Intracranial Tuberculomas Associated with Tuberculous Meningitis
Nurten Nur Aydın, Murat Aydın, Deniz Öztürk Koçakgöl, Ömer Karaşahin

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
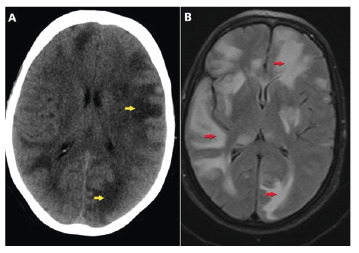 Figure 1
Figure 1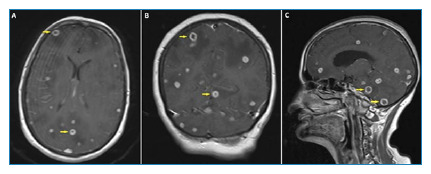 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Diseases and Tuberculosis · Tuberculosis Research and Epidemiology · Diagnosis and treatment of tuberculosis
A 58-year-old woman presented to the emergency department with fever, impaired consciousness, and seizures. Quadruple antituberculosis therapy for pulmonary tuberculosis was commenced and continued for one month. Physical examination revealed a fever of 37.7°C and stiffness of the neck. The C-reactive protein (CRP) levels (17.5 mg/L) and erythrocyte sedimentation rate (48 mm/h) were elevated; however, the remaining parameters were within normal limits. Previous sputum cultures confirmed the presence of Mycobacterium tuberculosis. Noncontrast computed tomography (CT) of the brain and magnetic resonance imaging (MRI) revealed white matter edema (Figure 1). Contrast-enhanced MRI revealed peripheral enhancement of the abscess foci (tuberculomas) (Figure 2).
FIGURE 1:Hypodense edema in the white matter on the non-contrast axial brain tomography image (A). Hyperintense edema in the white matter of the brain on the axial T2-weighted inversion recovery scan (FLAIR) image (B).
FIGURE 2:The axial (A), coronal (B), and sagittal (C) images of contrast-enhanced T1-weighted magnetic resonance imaging showing the foci of abscesses (tuberculomas) with peripheral enhancement.
The patient was diagnosed with tuberculous meningitis and related intracranial tuberculoma. Quadruple anti-TB therapy was commenced in addition to the administration of dexamethasone and mannitol to control intracranial pressure. Fluid and electrolyte management was also commenced. The lesions exhibited no significant regression following 6 months of therapy. Surgery was performed, and pathological examination confirmed the presence of necrotizing granulomatous inflammation associated with tuberculosis.
Tuberculomas are granulomatous masses arising from the hematogenous spread of M. tuberculosis 1 . These are hallmark features of severe extrapulmonary tuberculosis, present in approximately 5% of all cases of tuberculosis2. Imaging plays a crucial role in the early detection and differentiation of tuberculomas from other intracranial pathologies, thereby facilitating timely intervention and preventing long-term complications3.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Leonard JM Central nervous system tuberculosis Microbiol Spectrum 20175211010.1128/microbiolspec.tnmi 7-0044-2017 PMC 1168748628281443 · doi ↗ · pubmed ↗
- 2Haiga Y Pathogenesis of tuberculous meningitis (TBM): a mini-review IJBS 20221615154
- 3Koesbandono Muljadi R Sutanto R Fransiska SR Takaliuang D Erico A Intracranial tuberculomas: review of MRI findings and clinical features Clin Radiol 20247953543623828671810.1016/j.crad.2023.12.020 · doi ↗ · pubmed ↗