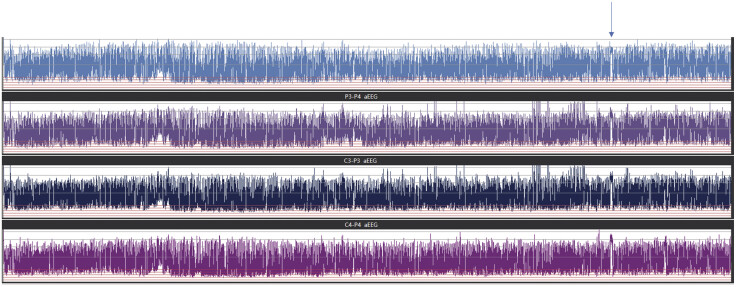 Fig. 1
Fig. 1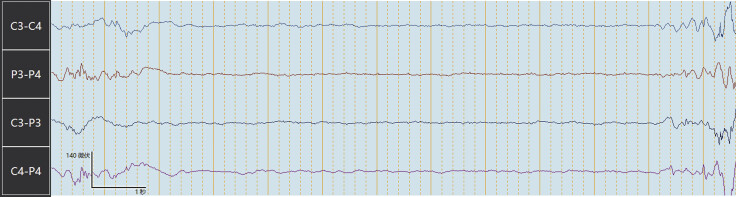 Fig. 2
Fig. 2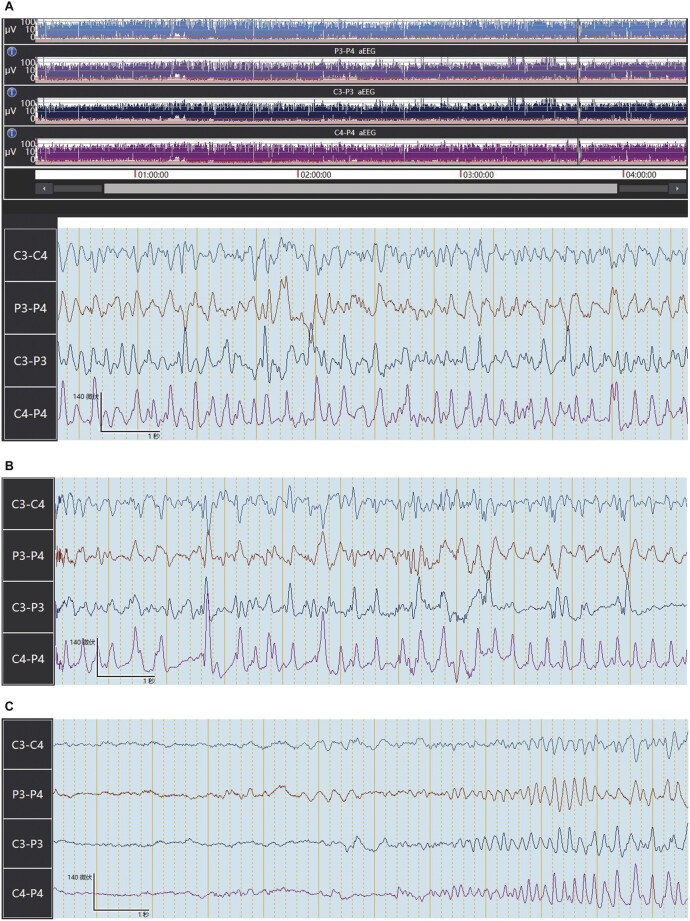 Fig. 3
Fig. 3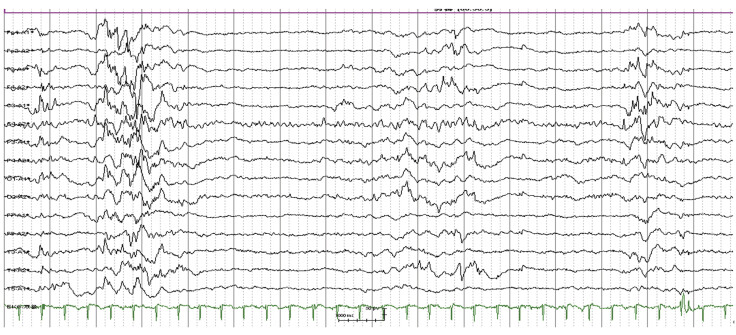 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMetabolism and Genetic Disorders · Neonatal and fetal brain pathology · Hyperglycemia and glycemic control in critically ill and hospitalized patients
Nonketotic hyperglycinemia (NKH; OMIM 605899) is a rare, congenital, and genetic metabolic disease with an estimated prevalence of 1:76,000. 1 It is an autosomal recessive disorder of glycine metabolism resulting in an excessive accumulation of glycine in all body tissues, especially in the central nervous system. 2 3 Mutations mostly occur in the GLDC and AMT genes. 1 There are only a few cases reported in the Chinese mainland so far, and the incidence is still unknown. Furthermore, most cases of NHK are caused by GLDC gene defects in the Chinese mainland. 4 5 6 7 In this study, a Chinese male infant diagnosed with NKH due to AMT gene mutations was the second case reported in the Chinese mainland.
