Bile Leakage after Liver Transplantation Owing to Stricture of Afferent Jejunal Loop Caused by an Intussusception Valve after Biliary Atresia Surgery: A Case Report
Hironobu Ito, Ryusuke Saito, Masaki Sato, Kyohei Kasuda, Naruhito Takido, Hiroyuki Ogasawara, Yoshihiro Shono, Muneyuki Matsumura, Ryuji Okubo, Kengo Sasaki, Atsushi Fujio, Hironori Kudo, Kazuaki Tokodai, Motoshi Wada, Michiaki Unno, Takashi Kamei

TL;DR
A long-term complication from a surgical valve used in biliary atresia led to bile leakage after liver transplantation in a patient.
Contribution
Highlights a rare but important late-onset complication of intussusception anti-reflux valves in liver transplant patients with biliary atresia.
Findings
Afferent jejunal stricture caused by an intussusception valve was identified as the cause of bile leakage after liver transplantation.
Long-term fibrotic changes from the valve likely contributed to the stricture 34 years after initial surgery.
Preoperative assessment and jejunal limb resection during transplantation helped prevent further complications.
Abstract
Biliary atresia (BA) is a progressive cholangiopathy in neonates that results in biliary cirrhosis and liver failure without early intervention. Hepatic portoenterostomy (Kasai operation) remains the standard treatment, significantly improving survival rates. However, postoperative cholangitis is a major determinant of prognosis. To prevent cholangitis, various surgical modifications, including anti-reflux procedures such as intussusception anti-reflux valves (IAV), have been introduced. Although IAV has been widely adopted, some reports suggest that long-term survivors may develop afferent jejunal limb stenosis, leading to complications such as cholangitis and intestinal obstruction. Herein, we report a case of afferent jejunal loop stricture caused by IAV, which became symptomatic after liver transplantation (LT). A 34-year-old man with a history of BA underwent Kasai operation with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
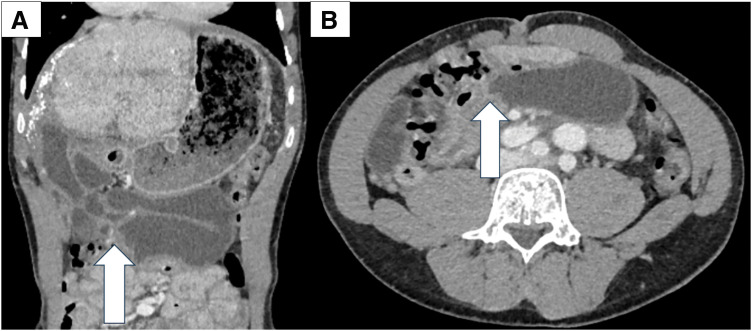 Fig. 1
Fig. 1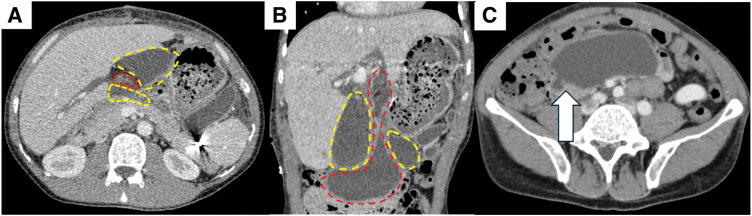 Fig. 2
Fig. 2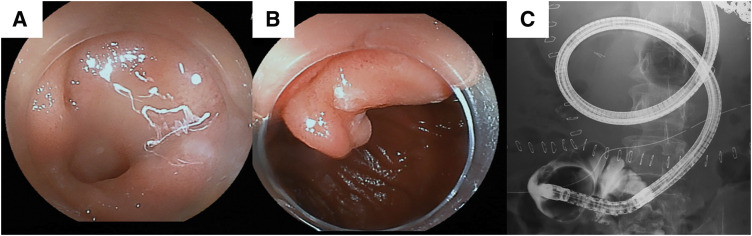 Fig. 3
Fig. 3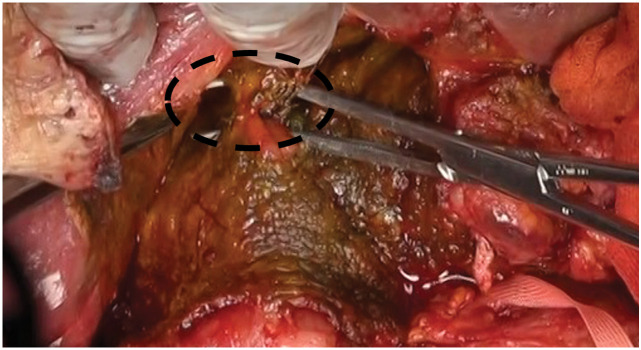 Fig. 4
