Incarceration of the Afferent Loop into the Sutured Closed Mesenteric Defect after Gastrectomy Followed by Billroth-II Reconstruction for Gastric Cancer: Two Case Reports
Kiyotomi Maruyama, Tadaaki Shimizu, Kou Shimada, Arano Makino, Natsuhiro Morita, Tasuku Kawaguchi, Takahiro Amano, Tomoki Shirota, Kuniyuki Gomi, Motohiro Mihara

TL;DR
Two patients developed internal hernias after gastrectomy with Billroth-II reconstruction, where the afferent loop became trapped in a closed mesenteric defect, highlighting the need for careful surgical closure to prevent such complications.
Contribution
The paper highlights a rare but critical complication of Billroth-II reconstruction and suggests optimal mesenteric defect closure techniques to prevent internal hernias.
Findings
In both cases, the afferent loop became incarcerated in a closed mesenteric defect after Billroth-II reconstruction.
Emergency surgery was required to relieve the intestinal incarceration, with one patient experiencing postoperative complications.
The hernia orifice was located near the Treiz ligament, suggesting the need for careful closure away from this area.
Abstract
Internal hernia is a critical complication after laparoscopic gastrectomy with Roux-en-Y, Billroth-II or double tract reconstruction. It is recommended that mesenteric defects should be closed to prevent internal hernias. We reported two patients who developed internal hernias, in which the afferent loop of Billroth-II reconstruction became incarcerated into the closed mesenteric defects. A man in his late 40s had undergone laparoscopic distal gastrectomy 3 months prior for gastric cancer followed by Billroth-II reconstruction, in which mesenteric defect was sutured closed. The patient visited our hospital complaining of sudden severe upper abdominal pain and was diagnosed with afferent loop obstruction due to an incarcerated internal hernia complicated by acute pancreatitis. Emergency surgery, in which intestinal incarceration was relieved and intestinal ischemia was not found, was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