Metabolic disorders are not symptomatic immediately after birth, and they can even manifest slowly with progressive encephalopathy. 8 Thus, accurate diagnostic evaluation of neural function in newborns with a possible metabolic disorder is very important. 9 Early recording of high-risk infants is helpful for the early diagnosis and treatment of seizures.
Amplitude-integrated electroencephalogram (aEEG) has been widely used as a continuous brain-function monitoring tool in neonatal intensive care units (NICUs). 10 11 12 The aEEG has a lot of practical advantages, such as a first-line bedside tool in patients with encephalopathy and/or seizures for longer time periods. Also, the aEEG only uses two channels rather than the multichannel array of a conventional electroencephalogram (EEG). The main features of the aEEG are background activity, presence or absence of sleep–wake cycle (SWC), and specific patterns indicating seizures. 13 aEEG has been used for more than a decade in the evaluation of infants with encephalopathy, there has been no study on the efficacy of aEEG to evaluate neonates with NKH in China.
In this study, aEEG was first used in NKH due to AMT gene mutations in the Chinese mainland. The aEEG assessment was stratified according to its background pattern, SWC, and the presence of electrographic seizures, which gave more objective and systemic results.
Case Report
A 2-day-old male child of the Chinese Han population was born at full term and delivered by cesarean section, with a birth weight of 3.785 kg. The Apgar scores were 9 points at 1 minute and 10 points at 5 minutes, and did not present asphyxia. The patient's parents and sister were all healthy. There was no death of any infant or miscarriage in his family history. The neonate was lethargic since birth with poor feeding and gross hypotonia. Several days later, the child presented a deterioration of consciousness until coma. The respiratory drive developed insufficiently, which required intubation and mechanical ventilation. Blood amino acids showed elevated serum glycine (1,470 μmol/L; normal range 131–368 μmol/L). Urine gas chromatography–mass spectrometry showed increased glycine in urine. Cerebrospinal fluid (CSF) glycine was elevated (215 μmoL/L; normal range 3–10 μmol/L), and the CSF/serum glycine ratio was 0.146 (normal ≤0.02).
At last, considering the lack of effective treatment and poor prognosis of the disease, the patient's parents decided to abandon treatment. The child died on the 21st day after birth.