Fig. 4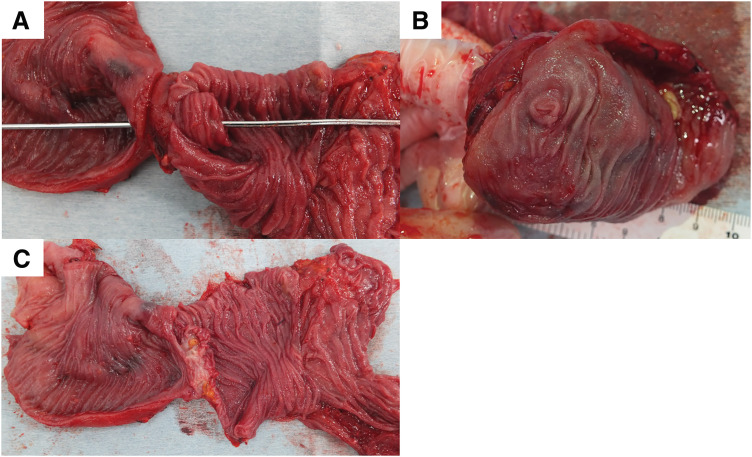 Fig. 5
Fig. 5| Case (Ref.) | Age | Sex | Valve type | Period after Kasai | Complication |
|---|---|---|---|---|---|
| 1 (11) | 24 | F | IAV | 24 years | Torsion of afferent limb (strangulated ileus) |
| 2 (12) | 15 | F | IAV | 15 years | Cholangitis from cholestasis |
| 3 (12) | 26 | M | IAV | 26 years | Cholangitis from cholestasis |
| 4 (17) | 2 months | M | IAV | 5 days | Jejunal perforation |
| 5 (22) | 20 | F | IAV | 20 years | Intestinal obstruction caused by gallstone |
| Our case | 34 | M | IAV and Spur valve | 34 years | Disruption of hepatojejunal anastomosis |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPediatric Hepatobiliary Diseases and Treatments · Congenital Anomalies and Fetal Surgery · Gallbladder and Bile Duct Disorders
Abbreviations
BA biliary atresia CT computed tomography IAV intussusception anti-reflux valves LT liver transplantation POD postoperative day
INTRODUCTION
BA is an idiopathic cholangiopathy that arises in newborns and leads to progressive inflammatory obstruction of the extrahepatic bile ducts. Without treatment, BA inevitably results in biliary cirrhosis and liver failure within the first or second year of life.^1)^ Hepatic portoenterostomy, commonly referred to as Kasai operation, is the essential surgical treatment that has significantly improved patient prognosis.^2,3)^ However, postoperative cholangitis significantly impacts the prognosis of patients with BA. Therefore, to prevent postoperative cholangitis, various surgical techniques have been implemented,^4)^ including external drainage procedures such as the Suruga II method.^5)^ Additionally, anti-reflux procedures, such as the double Roux-en-Y method and Roux-en-Y reconstruction with an anti-reflux intestinal valve, have been performed.^6–8)^ In the 1980s, hepatojejunostomy with an IAV was introduced to prevent cholangitis and was widely accepted.^9,10)^ On the other hand, there are some reports that IAV may cause stenosis of the afferent limb in the long-term survivors resulting in various complications such as strangulated intestinal obstruction or cholangitis due to cholestasis.^11,12)^ Herein, we report a case of afferent jejunal loop stricture caused by IAV after BA surgery, which became apparent post-LT.