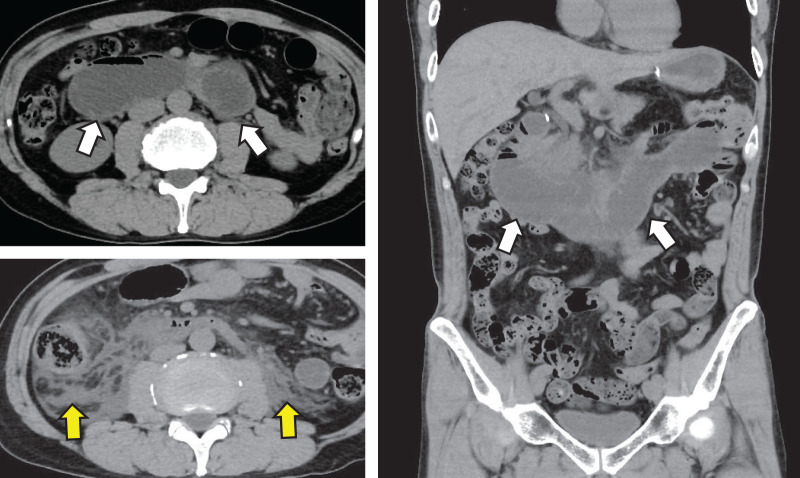 Fig. 1
Fig. 1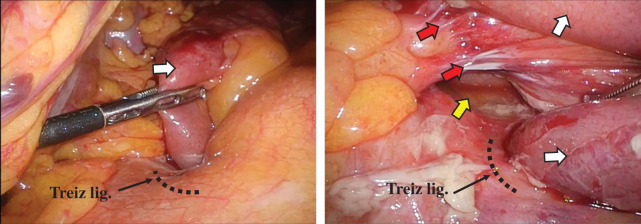 Fig. 2
Fig. 2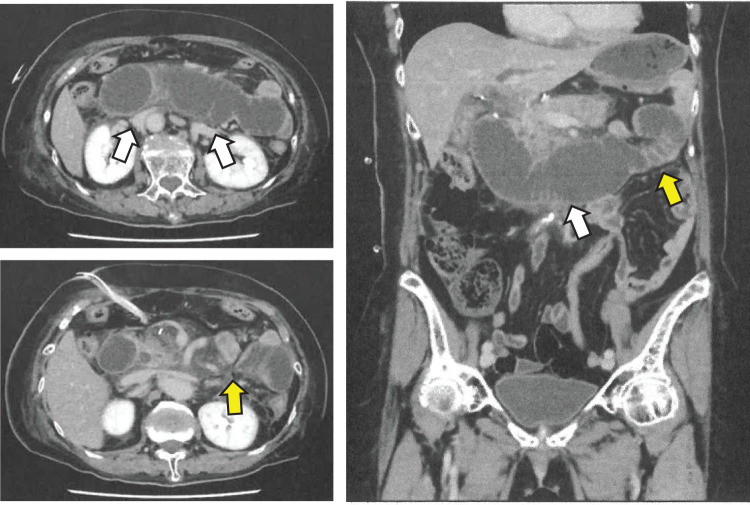 Fig. 3
Fig. 3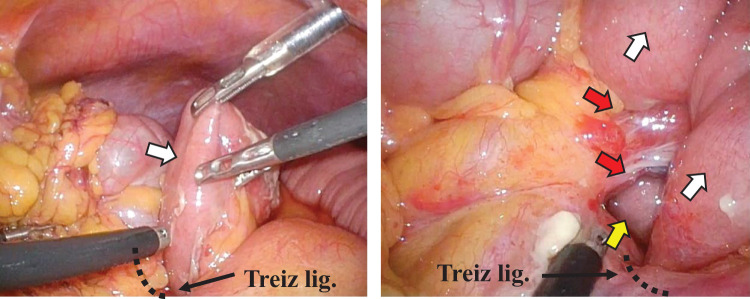 Fig. 4
Fig. 4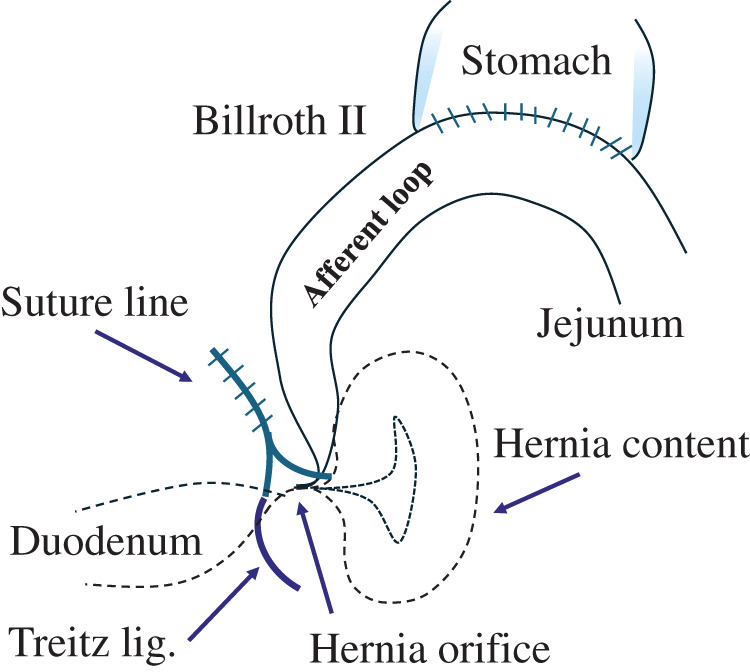 Fig. 5
Fig. 5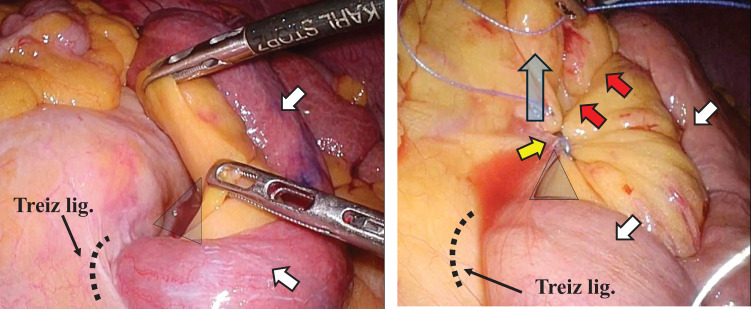 Fig. 6
Fig. 6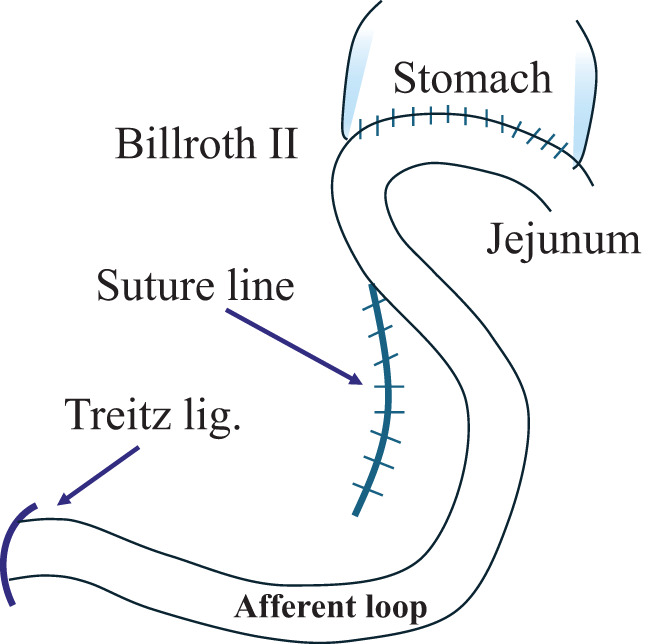 Fig. 7
Fig. 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Gastrointestinal disorders and treatments · Intestinal and Peritoneal Adhesions
Abbreviations
B-II Billroth-II reconstruction GC gastric cancer HP Helicobacter pylori IH internal hernia MD mesenteric defect R-Y Roux-Y
INTRODUCTION
Despite substantial declines in noncardia GC incidence due mainly to the global trend in decreasing HP infection rates, the incidence of proximal gastric cancer, that is, adenocarcinoma of the esophagogastric junction or upper portion of the stomach, has been rising markedly worldwide,^1–4)^ including in Japan.^5)^ For upper gastric cancer, total gastrectomy, proximal gastrectomy, or distal gastrectomy is selected depending on the location and progression of the cancer. As the number of upper gastric cancers is increasing, B-II and R-Y reconstruction may become more common for distal gastrectomy than Billroth-I reconstruction. In reconstructions such as B-II and R-Y, which leave an MD, postoperative IH can be a problem. Nonclosure of MDs, the laparoscopic approach, and the totally laparoscopic approach were found to be independent risk factors for IH.^6)^ MD should be closed to prevent IH after gastrectomy.^6,7)^