Amplitude-Integrated Electroencephalogram Recording and Interpretation
The aEEG was recorded by a trained nurse in charge of the infant. The aEEG was recorded as a two-channel EEG using gold caps. Skin was cleaned with alcohol and covered with electrode jelly. Electrodes were placed on the scalp corresponding to the positions C3, P3, C4, and P4 following the International 10–20 System. According to the International 10–20 System, the reference electrode Cz and grounding electrode Fz were also placed on the scalp. The upper limit of tolerated impedance was 20 kΩ. Frequencies lower than 2 Hz or higher than 15 Hz were filtered. The raw EEG data were processed and time-compressed, then displayed on a semilogarithmic scale at a speed of 6 cm/h. During the aEEG recording, video monitoring was also recorded as soon as possible. The quality of the recordings was monitored by continuous impedance tracing and the absence of interference from other electrical devices. The duration of the recordings was at least 4 hours. Handling or routine nursing care periods were marked on the tracing. In addition, the patient's diagnoses and the relevant clinical information were also recorded. The aEEG traces were examined by two investigators. The raw EEG data were also inspected to verify the aEEG assessment. Disagreement was resolved by consulting a third investigator.
In this aEEG recording, the interburst interval varied with a maximum of up to 30 seconds. Seizures and burst–suppression pattern were detected on his EEG, and no cyclic variation of the aEEG background was found ( Fig. 1 ). Seizures were recognized on his EEG, but clinical symptoms were not observed. EEG showed burst–suppression ( Fig. 2 ).
Distribution of aEEG background pattern, seizures (indicated by the arrow), and burst–suppression pattern were detected on his EEG, and no cyclic variation of the aEEG background. aEEG, amplitude-integrated electroencephalogram; EEG, electroencephalogram.
An electroencephalogram showing burst–suppression.
Classification of Amplitude-Integrated Electroencephalogram Background Pattern
According to the criteria described by Hellström-Westas and Rosen, 14 the aEEG background activity include five patterns: (1.) Continuous normal voltage: continuous activity with lower (minimum) amplitude around >5 μV and maximum amplitude >10 μV; (2.) discontinuous voltage (DC): discontinuous background with minimum amplitude variable, but mainly below 5 μV, and maximum amplitude over 10 μV; (3.) burst–suppression: discontinuous background with minimum amplitude without variability at 0–1[2] μV, and bursts with amplitude >25 μV; (4.) continuous low voltage: continuous background pattern of very low voltage (around or below 5 μV); (5.) inactive, flat trace: mainly inactive (isoelectric tracing) background below 3 to 5 μV.
In this study, the background belonged to DC ( Fig. 1 ), and showed discontinuity of cerebral activity in the form of a burst–suppression pattern ( Fig. 2 ). For a normal full-term neonate, the part of the raw EEG should display a continuous background rhythm in quiet sleep stage. But in this study, EEG typically showed a burst–suppression pattern. Interburst interval varied with a maximum of up to 9 seconds. The child had a significantly longer interburst intervals (IBI) than normal full-term neonates, with a maximum of up to 6 seconds, which suggested that the child may have brain injury. 15 Longer IBI than the corresponding gestational age suggested that the child might have brain injury. The IBI period is the time of voltage suppression between two bursts, reflecting the maturity of the brain and the severity of brain injury. The electrocortical background activity with very low-voltage IBI, is associated with adverse outcome in infants. The longer the IBI is prolonged, the more serious the injury to the brain. 16 The IBI measured by EEG is directly related to developmental neurobiology, which is considered important for brain wiring during development. 17 The electrocortical background activity with very low-voltage IBI is associated with adverse outcomes in infants. 16
Classification of Sleep–Wake Cycle
SWC in the aEEG is characterized by smooth sinusoidal variations, mainly in the minimum amplitude. The broader bandwidth represents discontinuous background activity during quiet sleep (trace alternant EEG in term infants), and the narrower bandwidth corresponds to more continuous activity during wakefulness and active sleep. Classification of SWC is as listed. (1.) No SWC: no cyclic variation of the aEEG background. (2.) Imminent/Immature SWC: some, but not fully developed, cyclic variation of the lower amplitude, but not developed as compared with normative gestational age representative data. (3.) Developed SWC: clearly identifiable sinusoidal variations between discontinuous and more continuous background activity with a cycle duration of 20 minutes. 14
SWC is defined as cyclic variations of aEEG background activity. 14 Electrophysiological maturity is intimately connected to the development of SWC. 18 The classification of SWC in this record belongs to “No SWC” ( Fig. 1 ), which means the child had severe brain damage. 15
Seizures
Seizure activity is defined as an abrupt rise of the lower border, usually accompanied by a simultaneous rise of the upper border of the recorded strip, with a simultaneous raw EEG seizure activity of at least 10 seconds duration. 14 18 19 In the compressed aEEG trend, a typical neonatal single seizure looks like a “hump” that interrupts the background trace. Epileptic seizures with a duration of <30 seconds can be difficult to detect in the compressed aEEG trend. 20 Therefore, epileptic seizures need to be detected in the raw EEG.