CASE PRESENTATION
The patient was a 34-year-old man who underwent Kasai operation with IAV and spur valve for BA 77 days after birth. There was no major complication in the postoperative course in his childhood and he had experienced only 3 episodes of cholangitis. As the liver function got worse, some complications due to liver cirrhosis happened including intestinal bleeding in his thirties. He was diagnosed with porto-pulmonary hypertension 10 years ago, and prescribed 10 mg of Tadarafil and 25 mg of Eplerenone per day. As the diagnosis was liver cirrhosis after BA with porto-pulmonary hypertension, deceased donor LT was performed when he was 34-year-old (Model for end-stage liver disease score: 12). Preoperative enhanced CT showed an atrophic liver and obstruction of the portal vein with dilated collateral circulation. During the operation, there were strong adhesions especially around the liver hilum. We could observe the dilatation of the afferent limb in the operation. Due to adhesion, we cut 30 cm of afferent jejunum, including hepaticojejunostomy. The superior mesenteric vein of the recipient was anastomosed with the portal vein of the donor using jump graft (iliac vein). Choledocho-jejunostomy with drainage tube was also performed. Although the initial postoperative course was stable, on POD 6, the patient developed a fever exceeding 38°C, accompanied by an elevation of the inflammatory markers and hepatobiliary enzymes. Given the suspicion of cholangitis, empirical antibiotic therapy was initiated. Despite the continued antibiotic treatment, cholangitis symptoms fluctuated and persisted for over a week. Retrospectively, the dilated bowel loop in the upper abdomen was considered to be the afferent limb with a beak sign (Fig. 1). CT image on POD 16 identified an intra-abdominal abscess surrounding the hepatojejunal anastomosis (Fig. 2). Consequently, percutaneous abscess drainage was performed, yielding a bile-like fluid, suggesting an anastomotic disruption secondary to jejunal limb stricture. To address this complication, double-balloon endoscopic retrograde cholangiography was performed to assess and attempt dilation of the afferent limb. However, complete luminal obstruction was observed (Fig. 3). The obstruction was attributed to an anti-reflux valve constructed during the previous Kasai operation, necessitating surgical reconstruction of the biliary drainage route on POD 25. The previous anastomosis of biliary tract was almost dehisced, with approximately half of the circumference disrupted (Fig. 4). The obstructed Roux-en-Y limb was resected, and a new limb was created, followed by reconstruction of the hepatojejunal anastomosis with the biliary drainage tube placement. On examination of the resected intestine, its lumen was nearly occluded by thickened fibrous tissue, with a pinhole (Fig. 5). Postoperatively, the patient exhibited rapid resolution of cholangitis, with no evidence of biliary leakage. He was discharged on POD 45 with stable laboratory findings.
Preoperative CT image. (A) Dilatation of the afferent limb with beak sign was observed in coronal view. (B) Axial view. White arrow: Beak sign.
CT image on POD 16. (A) Abscess area surrounding the cholangiojejunostomy was observed by axial view. (B) Coronal view of the image. (C) Beak sign and dilatation of the proximal bowel by axial view. Red dot area: Dilated afferent jejunal loop, Yellow dot area: Abscess, White arrow: Beak sign.
Double balloon endoscopy and retrograde cholangiography. (A), (B) Endoscopic examination revealed a valve-like structure, however, the lumen could not be observed. (C) Even with the use of a contrast agent, the jejunum loop was not visualized.
Picture of the second operation. The cholangiojejunal anastomosis was almost dehisced, with approximately half of the circumference disrupted. Black dot area: Cholangiojejunal anastomosis site.
Resected afferent jejunal limb. (A)–(C) The lumen was almost occluded by the fibrous tissue, with a pinhole.
DISCUSSION
Postoperative cholangitis has been reported to occur in approximately 40%–80% of patients with BA following Kasai operation, significantly contributing to poor prognosis.^13–15)^ Therefore, various anti-reflux procedures including intestinal anti-reflux valve have been reported.^4,9,11)^ There are 2 main types of anti-reflux valves: IAV and spur valve. The most significant difference between the spur valve and the IAV is that the spur valve is approximately semi-circumferential, whereas IAV is fully circumferential and is more likely to cause stenosis of the afferent limb. This is the first report that the afferent jejunal loop stricture caused by IAV became apparent due to bile leakage just after LT.
Since 1980, when Tanaka et al. first reported the addition of an anti-reflux valve,^9)^ several retrospective studies have suggested that anti-reflux valves reduce the incidence of postoperative cholangitis compared with the standard Kasai operation.^8,10,16–18)^ However, Ogasawara et al. conducted the first prospective study in 2003,^19)^ comparing 10 patients with IAV to 11 patients without it to evaluate its efficacy in preventing cholangitis. The study found no significant difference in the occurrence rate of cholangitis between the two groups. However, due to the small sample size, the possibility remains that the study lacked sufficient power to detect a true difference. Through those decades of discussions, the effectiveness of anti-reflux valves remains a subject of debate.
According to the National Registry of BA in 2022 in our country, the most common procedure is the simple long Roux-en-Y (71.0%), followed by Roux-en-Y with anti-reflux valve (14.5%).^20)^ There is a report from China that the spur valve construction was performed in more than half of the centers (51%).^21)^ In our department, Roux-en-Y anastomosis with double valve (IAV and spur valve) was the standard procedure in 1992–2000. However, Roux-en-Y anastomosis with spur valve is the standard procedure from 2000 to date. One of the reasons for the change in procedure during this period was the suboptimal rate of bilirubin reduction, possibly due to impaired intestinal motility caused by the double valve. There are no studies comparing the efficacy of spur valves and IAV by valve types; however, the spur valve is currently considered as the mainstream option.