IHs associated with the reconstructed intestine after laparoscopic gastrectomy was observed in 2.0% of cases (R-Y: one case; double tract: one case; B-II: four cases; including cases in which the MDs were not closed). Initially, we were not closing the MDs after B-II, when we were performing open gastrectomy. We started closing MDs after our first experience with an IH after gastrectomy followed by B-II, in which the MD was not closed. However, we experienced two cases of IH in which the afferent loop of B-II became incarcerated into the closed MD despite the suture closure. The mechanisms are reported in a literature review. There have been no reports of the intestine being incarcerated into the site of MD suture closure.
CASE PRESENTATION
Case 1
A man in his late 40s visited our emergency room late at night, complaining of sudden severe epigastric pain, and was admitted. The patient had undergone laparoscopic distal gastrectomy followed by B-II with antiperistalsis anastomosis through the antecolic route, in which the MD was sutured closed with continuous suturing with a 3-0 nonabsorbable barbed suture, for pStage I GC 3 month prior. The patient had no other medical history. The patient’s height was 177.7 cm, his weight was 70.0 kg, his body temperature was 36.2°C, his blood pressure was 139/103 mmHg, his pulse rate was 55 beats/min, and his respiratory rate was 18 breaths/min. Physical examination revealed that the abdomen was flat and soft, but there was tenderness in the epigastrium and no rebound tenderness or muscular guarding. Laboratory examination revealed no abnormalities except for a high serum amylase value of 991 U/L. A CT scan revealed abnormal dilation of the intestine from the duodenum to the afferent loop, and widespread edema around the pancreas head and in the right retroperitoneum posterior to the duodenum (Fig. 1). The patient was diagnosed with afferent loop obstruction due to an incarcerated IH complicated by acute pancreatitis.
CT scan revealed abnormal dilation of the intestine from the duodenum to the afferent loop (white arrow) and widespread edema in the right retroperitoneum posterior to the duodenum (yellow arrow).