In this study, a typical neonatal single seizure was found in Fig. 3 . The timing and duration of seizures were noted. Epileptic seizure was recorded at 3 hours and 45 minutes. The seizure activity lasted approximately 30 seconds ( Fig. 3A–C ). However, clinical symptoms were not observed. The presentation of the seizure was subclinical. Because of the paucity of clinical correlates, clinical diagnosis of neonatal seizures is difficult. Therefore, it was difficult to identify seizures without aEEG monitoring. Early recording of NKH would be helpful for the early diagnosis and treatment of seizures, and the phenobarbital sodium was initiated immediately. The early detection and intervention for seizures may improve outcomes in patients with NKH.
A typical neonatal single seizure was found in ( A ). Epileptic seizure was recorded at 3 hours and 45 minutes. The seizure activity lasted approximately 30 seconds ( A–C ).
Discussion
NKH is a rare inherited genetic metabolic disease with variable clinical manifestations, which is mainly divided into classic and non-classical types. 21 The classic type is more common (84%), with progressive encephalopathy manifestations, low response, lethargy, hypotonia, myoclonic epilepsy, and symptoms such as hiccups or apneas. The symptoms worsen in a short period of time, and most children need ventilator support. 2 5 22 23 Being a fatal disease, the majority of patients die within the first week of life, and those who survive suffer from neurologic sequelae. 24 In this study, the patient belonged to a neonatal type of NKH, which might have a severe prognosis. At last, his parents decided to abandon treatment. The patient was hospitalized for 20 days in our department and died 1 day after discharge.
Patients with NKH often exhibit complicated clinical phenotypes and a lack of specific symptoms, especially the symptoms of encephalopathy are atypical. The aEEG has been used for newborns with associated risks of neurological disorders. 25 26 It has also been used for monitoring seizures and the evaluation of antiepileptic drug treatment. 27 Transient phases of clinical stabilization and normalized plasma biochemical results may not reflect the actual encephalopathic process. Serial EEGs are helpful to assess the efficacy of treatment and to modify the therapeutic approach as early as possible. 2 In this study, the aEEG was performed as early as possible in our study. There has been no study on the efficacy of aEEG to evaluate neonates with NKH in China. Clinically, the symptoms of seizures were not observed. If aEEG was not performed as early as possible, the diagnosis and treatment may be delayed. aEEG is a tool, not a treatment, but aEEG was helpful for the early diagnosis and treatment of seizures. It can help the doctor to carry out appropriate treatment at the earliest. The early detection and intervention for seizures may improve outcomes in patients with NKH.
As shown in this study, the aEEG tracings in the NKH patient displayed a multitude of abnormalities. A rather featureless background pattern with a lack of normal sleep cycle was noted, which means the child had severe brain damage. 15 Also, the EEG typically showed a burst–suppression pattern. A longer IBI than the corresponding gestational age also suggested that the child might have brain injury. 16 In this study, the EEG findings were similar to aEEG findings. The 24-hour EEG also typically showed a burst–suppression pattern ( Fig. 4 ).
Electroencephalogram: burst–suppression.