There are some reports that state IAV caused some postoperative complications such as repeated cholangitis or strangulated intestinal obstruction, as summarized in Table 1.^11,12,17,22)^ According to these reports, these complications occurred in the long-term survivor with IAV, except for case 4. These complications are likely to result from stenosis that develops over a long-term course, occurring at least 15 years after the first operation, and subsequently leading to various clinical manifestations. We could not find a report that spur valve caused the stenosis of afferent limb or ascending cholangitis. In practice, it is extremely difficult to distinguish whether cholangitis and liver failure are caused by the valve, the progression of the underlying disease, or a combination of both. Even in LT cases after Kasai operation, cases where the valve played a harmful role are likely overlooked. In our case, he was diagnosed with porto-pulmonary hypertension 10 years before and the dilatation of the afferent limb was first observed by CT 1 year before LT. Therefore, it remains unclear to what extent IAV was involved in the development of liver cirrhosis or porto-pulmonary hypertension.
We could observe the dilatation of the afferent limb by CT before operation (Fig. 1). There are 3 possible hypotheses as to why narrowing of the afferent limb became apparent after LT. First, a large amount of bile was produced by the healthy liver after transplantation. Second, the intraoperative resection of 30 cm of jejunum reduced the reservoir capacity. Third, postoperative edema markedly exacerbated the existing stenotic region. It has been reported that the number of patients who survive with their native liver after Kasai operation is 44.5% at 20 years and 40.8% at 30 years.^20)^ Patients with IAV treated in 1980–2000 may require LT due to liver failure. Therefore, a similar case we reported this time could occur. To prevent postoperative complication after LT caused by the anti-reflux valve, we should check the operative procedure for BA for whether the anti-reflux valve was constructed or not, and additionally, the need to identify the type of valve. Hepatobiliary scintigraphy could have been one of the options for detecting stasis in the afferent limb.^23)^ In addition, resection of dilated afferent jejunum and reconstruction of Roux-en-Y anastomosis should be considered for cases with the dilatation of the afferent limb preoperatively.
CONCLUSIONS
We report a case of afferent jejunal loop stricture caused by IAV after BA surgery, which became apparent after LT. Stricture due to IAV can occur over a long-term course. In cases with intussusception valves or suspected stenosis of the afferent jejunum, reconstruction of Roux-en-Y anastomosis should be considered during LT.
DECLARATIONS
Funding
No funding was received for this report.
Authors’ contributions
H. Ito and R.S. participated in all aspects of this study, including patient management, report conceptualization, and draft writing.
M.S., K.K., N.T., H.O., Y.S., M.M., K.S., and A.F.; managed the patients.
R.O., H.K., K.T., M.W., M.U., and T.K.; supervised the article.
All authors have read and approved the manuscript and agree to be held accountable for all aspects of this report.
Availability of data and materials
The datasets supporting the conclusions of this study are included in this article.
Ethics approval and consent to participate
This work does not require ethical considerations or approval. Informed consent to participate in this study was obtained from the patient.
Consent for publication
Consent was obtained from the patient for the publication of this case report.
Competing interests
All authors declare no competing interests for this article.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hartley JL Davenport M Kelly DA. Biliary atresia. Lancet 2009; 374: 1704–13.19914515 10.1016/S 0140-6736(09)60946-6 · doi ↗ · pubmed ↗
- 2Kasai M Suzuki S. A new operation for “non-correctable” biliary atresia: hepatic portoenterostomy (in Japanese). Shujutsu (Operation)1959; 13: 733–9.
- 3Ohi R. A history of the Kasai operation: hepatic portoenterostomy for biliary atresia. World J Surg 1988; 12: 871–4.3074594 10.1007/BF 01655504 · doi ↗ · pubmed ↗
- 4Sharma S Gupta DK. Surgical modifications, additions, and alternatives to Kasai hepato-portoenterostomy to improve the outcome in biliary atresia. Pediatr Surg Int 2017; 33: 1275–82.28980051 10.1007/s 00383-017-4162-8 · doi ↗ · pubmed ↗
- 5Suruga K Miyano T Kitahara Y Treatment of biliary atresia: a study of our operative results. J Pediatr Surg 1981; 16(Suppl 1): 621–6.7277165 10.1016/0022-3468(81)90016-6 · doi ↗ · pubmed ↗
- 6Kasai M. Treatment of biliary atresia with special reference to hepatic portoenterostomy and its modifications. Prog Pediatr Surg 1974; 6: 5–52.4596366 · pubmed ↗
- 7Zhang JZ Wang YX Chen JJ. Antireflux spur valve in Roux-Y anastomosis. Chin Med J (Engl) 1982; 95: 921–4.6819936 · pubmed ↗
- 8Nakajo T Hashizume K Saeki M Intussusception-type antireflux valve in the Roux-en-Y loop to prevent ascending cholangitis after hepatic portojejunostomy. J Pediatr Surg 1990; 25: 311–4.2313499 10.1016/0022-3468(90)90074-j · doi ↗ · pubmed ↗