We performed emergency surgery 10 hours after his visit. The surgery was performed laparoscopically. Surgical findings revealed that the afferent loop was incarcerated at the lowest end of the suture line in the MD that had been closed during the initial operation and that the duodenum and the incarcerated afferent loop were significantly dilated. The intestine was carefully and gently returned to its original position (Fig. 2). We decided not to close the hernia orifice because it was close to the duodenum at the Treiz ligament. The operation lasted for 85 minutes, and the blood loss volume was 5 g. In the postoperative course, on the 8th postoperative day, a duodenal microperforation occurred, and emergency surgery, involving peritoneal lavage, abdominal drainage, retrograde duodenal tube drainage, and biliary drainage, was performed. The patient had difficulty with treatment and was discharged on the 59th postoperative day.
The incarcerated afferent loop (white allow) was carefully and gently returned to its original position. It was found after hernia reduction that a hernia orifice (yellow arrow) formed between the lower end of the suture line (red arrow) in the initial operation and the Treiz ligament.
Case 2
A woman in her late 70s experienced nausea without abdominal pain on the 7th postoperative day. The patient had undergone laparoscopic distal gastrectomy followed by B-II with antiperistalsis anastomosis through the antecolic route, in which the MD was sutured closed with continuous suturing with a 3-0 nonabsorbable barbed suture, for pStage IIA GC 7 days prior. The patient’s medical history included hypertension. The patient’s height was 150.3 cm, her weight was 58.0 kg, her body temperature was 37.2°C, her blood pressure was 147/74 mmHg, her pulse rate was 93 beats/min, and her respiratory rate was 168 breaths/min. Physical examination revealed that the abdomen was flat and soft without tenderness. Laboratory examination revealed a high level of inflammatory response, with a WBC count of 135.9 × 10^2^/μL and a CRP value of 19.2 mg/dL, hypoproteinemia with an Alb value of 2.7 mg/dL; and an increase in hepatobiliary data, with an AST value of 310 IU/L, an ALT value of 433 IU/L, a total bilirubin value of 10.57 mg/dL, an LDH value of 357 IU/L, an ALP of 318 IU/L, and a γGTP value of 436 U/L, but no other abnormalities were found. A CT scan revealed abnormal dilation of the intestine from the duodenum to the afferent loop and stricture after the dilatation (Fig. 3). The patient was diagnosed with afferent loop obstruction due to an incarcerated IH.
CT scan revealed abnormal dilation of the intestine from the duodenum to the afferent loop (white arrow) and stricture after the dilatation (yellow arrow).
We performed emergency surgery that same day. The surgery was performed laparoscopically. Surgical findings revealed that the afferent loop was incarcerated at the lowest end of the suture line in the MD that had been closed during the initial operation and that the duodenum and the incarcerated intestine were significantly dilated. The intestine was carefully and gently returned to its original position (Fig. 4). We decided not to close the hernia orifice because it was close to the duodenum at the Treiz ligament. The operation lasted for 56 minutes, and the blood loss volume was 3 g. The patient’s postoperative course was uneventful, and the patient was discharged on the 20th postoperative day.
The incarcerated afferent loop (white allow) was carefully and gently returned to its original position. It was revealed after hernia reduction that a hernia orifice (yellow arrow) formed between the lower end of the suture line (red arrow) in the initial operation and the Treiz ligament.
DISCUSSION
In Japan, the prevalence of HP infection has decreased^8)^; consequently, the incidence of HP-related GC has decreased. However, the incidence of HP infection-negative GC is expected to increase. Imamura et al.^9)^ reported that HP infection-negative GC lesions were predominantly observed in the fundic gland (72.2%). For these reasons, an increase in GC in the upper part of the stomach is predicted in the near future, which may result in an increase in total gastrectomy, proximal gastrectomy, and distal gastrectomy with a small stomach remnant, leading to an increase in R-Y, double tract reconstruction, and B-II.
IH is a well-known complication following laparoscopic and open gastrointestinal surgery and is a critical problem because it can cause life-threatening conditions, such as bowel strangulation or perforation.^10,11)^ IH is particularly likely to occur after surgery in which MDs are formed, such as those followed by R-Y and B-II, or after surgery in which the intestine is fixed to the abdominal wall, such as jejunostomy or colostomy. Low level of postoperative intestinal adhesion is a risk factor for the development of IH. Free intestines can become incarcerated in the MD or become entangled with the fixed intestine. IH, which obstructs the duodenum in the reconstructed intestine, is often complicated by acute pancreatitis, especially when the duodenum is blind-ended, and requires immediate treatment. Laparoscopic surgeries have long been the standard treatment for gastrointestinal cancer surgery, and the use of adhesion prevention agents has also become widespread.^12)^ These procedures and agents are less invasive and reduce the risk of postoperative adhesions. In subsequent operations following laparoscopic surgery, surgeons notice less adhesion than they do after conventional open surgery. Laparoscopic surgery offers various benefits to patients, but the low incidence of postoperative intestinal adhesions appears to increase the risk of IH.