A typical neonatal single seizure was found in Fig. 3A–C , but clinical symptoms were not observed. The presentation of the seizure was subclinical. Because of the paucity of clinical correlates, clinical diagnosis of neonatal seizures is difficult. Early recording of high-risk infants is helpful for the early diagnosis and treatment of seizures. Despite conventional EEG remaining the “gold standard” for epileptic seizures and electroencephalographic assessment of encephalopathic changes, the conventional EEG requires complex equipment and specialized staff to apply the numerous electrodes, and needs neurophysiologists in the clinical centers to interpret the report. 28 Compared with the EEG, the most important thing about aEEG is unnecessary to wait for neurophysiologists to interpret the report. That means the doctors can also detect the epileptic waves and give the appropriate treatment as soon as possible. It is good for the patient. The aEEG examination is more convenient than EEG in clinical settings. For the aEEG, recordings of longer duration can be obtained easily, and the ongoing monitoring of patients is encouraged. However, a review of the raw EEG tracing is indicated to confirm the presence of typical seizure potentials. The aEEG and EEG complement each other.
In previously reported NKH cases, genetic analysis determined that approximately 70 to 80% of the gene mutations were caused by GLDC gene mutations, and only 15 to 20% by AMT gene mutations. 1 To our knowledge, this is the second case of NKH caused by the AMT gene mutation found in Chinese people, and the mutation is homozygous, as follows: homozygous p.(Arg222Cys) mutation. Furthermore, this is the first case report describing the changes in the aEEG pattern of NKH in Chinese people so far. Therefore, it is necessary to report this case.
In conclusion, patients with NKH often exhibit complicated clinical phenotypes and lack specific symptoms, especially the symptoms of encephalopathy are atypical. This case showed that the aEEG monitoring was useful for the early diagnosis and treatment of seizures. It can help the doctor to carry out appropriate treatment as soon as possible. The application value of the aEEG in patients with NKH was significant.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Coughlin C RII Swanson M A Kronquist K The genetic basis of classic nonketotic hyperglycinemia due to mutations in GLDC and AMT Genet Med 2017190110411127362913 10.1038/gim.2016.74 · doi ↗ · pubmed ↗
- 2Poothrikovil R P Al Thihli K Al Futaisi A Al Murshidi F Nonketotic hyperglycinemia: Two case reports and review Neurodiagn J 2019590314215131433733 10.1080/21646821.2019.1645549 · doi ↗ · pubmed ↗
- 3Swanson M A Coughlin C R Jr Scharer G H Biochemical and molecular predictors for prognosis in nonketotic hyperglycinemia Ann Neurol 2015780460661826179960 10.1002/ana.24485 PMC 4767401 · doi ↗ · pubmed ↗
- 4Gao Z J Jiang Q Chen Q Xu K M Clinical and molecular genetic study of nonketotic hyperglycinemia in a Chinese family [in Chinese]Zhongguo Dang Dai Er Ke Za Zhi 2017190326827128302194 10.7499/j.issn.1008-8830.2017.03.003PMC 7390153 · doi ↗ · pubmed ↗
- 5Lin Y Zheng Z Sun W Fu QA novel compound heterozygous variant identified in GLDC gene in a Chinese family with non-ketotic hyperglycinemia BMC Med Genet 20181901529304759 10.1186/s 12881-017-0517-1PMC 5755286 · doi ↗ · pubmed ↗
- 6Li H F Clinical and molecular genetic characteristics of nonketotic hyperglycinemia [in Chinese]Zhongguo Dang Dai Er Ke Za Zhi 2017190327227428302195 10.7499/j.issn.1008-8830.2017.03.004PMC 7390138 · doi ↗ · pubmed ↗
- 7Jiang T J Jiang J J Xu J L Zhen J Jiang P F Gao F Clinical and genetic analyses of a family with atypical nonketotic hyperglycinemia caused by compound heterozygous mutations in the GLDC gene [in Chinese]Zhongguo Dang Dai Er Ke Za Zhi 201719101087109129046206 10.7499/j.issn.1008-8830.2017.10.011PMC 7389275 · doi ↗ · pubmed ↗
- 8Karimzadeh P Taghdiri M M Abasi E Metabolic screening in children with neurodevelopmental delay, seizure and/or regression Iran J Child Neurol 20171103424728883876 PMC 5582359 · pubmed ↗