Kang et al.^6)^ analyzed 111 (1.7%) patients with IHs identified via CT or surgical exploration and reported that among the 6474 patients who underwent gastrectomy for GC, 2.0% developed IHs after laparoscopic surgery, 0.9% developed IHs after open surgery, and 0%, 1.1%, 3.1%, and 2.3% developed IHs after undergoing Billroth-I reconstruction, B-II, R-Y, or double tract, reconstruction, respectively. IH occurs most often after R-Y, the so-called Petersen’s hernia. According to the multivariate analysis, nonclosure of MDs (P < 0.01), laparoscopic approach (P < 0.01), and totally laparoscopic approach (P = 0.03) were independent risk factors for IH. The importance of closing MDs was emphasized to prevent IH after gastrectomy. We have been closing the MDs with sutures since our first experience with IH after B-II.
The median interval time to the development of IH was reported to be 450 days after gastrectomy.^6)^ It is presumed that stitches closing the MDs may loosen or that gaps between sutures may become larger, as the amount of mesenteric fat tissue decreases due to excess body weight loss after gastrectomy. This may contribute to the development of IHs even after closure of the defects.^13–15)^ There is a high possibility of dehiscence, especially if the suture is absorbable. However, in our cases, MDs were sutured with non-absorbable sutures and IHs developed at 7 days and 3 months immediately after gastrectomy, so this is not the only cause of incarceration of the afferent loop.
Left paraduodenal hernia, a rare condition, has been reported.^16–18)^ Left paraduodenal hernias occur when the intestinal tract prolapses to the dorsal side of the descending mesocolon via the dorsal side of the inferior mesenteric vein (Landzert’s fossa). This fossa is formed congenitally, and although the anatomical structure that forms the hernia orifice is completely different, we believe that a similar phenomenon occurred in our patients. In other words, the terminal part of the duodenum at the Treiz ligament, which was fixed to the retroperitoneum, became the leading part, passed through a hernia orifice formed at the Treiz ligament, protruded into the dorsal side of the mesenterium, and the following afferent loop was pulled in and became incarcerated (Fig. 5). Furthermore, in our patients, the MDs were continuously closed using a barbed suture, with the starting point close to the Treiz ligament and the proceeding suture toward the gastric remnant. This method involved shortening the suture line and lifting upward the sutured mesenterium, resulting in the formation of a hernia orifice close to the Treiz ligament, which was fixed to the retroperitoneum (Fig. 6). Therefore, the MD should be closed with the starting point of the suture and the suture line being at the left side as far from the Treiz ligament as possible (Fig. 7). In this regard, performing MD suturing following B-II with isoperistalsis may be effective since suturing can be easily performed without involving the Treiz ligaments. It is thought that continuous suturing will not be an issue if the suture line is placed away from the Treiz ligament. The precautions regarding the position of the suture line also apply to R-Y reconstruction.
This schema shows the mechanism of IH after Billroth II. As a result of closure of the MD adjacent to the Treiz ligament, a hernia orifice was formed at the site. The duodenum at the Treiz ligament was pulled dorsally and the afferent loop was retracted into the hernia orifice.
Surgical findings in the initial operation in case 1. Afferent loop (white arrow). The mesenteric defect was continuously closed using a nonabsorbable barbed suture, with the starting point (yellow arrow) close to the Treiz ligament and the proceeding suture toward the gastric remnant (red arrow). This method involved shortening the suture line (red arrow) and lifting upward the sutured mesenterium (blue arrow), resulting in the formation of a hernia orifice (triangle) close to the Treiz ligament.
To prevent the development of the IH, the MD should be closed with the starting point of the suture and the suture line being at the left side as far as possible from the Treiz ligament.
One point to consider is whether the hernia orifice should be sutured closed. We did not dare close the hernia orifice in our patients. In fact, since we had no experience with this type of IH, we were unable to elucidate its mechanism during the operation. We were aware that the duodenum at the Treiz ligament was pulled dorsally and that this intestine was the leading part, so we were worried that closing the hernia orifice would cause further stenosis and result in the duodenum becoming incarcerated at that site again. The cause of the IH in these cases was that the closure of the MD was performed close to the Treiz ligament. Therefore, in order to prevent the future recurrence of IH, we retrospectively concluded that it was necessary to release the MD that was sutured closed in the initial surgery and suture the MD again at a part farther to the left side from the Treiz ligament. In our patients, the tissues around the hernia became hardened due to the postoperative changes, releasing the MD, which was sutured with barbed sutures, and was avoided as it would have risked damaging the blood vessels of the reconstructed intestine. However, we would like to emphasize again that to prevent hernia recurrence, it is better to re-close the MD.
The hernia orifice formed after suturing the MD is very narrow, so once the intestine protrudes into the orifice, it is prone to becoming incarcerated. This IH is more likely to develop into a serious condition than an IH without closing the MD; therefore, greater caution and immediate treatment are needed.
CONCLUSIONS
IHs after MD closure are prone to incarceration and can easily become serious, so immediate treatment is needed. Although closure of the MD after B-II is necessary to prevent IH, it is recommended that the MD should be closed on the left side as far as possible from the duodenum situated at the Treiz ligament.
ACKNOWLEDGMENTS
We would like to thank AJE (https://www.aje.com) for English language editing.
DECLARATIONS
Funding
No external support was obtained for this manuscript, including funding for equipment and drugs.
Authors’ contributions
KM and TShim contributed to the acquisition of the clinical data and prepared the manuscript for this case report.
KM, KS, AM, TShim, NM, and TK performed the operations and perioperative management.
KM and TShim contributed to the drafting and revision of the manuscript.
TA, TShir, KG, and MM supervised decision-making, implemented the treatment plan for the patient, and prepared the manuscript.
All authors have read and approved the final version of the manuscript.
Availability of data and materials
The data are not available for public access because of patient privacy concerns, but are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
The present study was conducted in accordance with the ethical standards of our institution. This work does not require ethical considerations or approval. Informed consent to participate in this study was obtained from the patients.
Consent for publication
Informed consent was obtained from the patients for the publication of this case report and any accompanying images.
Competing interests
The authors declare that they have no competing interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brown LM Devesa SS Chow WH. Incidence of adenocarcinoma of the esophagus among white Americans by sex, stage, and age. J Natl Cancer Inst 2008; 100: 1184–7.18695138 10.1093/jnci/djn 211PMC 2518165 · doi ↗ · pubmed ↗
- 2Dikken JL Lemmens VE Wouters MW Increased incidence and survival for oesophageal cancer but not for gastric cardia cancer in the Netherlands. Eur J Cancer 2012; 48: 1624–32.22317953 10.1016/j.ejca.2012.01.009 · doi ↗ · pubmed ↗
- 3Xie SH Lagergren J. Time trends in the incidence of oesophageal cancer in Asia: variations across populations and histological types. Cancer Epidemiol 2016; 44: 71–6.27504606 10.1016/j.canep.2016.08.002 · doi ↗ · pubmed ↗
- 4Deans C Yeo MS Soe MY Cancer of the gastric cardia is rising in incidence in an Asian population and is associated with adverse outcome. World J Surg 2011; 35: 617–24.21203759 10.1007/s 00268-010-0935-0 · doi ↗ · pubmed ↗
- 5Matsuno K Ishihara R Ohmori M Time trends in the incidence of esophageal adenocarcinoma, gastric adenocarcinoma, and superficial esophagogastric junction adenocarcinoma. J Gastroenterol 2019; 54: 784–91.30927083 10.1007/s 00535-019-01577-7 · doi ↗ · pubmed ↗
- 6Kang KM Cho YS Min SH Internal hernia after gastrectomy for gastric cancer in minimally invasive surgery era. Gastric Cancer 2019; 22: 1009–15.30758761 10.1007/s 10120-019-00931-1PMC 6694080 · doi ↗ · pubmed ↗
- 7Murakami K Obama K Kanaya S Mesenteric closure after laparoscopic total gastrectomy with Roux-en-Y reconstruction is effective for prevention of internal hernia: a multicenter retrospective study. Surg Endosc 2022; 36: 4181–8.34580775 10.1007/s 00464-021-08744-z · doi ↗ · pubmed ↗
- 8Kamada T Haruma K Ito M Time trends in Helicobacter pylori infection and atrophic gastritis over 40 years in Japan. Helicobacter 2015; 20: 192–8.25581708 10.1111/hel.12193 PMC 6905084 · doi ↗ · pubmed ↗